
Abstract
While large language models (LLMs) hold potential for informing prospective trial participants, their deployment raises critical questions regarding patient autonomy and the integrity of informed consent. This paper examines how LLM-mediated communication may influence trial participation decisions. We situate such influence along a continuum from ethically permissible persuasion to impermissible manipulation and coercion, highlighting the concepts of algorithmic nudging and hypernudging. These advanced techniques, capable of adapting messages in real time based on user-specific data, pose unique risks to voluntariness, especially in sensitive contexts such as clinical research. To explore these dynamics, we performed an explorative case analysis based on trial NCT04387916 (KC1036), a phase I oncology study. We prompted ChatGPT-5 to generate three consent texts: a standard informative summary, a strictly neutral version, and a nudged version employing positive framing and collective benefit appeals. We analyzed them against established ethical categories: voluntariness, risks and discomforts, potential benefits, and scientific and social value. The findings exemplify how even minor linguistic variations can introduce normative assumptions and shift the balance between supporting comprehension and exerting undue influence. We conclude that neutrality in LLM outputs cannot be assumed and persuasion cannot be excluded. Without safeguards that explicitly address the design space, LLMs risk transforming informed consent from a protective mechanism into a mere recruitment tool. Safeguarding autonomy in this context requires careful delineation of ethically acceptable influence, critical awareness of the design space of LLM prompts, and alignment with established research ethics principles to ensure that informed consent remains voluntary, informed, and free from hidden persuasion.
Introduction
The principle of informed consent (IC) serves as a bedrock of ethical clinical research, which is essential to respect individuals’ rights to voluntarily decide whether research participation aligns with their interests, including protection from exploitation and harm, and to withdraw at any time without negative consequences (Faden and Beauchamp, 1986; Miller, 2010). This concept has undergone evolution, stemming from a philosophical transition away from paternalistic medical practices toward an ethos centered on patient autonomy (Eyal, 2011; Faden and Beauchamp, 1986). Fundamentally, the IC process provides individuals with the opportunity to comprehend relevant information about the research and to make a voluntary, autonomous decision regarding their participation (Miller and Wertheimer, 2011). Its normative foundations, shaped in response to historical abuses in research, are articulated in the Belmont Report and later codified in international frameworks such as the Declaration of Helsinki (DoH; The National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research (“National Commission”), 1979; WMA Declaration of Helsinki, 2024). In clinical drug trials, IC involves not only written documentation but essentially consists of the conversational process through which participants receive and understand relevant information (Koyfman et al., 2016). Large language models (LLMs) could, in principle, be involved in both components, either by generating written consent materials or by supporting dialogic exchanges, with distinct ethical implications for voluntariness and influence.
Even under extensive regulatory oversight, IC remains difficult to implement effectively. Consent forms have become overly long and complex, often serving institutional and legal interests more than those of participants, and studies show that many participants have limited understanding even after signing (Grady, 2015). The discrepancy between procedural compliance and ethical adequacy has prompted calls for innovative, participant-centered approaches to IC, particularly in light of emerging technologies and AI-driven tools.
While there is no reliable evidence on how LLMs are currently used in consent procedures, such technologies may be applied at several stages of clinical trials, for example, for identifying eligible participants, developing recruitment materials, or supporting certain aspects of the consent process such as record-keeping and communication (Bard, 2023). Recent developments such as TrialGPT demonstrate the accelerating uptake of such tools: in a pilot study, LLM-based systems have reduced patient-trial matching time by over 40%, highlighting both their practical promise and the ethical risks of deploying opaque AI in clinical decision-making, even when these systems are not directly involved in consent communication (Jin et al., 2024). Furthermore, their application is being extended to critical research oversight functions, with recent proposals highlighting the potential of application-specific LLMs to enhance Institutional Review Board (IRB) review processes, including tasks such as pre-review screening and ethical assessment (Porsdam Mann et al., 2025).
Although persuasive capabilities of LLMs have not yet been documented in IC interactions, vendor materials and industry trends suggest that its integration may be imminent, particularly as some sponsors begin participant engagement even before formal trial approval (Cohen, 2020; Koyfman et al., 2016). Prototypes of consent-facilitating LLMs are currently being tested with promising initial results (Aydin et al., 2023). LLMs may also support IC by translating complex trial information into multiple languages with minimal additional effort, potentially improving accessibility for linguistically diverse participant populations (Zhu et al., 2023). As a normative principle, LLMs should not be more persuasive than human counterparts, yet distinguishing ethical persuasion from undue influence in algorithmic outputs remains difficult in practice (Valenti and Giacco, 2022). What feels non-coercive to one participant may feel coercive to another. Measuring LLM-induced coercion is difficult, as enrollment rates are shaped by confounding factors (e.g. recruitment scale, ease of access, staff availability), and participants may not recognize subtle algorithmic influence, that is, the capacity of adaptive AI systems to steer user decisions through personalized framing or data-driven communication patterns (Allen et al., 2025). Although coerciveness in human consent conversations is equally hard to assess, the persuasive intensity of LLMs can be programed, standardized, and monitored through consent transcripts, offering a level of control not feasible in traditional consent processes.
The DoH sets clear ethical standards for research involving human subjects, particularly emphasizing that participation must be voluntary, informed, and free from coercion or undue influence (Art. 25; WMA Declaration of Helsinki, 2024). Personalized communication must not be manipulative; individual tailoring of information must serve comprehension, not persuasion (Art. 26). Any emotional or linguistic pressure that compromises autonomy, especially in vulnerable populations, risks violating the standard of voluntariness (Art. 27, Art. 19). These principles are directly challenged by the rise of LLMs that can be used to adaptively steer decisions. In particular, adaptive language may threaten the integrity of IC if it blurs the line between support and influence.
We aim to address the following central question: How can the design and training of LLMs follow ethical guidelines to adopt context-specific nudging approaches that respect patient autonomy and safeguard participant rights within the complex “design space” of clinical studies? Clinical trials are understood here as drug trials for the sake of conceptual clarity; other types of clinical research, while important, fall outside the scope of our analysis.
The paper begins by outlining traditional ethical challenges of IC in clinical research and examines how LLMs add novel layers of complexity through personalization, adaptivity, and potential influence. We then delineate ethical boundaries between persuasion, nudging, and manipulation and present an explorative case study using LLM-generated consent texts to illustrate these dynamics. We focus on written consent texts rather than dialogic applications, as they remain an ethically and legally binding component of IC in clinical research and thus provide a controlled setting as entry point for normative analysis. Finally, we conclude with reflections on practical and normative implications for the ethically responsible design and governance of LLM-based consent systems.
Challenges in informed consent for clinical research and prospects for the use of LLMs
Despite significant ethical and regulatory advancements, obtaining valid IC in clinical trials remains fraught with persistent challenges that compromise the quality of participants’ decision-making. While these challenges are well documented in research ethics, they acquire renewed relevance in the context of LLMs. We outline five recurring pitfalls to illustrate how the integration of LLMs could either mitigate or exacerbate these longstanding ethical concerns. Identifying these challenges provides the conceptual grounding for our later analysis of LLM-generated consent texts, helping to clarify where algorithmic mediation might reinforce existing weaknesses or introduce new forms of ethical risk.
Therapeutic misconception (TM)
Participants often fail to understand key differences between clinical research and ordinary clinical care, assuming that decisions about their care are being made primarily with their personal benefit in mind (Appelbaum et al., 1982). Hence, they overestimate the likely personal benefits and underestimate the risks of participating in a study, not understanding aspects like randomization or the investigational nature of interventions, especially in the increasingly complex landscape of multi-arm, multi-stage platform trials, as well as umbrella, basket, and adaptive randomization designs (Heynemann et al., 2023). Improved response rates in some phase I cancer trials due to precision medicine make personal benefit expectations more reasonable, reducing the extent of “misconception” in such cases (Heynemann et al., 2024). However, TM is still common, even after thorough IC processes, and it can significantly undermine the quality of a participant’s decision-making and the validity of their consent (Appelbaum et al., 2004).
If LLMs prioritize persuasive communication without clearly distinguishing research from treatment, they risk reinforcing TM. Conversely, if appropriately calibrated, LLMs could assist in mitigating TM by delivering tailored, transparent explanations that clarify the goals of clinical trial research, namely, the generation of generalizable knowledge rather than the provision of individualized care.
Social value misconception (SVM)
This recently discussed misconception involves participants holding false beliefs about a study’s potential benefits for non-participants or its expected social value (Earl et al., 2026). Altruistically motivated individuals, who often enroll in research to advance science or help future participants, may substantially overestimate the impact of their participation. SVM often arises in trials with limited epistemic or therapeutic value, including “me-too” drug studies or overhyped interventions with marginal innovation. When participants enroll on the basis of an inflated sense of social utility, their ability to make decisions aligned with their authentic values is impaired, thereby undermining their autonomy.
LLMs may reinforce SVM if their outputs amplify emotional appeals or emphasize vague promises of social benefit without adequate qualification. Given their capacity to personalize responses based on user preferences and values, LLMs could “play to” altruistic motives by presenting participation as meaningful or noble, even when the underlying trial lacks substantial public health significance. Without clear safeguards, such framing risks crossing the line from participant engagement to subtle manipulation.
At the same time, LLMs could, in principle, help mitigate SVM. When carefully constrained, such systems may support clearer articulation of societal value without implying personal therapeutic gain, though this potential benefit mirrors the same design sensitivities that, if misaligned, risk reinforcing SVM rather than alleviating it.
Comprehension challenges
IC documents are frequently criticized for being too long, complex, and filled with medical jargon, making them difficult for laypeople to understand (Millum and Bromwich, 2021; Paasche-Orlow et al., 2003). Participants often sign or click “Agree” without a second glance, similar to “terms and conditions” documents encountered outside medical contexts (Bakos et al., 2014). While ethical guidelines, such as the DoH, state that “Special attention should be given to the specific information and communication needs of individual potential participants as well as to the methods used to deliver the information,” current practices often fall short (WMA Declaration of Helsinki, 2024).
LLMs potentially offer a promising avenue to address this by personalizing and simplifying complex information (Allen et al., 2025). However, unlike static consent forms or scripted conversations, LLM outputs are unpredictable and adapt dynamically to each participant’s input. This undermines the assumption that all information provided during the consent process can be reviewed and approved in advance, posing a significant regulatory challenge under current frameworks, calling for new oversight mechanisms tailored to AI-mediated communication.
In practice, LLMs could be deployed at different stages of the consent process, ranging from static assistance in drafting written consent materials to interactive chatbot-based systems that allow prospective participants to ask questions in real time. Such systems might operate prior to a participation decision and could, in principle, be integrated with subsequent discussions with human investigators. Personalization could be operationalized through adaptation to user inputs such as literacy level, expressed concerns or prior questions without necessarily relying on sensitive personal data. Although LLMs could be instructed to follow predefined, ethics-approved scripts, their generative nature means that tone, emphasis, and framing may still vary in ways that are difficult to anticipate or fully constrain, distinguishing them from scripted human communication.
Power asymmetries and vulnerability
A significant challenge arises from the strong interest of sponsors and principal investigators (e.g. pharmaceutical companies, trial coordinators) in securing sufficient participation for their trials. In contrast, participants, especially when they are also receiving medical care for their condition, are often in a vulnerable position (Bard, 2023). The persuasive capabilities of LLMs raise concerns about their potential to lead to unintended manipulation or coercion (Allen et al., 2025).
Structural and time constraints
In many settings, researchers face limited time for consent conversations due to overloaded schedules. As a result, consent may be reduced to a procedural formality, rather than a reflective dialog. This is further compounded by structural inequities such as language barriers. Participants may not be fluent in the primary language of the research institution, which can compromise their ability to engage with complex medical information. In such cases, consent quality suffers not because of participant capacity, but due to systemic limitations in communication resources.
LLMs offer promising tools to address some of these structural constraints. Their ability to provide self-paced, on-demand access to information can extend consent conversations beyond the limitations of the clinic schedule. These systems can translate consent materials into participants’ native languages, simplifying complex concepts and offering real-time clarification. This technological capability, however, does not remove the need for human supervision (Allen et al., 2025; Taylor and Bramley, 2012). In fact, their use may paradoxically increase researchers’ workload, especially in large-scale trials since interactions must still be monitored to ensure accuracy, ethical integrity, and legal compliance (Allen et al., 2025).
Forms of influence in informed consent
To assess the risks of LLMs influencing participants’ decisions, we place algorithmic influence within the ethical spectrum of persuasion, manipulation, and coercion. Each represents a distinct form of influence with different implications for autonomy. Persuasion involves a transparent appeal to reasoning, preserving voluntary choice (Botes, 2023; Susser et al., 2018). In the context of IC, the normative aim is not persuasion but the provision of information that enables autonomous, well-informed decision-making. Such information, however, might also serve to de-bias patients in ways that promote their health and related values. When aligned with personal values, this form of communication, known as beneficent persuasion, is usually deemed ethically permissible (Swindell et al., 2010). In IC, beneficent persuasion is ethically permissible only insofar as it remains autonomy-supportive and does not function as advocacy for a particular decision.
In contrast, manipulation operates covertly, exploiting cognitive and emotional vulnerabilities without the subject’s awareness. This subverts autonomy by undermining the participant’s ability to reason clearly (Botes, 2023; Susser et al., 2018). The ethical boundary between autonomy-supportive communication and manipulation rests on transparency, intent, and respect for autonomy, yet it remains unclear when an LLM’s tone or framing crosses this boundary, for example, by selectively presenting information or systematically favoring enrollment. (Zohny et al., 2026).
Coercion and undue influence are prohibited under U.S. regulations like the Common Rule (45 CFR 46) and international frameworks such as the DoH (Bard, 2023; Largent and Fernandez Lynch, 2017). However, these terms lack precise definitions and research ethics committees (RECs) and investigators often lack clear criteria for assessing whether a given form of influence compromises voluntariness in the consent process.
Within this context, the concept of “algorithmic nudging” requires formal clarification. According to Thaler and Sunstein’s behavioral economics, a nudge is any modification of the choice architecture that predictably alters behavior without removing options or changing incentives (Thaler and Sunstein, 2008). Algorithmic nudging, refers to the use of AI systems to personalize and dynamically adapt nudges based on user-specific data. It is more scalable, real-time, and adaptive than traditional nudging but remains largely opaque to end users. Such nudges include recommender systems, personalization engines, and interface design patterns, which influence user behavior without overt awareness. Hypernudging takes thus this to the extreme by continuously adjusting nudges based on behavioral feedback, environmental variables, and population trends (Yeung, 2017). When embedded in LLM-driven consent dialogs, algorithmic and hyper nudging raise concerns about manipulation and undue influence, particularly in high-stakes settings like clinical trials.
Although nudging is not an ethically appropriate goal of IC, it is analytically relevant in the present context because clinical research operates under substantial structural pressures. Empirical research shows that around 80% of trials fail to meet their initial enrollment targets and timelines, and this failure to recruit sufficient participants is the most common reason for premature trial discontinuation, particularly in investigator-initiated trials where scarce human and financial resources and overoptimistic recruitment estimates are pronounced (Briel et al., 2021; Brøgger-Mikkelsen et al., 2020). Given ongoing developments in LLM-based systems for trial matching, it is plausible that similar communicative functions could be extended to consent-related contexts in the future. Our aim is therefore neither to describe current practice nor to frame nudging as an ethical option but to assess, in advance, the concrete character of such uses that might be incompatible with established research ethics standards.
Explorative case study of LLM-generated informed consent in a phase I oncology trial
Building on the preceding ethical framework distinguishing persuasion, manipulation, and coercion, we now examine how LLMs might influence clinical trial participation decisions through consent communication. The analysis is guided by normative principles of autonomy, voluntariness, and transparency, as outlined in the DoH. The aim is not only to tentatively assess ethical alignment of designing LLMs with the DoH, but also to explore the design space for ethically permissible LLM interventions in clinical research settings. By “design space” we mean the full range of possible configurations and communicative strategies that an LLM system could employ. This includes, for example, the tone of the output (neutral vs encouraging), the degree of personalization (generic vs user-specific phrasing), and the extent to which the system subtly guides user choices (autonomy-supportive vs persuasive). Newer LLM training methods, in particular Reinforcement Learning from Human Feedback (RLHF), optimize models to generate responses that satisfy users, which can tend to lead them to use affirmative or agreeable formulations (Ouyang et al., 2022). Investigating the design space helps identifying forms of LLM communication that, from a research ethics perspective, support participant autonomy and informed decision-making or risk crossing ethical boundaries.
Trial selection
To simulate a realistic use case, we selected a first-in-human phase I dose-escalation study titled “A Study of KC1036 in Patients With Advanced Solid Tumors” (ClinicalTrials.gov Identifier: NCT04387916). This study involves the administration of KC1036, a multi-kinase inhibitor, to patients with advanced-stage cancer. Phase I trials are characterized by significant uncertainties regarding safety and efficacy, and offer minimal direct benefit to individual participants while aiming to generate knowledge of broader societal value. This makes such trials ethically sensitive as severely ill patients often perceive participation as a last therapeutic opportunity which can make them vulnerable to persuasion and necessitates additional support in decision-making. These features render the trial ethically salient for evaluating the limits of persuasive communication in IC processes, particularly when mediated by LLMs.
The purpose of this simulation is illustrative rather than experimental. It demonstrates, through a single case example, how specific prompting instructions can produce different framings of consent-relevant information. The broader contribution of this article is normative. It analyzes why such variations in framing matter ethically for IC and considers their implications for the governance of LLM-generated consent communication.
LLM-generated consent texts
On 18 August 2025, we instructed ChatGPT-5 to generate IC summaries for the Phase I trial NCT04387916 (KC1036). To explore how small shifts in framing can affect ethically significant aspects of consent communication, we designed three distinct prompt conditions. The full prompts are provided in the Supplemental Material. This tripartite design was chosen to capture a minimal but illustrative spectrum: a standard version (ChatGPT-5’s standard style), a neutral version (strictly descriptive, avoiding affective or value-laden language), and a nudged version (subtly encouraging participation through positive framing, collective benefit, and altruistic meaning). Representative excerpts are reproduced verbatim in Table 1. We deliberately focus on non-personalized written consent texts rather than real-time dialogic systems. Written consent materials remain a legally and ethically binding component of IC and provide a controlled setting in which to isolate how prompt-level framing alone can shift ethical properties of disclosure, independent of interpersonal dynamics or user-specific tailoring.
Representative excerpts from standard, neutral, and nudged LLM-generated informed consent texts.
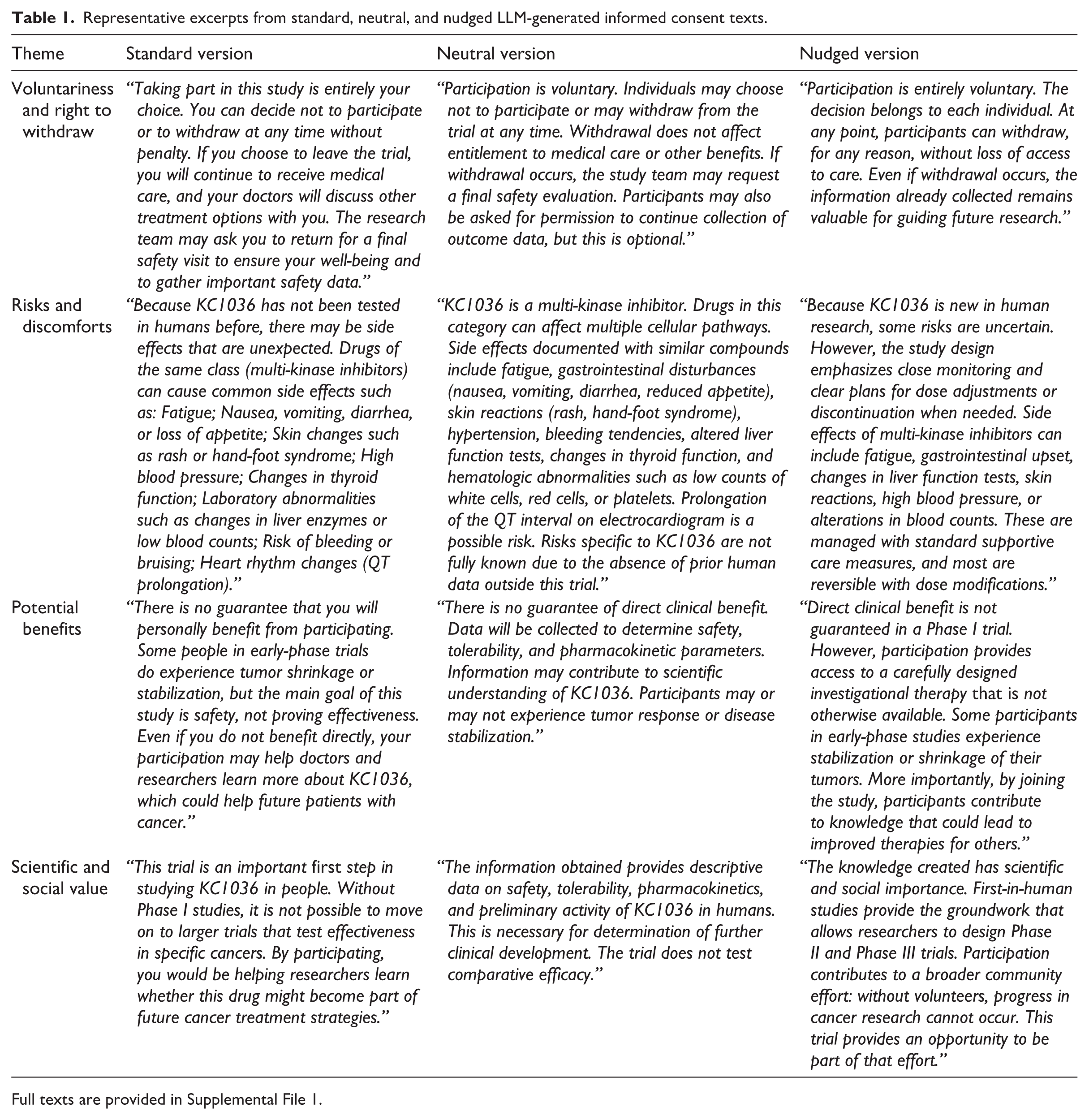
Full texts are provided in Supplemental File 1.
The simulation was conducted using ChatGPT-5 via the standard interface. For each prompt condition (standard, neutral, and nudged), a single output was generated and analyzed. Systematic evaluation of variability across multiple generations and model configurations was not performed due to merely illustrative character of the simulation.
While some authors argue that nudging is incompatible with genuine IC, others note that certain forms of influence may be unavoidable in practice and propose reflexive strategies, such as meta-nudges, to mitigate their ethical impact, and empirical studies suggest that recruitment practices already involve framing techniques (e.g. “sandwiching” risks between two benefits) that function as nudges, often without being explicitly labeled as such (Gelfand, 2023; Simkulet, 2019; Volkmar et al., 2025). In the context of IC, the ethical aim is not to steer participants toward or away from enrollment, but to support autonomous, well-informed decision-making. Nudging is therefore not introduced here as a permissible goal of consent design. Rather, it serves as an analytical category to examine forms of influence that may arise in practice, including unintentionally, through framing, tone, or emphasis. This is particularly relevant for LLM-mediated communication, where subtle prompt choices can systematically shape outputs at scale. By analyzing nudging as a boundary case, we aim to clarify where consent communication risks shifting from autonomy-supportive information provision toward ethically problematic influence.
Ethical analysis of LLM-generated consent text
The generated texts were examined against established ethical criteria relevant to IC, including voluntariness, risks and discomforts, potential benefits, and scientific and social value. These categories reflect core elements of research ethics frameworks such as the DoH and widely used bioethical analyses of IC. The analysis therefore focuses on how different prompting conditions shape ethically relevant features of consent communication, including the presentation of risks, the framing of potential benefits and the degree to which the communication supports voluntary decision-making.
The comparison between the three consent versions shows how small linguistic shifts can reshape the ethical implications of IC while engaging the obligations articulated in the DoH. At the core of the DoH is the requirement that participation should be voluntary, well informed, and free from coercion or undue influence (WMA Declaration of Helsinki, 2024). The excerpts on voluntariness and the right to withdraw illustrate the clearest contrasts. The neutral version is strictly descriptive, stating that participation is voluntary and that withdrawal will not affect ongoing care. The standard version communicates the same right in a more patient facing manner, assuring continued access to care and a safety follow up, which may promote trust without directing the decision. Notably, the standard and neutral versions also display autonomy-supportive features, including clear articulation of the right to withdraw, structured presentation of risks, and the absence of explicit value-laden appeals, which can be understood as forms of autonomy scaffolding rather than persuasion, insofar as they support participants’ capacity to make reflective decisions without steering their choice direction (Allen et al., 2026). The nudged version also affirms voluntariness, yet it embeds withdrawal in a collective frame, noting that “the information already collected remains valuable for guiding future research.” That sentence misattributed social value to any degree of participation, including partial participation. Although not coercive, it places the decision in a morally colored context that can shape preferences at the margin. This framing creates tension with the DoH’s insistence that the participant’s welfare and autonomous choice take precedence over scientific aims and societal goals.
The ability of LLMs to generate outputs steered toward a particular dimension such as emphasizing altruistic or collective framing is technically feasible through methods like preference-based activation steering, where lightweight steering vectors are injected during inference to guide the LLM’s output in the direction of a desirable concept (Bo et al., 2025). This steering provides finer control over the LLM’s output than natural language prompting alone.
The treatment of risk reinforces the concern about framing. The neutral version lists potential harms in precise technical terms and foregrounds uncertainty that is intrinsic to a first-in-human trial, including the possibility of serious or life-threatening toxicities. The standard version conveys essentially the same content, while describing monitoring as responsive and protective, which softens tone but preserves balance between sincerity and reassurance. The nudged version shifts emphasis toward monitoring intensity, reversibility of adverse effects, and the manageability of toxicities, thereby moving the attention from the magnitude and unpredictability of harms to the promise of control. Notably, the nudged version omits explicit mention of bleeding and QT prolongation, both of which are included in the standard and neutral versions and constitute among the more serious risks of participation. This omission is ethically and legally important, as such risks would plausibly qualify as material under standards articulated in Montgomery v Lanarkshire, a clinical care case whose patient-centered disclosure standard is widely regarded as normatively relevant to research consent, according to which disclosure must include risks that a reasonable person in the participant’s position would likely consider significant (Montgomery v Lanarkshire Health Board, 2015). The absence of these risks illustrates how LLM-mediated framing and selection effects can undermine adequate risk disclosure, even without overtly coercive language.
A proper recognition of this deliberate framing is critically important, for example, because surrogate decision-makers who perceived a higher risk of participation were significantly less likely to enroll the patient (Krutsinger et al., 2020). Therefore, framing risks in a way that predictably compresses perceived risk constitutes an ethical threat. The goal of behavioral nudges in the trial recruitment context is to rebalance illegitimate influences acting against enrollment without causing undue inducement. However, the DoH requires transparent and balanced disclosure of potential risks. When salience is placed on control and reversibility, patients may rationally infer that serious outcomes are unlikely, which undermines adequate understanding even if no statement is false.
The handling of potential benefits shows a parallel dynamic. The DoH warns against overstating benefits in early phase studies, where therapeutic intent is secondary to dose finding and safety. The neutral version adheres closely to this constraint, denying any guarantee of benefit and locating the value of enrollment in the production of reliable data. The standard version remains cautious yet accessible, acknowledging that some individuals in comparable trials have experienced tumor shrinkage and reiterating that safety is the primary aim. The nudged version goes further by presenting access to the investigational agent as a meaningful opportunity and by coupling the remote possibility of tumor control with an appeal to altruism and future patients. The nudged version places greater emphasis on possible tumor stabilization or shrinkage without reiterating that efficacy is not the study’s objective. This asymmetry increases the risk of therapeutic misconception, insofar as participants may misinterpret the trial’s primary purpose as therapeutic rather than knowledge-generating. The rhetoric of contributing to progress introduces an implicit incentive structure, shifting the choice from a personal clinical decision to a socially valorized act. This strategy employs behavioral economic concepts known as social norms and the duty of reciprocity to encourage participation, leveraging the sense that one should repeat prosocial behavior or that others approve of the action (Karthic et al., 2023). This value laden framing risks moving consent away from the voluntariness protected by the DoH, which requires decisions that are free from undue influence.
The final contrast concerns scientific and social value where the neutral version states that the study will yield descriptive data necessary for further clinical development. The standard version explains that Phase I trials are prerequisite steps before larger efficacy studies and acknowledges that participants make those steps possible. The nudged version amplifies the collective frame, characterizing enrollment as a broader community effort and invoking progress that cannot occur without volunteers. The DoH recognizes that social value justifies exposing participants to some risk, yet it also requires that the interests of the research subject prevail over those of science and society.
When collective benefit is repeatedly foregrounded, the rhetorical balance can tilt toward subordinating autonomy in practice, even if formal rights are preserved. While behavioral economics strategies like altruism have been tested in a randomized controlled trial for recruitment (in a pediatric trial on postoperative pain relief), the study found no statistically significant increase in the primary outcome of patients’ intentions to enroll into the trial (Karthic et al., 2023). However, it did find that the behavioral economics-informed video made participants less likely to perceive the therapy as being risky.
Beyond these rhetorical distinctions, the comparison reveals structural risks in how LLMs mediate research communication. One might argue that instructing an LLM to generate “neutral” consent text offers a simple solution to ethical concerns. Yet this assumption overlooks the opacity of LLM behavior and the practical realities of prompt use in clinical environments. In practice, research institutions rarely formulate prompts with neutrality as their explicit goal. Instead, objectives are often framed in terms of enhancing recruitment or improving engagement. Such goals, even if well-intentioned, embed subtle normative value orientations into the communicative process. Our simulation makes these dynamics visible by showing how seemingly minor linguistic shifts without any malicious intent can alter the ethical meaning of IC in ways that are not easily perceived by neither researchers nor participants.
This raises deeper normative questions that extend beyond the dualism of “neutral versus nudging.” At what point does tone cross the boundary from informative to persuasive? How can the shift from presenting risks and benefits to subtly steering choices be reliably detected and regulated? Empirical evidence shows that GPT-4’s persuasive success in structured debates with human participants increased by 81.7% when it had access to personal information about its interlocutor (Salvi et al., 2024). This confirms the concern that LLMs can exploit personal data to create hyper-tailored arguments (personalized persuasion) that effectively manipulate opinions. Although our simulation does not implement personalization, it reveals a baseline ethical vulnerability: even minimal prompt-induced framing in non-personalized consent texts can influence how information is normatively interpreted. Personalization and real-time interaction would be expected to intensify this effect by making such framing more targeted and salient, rather than introducing a fundamentally different ethical mechanism. Without such conceptual clarity, the line between ethically permissible explanation and ethically problematic influence remains blurred, undermining the DoH’s demand that voluntariness be free from undue influence.
With regard to model’s training and optimization, most contemporary LLMs are fine-tuned using human feedback toward alignment criteria that emphasize being helpful, honest (or truthful), and harmless (Ouyang et al., 2022). While these qualities may appear beneficial, they also predispose outputs toward confirmatory or affectively colored language. Our results underscore why this default orientation matters ethically: it introduces subtle persuasion into contexts where neutrality is essential when communicating material risks and the non-therapeutic aims of early-phase trials. In our case study, the neutral and standard consent texts explicitly listed serious risks such as bleeding and QT prolongation, whereas the nudged version omitted these risks while emphasizing collective benefit, illustrating how even subtle persuasive framing can alter participants’ interpretation of material information. This suggests that ethical evaluation cannot focus solely on prompt content, but must also consider model architecture and training objectives as part of the design space in which IC communication takes place.
The importance of making the design space explicit is underscored by the rapid integration of LLMs into clinical trial pipelines. Systems such as CohortGPT and TrialGPT already demonstrate how patient classification and trial matching can be automated, reducing expert screening time and embedding LLMs into recruitment processes (Guan et al., 2023; Jin et al., 2024). These systems, however, operate at the level of backend trial infrastructure and are not designed to generate or mediate IC communication. This trajectory extends to IC itself. LLMs can generate key information sections of IC forms that are as accurate and complete as human-written text, while markedly outperforming them in readability, understandability, and actionability (Shi et al., 2025). Similarly, GPT-4 can generate patient-friendly summaries and question–answer sets that improved comprehension and interest, although hallucinations remain a risk when source material is incomplete (Gao et al., 2025). Together, these developments confirm that LLM-mediated consent communication is not speculative but imminent. This makes the ethical evaluation of tone, framing, and neutrality not a theoretical exercise but a practical requirement for safeguarding voluntariness in trial participation. Human investigators also convey tone in consent conversations, and such tonal cues inevitably shape participants’ interpretations. The ethical concern with LLM-mediated consent is therefore not the presence of tone as such, but its institutional embedding. This means that clinicians are bound by professional duties to act in the participant’s interests and operate within identifiable accountability structures, whereas LLM outputs are shaped by training data, alignment objectives, and prompts that may prioritize engagement or sponsor-defined goals over participant autonomy. Moreover, while an overly persuasive clinician affects a limited number of individuals and can be supervised or corrected, an LLM-based consent system can deploy the same subtle framing at scale across thousands of participants, increasing the risk of systematic and less visible distortion of voluntariness.
The comparative table demonstrates that even small prompt-induced differences can recalibrate the ethical status of consent, often in ways invisible to participants. These prompts were deliberately designed to represent distinct communicative personae of the LLM neutral, standard, and nudging in order to capture how minor framing choices may ethically reorient participant understanding. This finding is significant because real-world deployments rarely guarantee full transparency or control over prompt design. This implicates: without safeguards that explicitly address the design space, LLMs risk turning IC from a protective mechanism into a recruitment tool. Taken together, the three versions show that tone, without changing facts, can reconfigure the ethical meaning of consent. The neutral version aligns most closely with the DoH’s demands for clarity, transparency, and absence of undue influence, the standard version balances accessibility with those demands, and the nudged version, while factual, introduces subtle pressures that approach the boundary the DoH is meant to defend.
Future research should complement this normative analysis with empirical investigations examining how different stakeholders, including clinicians, research coordinators, ethics review boards and prospective participants evaluate LLM-generated consent texts. Such studies could also assess readability, comprehension and perceived autonomy support across different prompting strategies.
Conclusion
Our explorative case study shows that subtle linguistic variations in LLM-generated consent can shift ethical boundaries, influencing how participants perceive risk, benefit, and autonomy. While LLMs may improve trial accessibility and efficiency, they also introduce risks of unintentional persuasion and opacity in decision-making. Ethically responsible use therefore requires operational safeguards that emphasize neutrality, explicitly present non-participation as a valid option, and acknowledge uncertainty. Future LLM design for IC should adopt neutrality as the default communicative mode, with transparent supervision and prompt control to ensure that autonomy, not recruitment, remains the guiding principle, while clarifying the ethical design space for permissible interventions.
Concretely, we propose the following: (1) neutrality should be set as the default communicative mode in consent generation; (2) prompt governance should be formalized, with recruitment-oriented framing explicitly prohibited; (3) model tuning requires independent scrutiny to prevent drift into motivational or moralized language; (4) transparency and auditability must be ensured, with RECs requiring documentation of prompts, outputs, and safeguards; and (5) the design space of permissible interventions should be explicitly mapped. Together, these recommendations stress that the ethical promise of LLMs in clinical trial recruitment lies not in their ability to persuade but in their ability to sustain truly autonomous and informed decision-making provided that humans carefully design and oversee their deployment. While we argue that neutrality should serve as the default communicative mode for LLM-generated consent materials, our exploratory analysis does not demonstrate that neutral prompts cannot produce ethically problematic outputs. Establishing this would require systematic testing across a wider range of prompts and model settings. Future research should empirically examine how LLM-mediated consent compares with traditional human-led consent processes, particularly with respect to participant understanding, perceived voluntariness, and susceptibility to nudging. Comparative studies assessing participant feedback on human versus AI-supported consent, as well as observational analyses of recruitment practices under different consent modalities would help clarify when and how LLMs may responsibly augment, rather than undermine, IC in clinical research.
Supplemental Material
sj-docx-1-rea-10.1177_17470161261451591 – Supplemental material for Algorithmic nudging for clinical trial participation: Autonomy and consent in the era of large language models
Supplemental material, sj-docx-1-rea-10.1177_17470161261451591 for Algorithmic nudging for clinical trial participation: Autonomy and consent in the era of large language models by Pranab Rudra, Wolf-Tilo Balke, Tim Kacprowski, Frank Ursin and Sabine Salloch in Research Ethics
Footnotes
Author contributions
All authors contributed substantially to the manuscript via writing, reviewing and editing
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.