
Abstract
Egocentric (subject-to-object) and allocentric (object-to-object) spatial reference frames are fundamental for representing the position of objects or places around us. The literature on spatial cognition in blind people has shown that lack of vision may limit the ability to represent spatial information in an allocentric rather than egocentric way. Furthermore, much research with sighted individuals has reported that ageing has a negative impact on spatial memory. However, as far as we know, no study has assessed how ageing may affect the processing of spatial reference frames in individuals with different degrees of visual experience. To fill this gap, here we report data from a cross-sectional study in which a large sample of young and elderly participants (160 participants in total) who were congenitally blind (long-term visual deprivation), adventitiously blind (late onset of blindness), blindfolded sighted (short-term visual deprivation) and sighted (full visual availability) performed a spatial memory task that required egocentric/allocentric distance judgements with regard to memorised stimuli. The results showed that egocentric judgements were better than allocentric ones and above all that the ability to process allocentric information was influenced by both age and visual status. Specifically, the allocentric judgements of congenitally blind elderly participants were worse than those of all other groups. These findings suggest that ageing and congenital blindness can contribute to the worsening of the ability to represent spatial relationships between external, non-body-centred anchor points.
Keywords
Introduction
According to a global estimate of the visually impaired population by the World Health Organisation (WHO), people aged 50 years and above represent 82% of the entire blind community (Pascolini & Mariotti, 2012). Research has shown that age-related cognitive decline can lead to difficulties in daily life activities, such as locating spatial positions or wayfinding (Colombo et al., 2017; Lester et al., 2017; K. Z. Li et al., 2001; Moffat, 2009) with consequent reduced mobility in the visually impaired elderly compared to the normally sighted elderly (e.g., Wilkie et al., 2006). A decrease in mobility has indeed been observed in elderly blind individuals (e.g., Mac Cobb, 2013). Therefore, it is important to understand the impact of ageing on spatial memory abilities in blind individuals as maintaining these fundamental abilities may be more crucial in blind elderly people than in normally sighted elderly people (e.g., Heyl & Wahl, 2012; Pigeon & Marin-Lamellet, 2017).
Long-standing research in spatial memory has demonstrated that external positions can be encoded according to egocentric (subject-to-object) and allocentric (object-to-object) spatial frames of reference (Burgess, 2006; O’Keefe & Nadel, 1978; Paillard, 1991). Neurofunctional studies have reported the activation of the posterior parietal/frontal network in egocentric processes and posteromedial and medio-temporal substructures in allocentric processes (e.g., Galati et al., 2010; Moffat, 2009; Ruotolo et al., 2019).
Separate lines of research have shown that the capacity to process egocentric and allocentric spatial representations can be reduced to different degrees in people with visual impairments (Cattaneo et al., 2008; Pasqualotto & Proulx, 2012; Schmidt et al., 2013; Tinti et al., 2006) and in healthy and pathological ageing (e.g., Caffò et al., 2020; Colombo et al., 2017; Iachini, Ruggiero, & Ruotolo, 2009; Lopez et al., 2019; Moffat, 2009; Ruggiero et al., 2016; Ruggiero, Iavarone, & Iachini, 2018; S. Serino et al., 2014).
Blindness and reference frames
Regarding blindness, much research has demonstrated a link between the dominant perceptual modality and the processing of reference frames. In the absence of visual experience, non-visual perceptual modalities, such as proprioceptive, haptic, and kinesthetic modalities, are preferably organised in relation to egocentric frames of reference (Cattaneo et al., 2008; Noordzij et al., 2006; Pasqualotto & Proulx, 2012; Pazzaglia & De Beni, 2001; Ruggiero, Ruotolo, & Iachini, 2018; Schmidt et al., 2013; Steyvers & Kooijman, 2009; Thinus-Blanc & Gaunet, 1997). The term “haptic” indicates that cutaneous, proprioceptive, and kinesthetic inputs work together to encode information (see Millar, 1994; Révész, 1950). Therefore, the main flow of information relies on a spatio-temporal sequence of stimuli anchored on the body (Arbib, 1991; Millar, 1994). As a consequence of this piecemeal exploratory strategy, blind people meet difficulties in holistically organising haptic stimuli (Cheryl Kamei, 2006; Cornoldi & Vecchi, 2004; Millar, 1994). This difficulty may lead to a specific allocentric limitation. In fact, several studies have shown that the capacity to process spatial information according to egocentric frames is similar in congenitally (blind from birth) and adventitiously (late onset of blindness) blind people compared to sighted people (e.g., Bigelow, 1996; Millar, 1994; Morrongiello et al., 1995; Noordzij et al., 2006; Postma et al., 2008; Tinti et al., 2006; Vecchi et al., 2004). In contrast, the processing of allocentric spatial information appears to be more difficult for the congenitally blind than for the adventitiously blind and the sighted (Cornoldi & Vecchi, 2004; Iachini et al., 2014; Merabet & Pascual-Leone, 2010; Noordzij et al., 2006; Pasqualotto & Proulx, 2012; Ruggiero et al., 2009, 2012; Schmidt et al., 2013; Vecchi, 1998; Vecchi et al., 2004). Much research has suggested that the absence of any visual experience may limit the ability to process efficient allocentric representations (but see Landau et al., 1981; Loomis et al., 1993; Passini et al., 1990; Postma et al., 2007). For example, Pasqualotto et al. (2013) have demonstrated that people who can rely on visual experience even if visual information is inhibited, such as the blindfolded sighted and the late blind, tend to use allocentric frames to represent spatial information, while the congenitally blind people prefer body-based egocentric frames of reference. The egocentric preference could be due to the lack of experience with the visual modality, i.e., the modality that allows the simultaneous representation of relative positions between different objects in a spatial configuration. This is coherent with the idea that visual information is fundamental in the setting up of the cerebral structures underlying these spatial functions, especially the allocentric ones (Cattaneo et al., 2008; Iachini & Ruggiero, 2010; Leporé et al., 2009; Maurer et al., 2005; Ruotolo et al., 2012).
Although the exact neural mechanisms underpinning cross-modal plasticity and behavioural compensation strategies in blindness need to be further elucidated (Merabet & Pascual-Leone, 2010), several Transcranial magnetic stimulation (TMS), functional imaging, and lesion studies have documented that early vision loss may result in massive cross-modal functional reorganisation, with the deprived visual cortex being activated by inputs from other sensory modalities (e.g., Amedi et al., 2003; Collignon et al., 2007; Raz et al., 2005). In particular, research investigating the impact of different levels of visual experience has found functional and structural differences in brain areas involved in spatial processing (especially the hippocampus and the posterior parietal cortex) that could explain behavioural differences between individuals (see Chebat et al., 2007; Leporé et al., 2009; but see Fortin et al., 2008). For example, differences in activation of the posterior parahippocampus, posterior parietal, and ventromedial occipito-temporal cortices were observed in congenitally blind as compared to sighted participants during mental navigation (Kupers et al., 2010; Merabet & Pascual-Leone, 2010). The cerebral plasticity of the visual cortex may mediate several abilities, such as Braille reading, spatial and episodic memory tasks, imagery processes, spatial discrimination, working memory, and spatial navigation (for reviews, see Merabet & Pascual-Leone, 2010; Noppeney, 2007). With regard to late blindness, the loss of vision after the age of 10–16 years represents a critical period. The late onset of blindness causes a functional shift in the striate cortex from processing visual stimuli to processing tactile and linguistic stimuli (L. G. Cohen et al., 1999; Sadato et al., 2002; see also Ofan & Zohary, 2007).
There is also evidence that when spatial information is encoded in small-scale space compared to large-scale space, differences between the spatial performance of sighted and blind individuals are attenuated (Iachini et al., 2014). The distinction between small- and large-scale spaces is based on the classical literature on spatial cognition (Acredolo, 1981; Rieser et al., 1992; Siegel, 1981; Thinus-Blanc & Gaunet, 1997; Weatherford, 1985). The small-scale spaces do not enclose the observer and can be apprehended with a single glance. Large-scale spaces require the movement of the observer’s whole body to explore because they can only be perceived in segments. Therefore, blind people can use haptic exploration with the body that provides a stable egocentric frame to learn spatial information in small-scale spaces; instead, in large-scale spaces they have to move with the whole body through the space to explore objects sequentially (Acredolo, 1981; Siegel, 1981; Weatherford, 1985). This distinction is akin to that between peripersonal and extrapersonal space. Indeed, the peripersonal space refers to the reaching portion of space where action is possible in the here and now (Berti & Frassinetti, 2000; Rizzolatti et al., 1987; for a review, see A. Serino, 2019). In contrast, extrapersonal space is the far area beyond the reach of our limbs where we cannot act directly (e.g., Bartolo et al., 2014; Ruggiero et al., 2020). For example, Hollins and Kelley (1988) reported that in a small-scale setting, blind individuals performed similarly to sighted blindfolded individuals in a spatial relocation task. Similar results were achieved by Coluccia and colleagues (2009) by means of an object location memory task. In contrast, Ruggiero et al. (2012) demonstrated that congenitally blind individuals performed worse than sighted, blindfolded sighted, and adventitiously blind participants in processing allocentric metric representations and in switching from allocentric to egocentric encodings (Ruggiero, Ruotolo, & Iachini, 2018). Iachini et al. (2014) explored whether the ability to represent spatial frames of reference in people with different degrees of visual experience was mediated by the scales of space and exploratory modalities: large-scale space (haptic + locomotor exploration) versus small-scale space (haptic exploration). They found that early blind compared to late blind and sighted participants had difficulty in representing allocentric information, especially in large-scale space. An allocentric difficulty in congenitally blind participants, probably due to a limitation in spatial updating processes, was also demonstrated in small-scale spaces by Pasqualotto and Newell (2007). On the whole, findings are not yet fully convergent.
Ageing and reference frames
With regard to the effect of ageing on the spatial memory of healthy sighted individuals, research has reported a detrimental impact on egocentric and, above all, allocentric spatial representations. Typically, normal age-related decline is ascribed to functional changes in the posteromedial, medio-temporal, and frontal areas (Klencklen et al., 2012; A. W. Li & King, 2019; Moffat, 2009). Studies have generally shown poorer allocentric performance of elderly people as compared to young people in memorising unfamiliar environments (Kirasic, 1991; Wilkniss et al., 1997) and orienting themselves in simulated navigation spaces (Iaria et al., 2009; Jansen et al., 2010; Picucci et al., 2009; Rodgers et al., 2012; for reviews, see Klencklen et al., 2012; A. W. Li & King, 2019; Moffat, 2009). Research has also shown a difficulty of elderly people in performing spatial tasks that require egocentric encodings, such as route learning in complex real or virtual settings (Wiener et al., 2012; Wilkniss et al., 1997), localising positions (Ruggiero et al., 2009, 2012, 2016), integrating positions or working out routes (Moffat et al., 2001), recalling the temporal order of landmarks, and directional information (Eichenbaum et al., 2007; Head & Isom, 2010). Literature has shown that ageing negatively affects navigation ability and spatial location memory (e.g., Lester et al., 2017; Moffat, 2009; Wolbers et al., 2014). For example, elderly people have difficulties with allocentric navigation tasks (Head & Isom, 2010; Iaria et al., 2009) and prefer egocentric navigation strategies (Rodgers et al., 2012), even though these strategies are maladaptive by producing navigation errors (Wiener et al., 2013). In addition, navigation strategies also with age change with respect to the type of spatial information to be processed and the characteristics of the environment (see Lester et al., 2017). Segen et al. (2021), for example, found that elderly people preferred to encode object positions by exploiting room-based cues, whereas younger adults tended to encode spatial relationships between objects. Bécu et al. (2019) demonstrated that the ability to combine landmark and geometric cues is negatively impacted by ageing, with elderly adults preferring geometrical ones during navigation. Furthermore, elderly people also have difficulties in switching between spatial reference frames and in changes of cue or task demand (Harris et al., 2012; Harris & Wolbers, 2012, 2014; but see Ruggiero, Iavarone, & Iachini, 2018; Ruggiero, Ruotolo, & Iachini, 2018 for object location memory).
Overview of the study
In sum, during ageing, the process of normal decline in the functions of the medio-temporal lobe causes difficulty mainly in the use of allocentric representations (e.g., Colombo et al., 2017; Lester et al., 2017; Moffat, 2009). However, research on blind people has shown functional and structural differences in brain areas involved in spatial processing (especially the hippocampus and the PPC) compared to sighted people, which could explain the difficulty of early blind people in processing allocentric rather than egocentric spatial representations (e.g., Cattaneo et al., 2008). Therefore, it would be important to understand the combined effect of ageing and blindness on the ability to encode egocentric and allocentric spatial representations. This would allow us to clarify a double issue: on the one hand, the weight of visual resources on spatial information processing in a life course perspective; on the other hand, whether the compensatory capacity in blind people is affected by the age-related decline we usually observe in spatial cognition (Wittich et al., 2019).
To address these issues, we compared young and elderly participants with different degrees of visual experience on a spatial memory task: congenitally blind (blind from birth), adventitiously blind (late onset of blindness), blindfolded sighted (short-term visual deprivation), and sighted (full visual availability). The task required egocentric/allocentric verbal judgements of relative distances between memorised stimuli (Iachini et al., 2014; Iachini & Ruggiero, 2006; Ruggiero et al., 2016) after haptic (blind and blindfolded sighted people) and visual (sighted people) exploration of spatial arrays presented in participants’ reachable space. The congenitally and adventitiously blind individuals were compared to understand whether specific limitations are linked to the early onset of blindness. The blindfolded sighted group was included to distinguish the weight of the explorative modalities (tactile sequential of the blind group vs simultaneous vision of the sighted group) and the lack of visual information (short term of the blindfolded participants vs long term of the blind participants). The experimental paradigm was based on previous studies involving different populations (healthy individuals, Ruggiero et al., 2016, 2021; Ruotolo et al., 2015; neurological patients, Iachini, Ruggiero, Conson, et al., 2009; Ruggiero et al., 2020; Ruggiero, Iavarone, & Iachini, 2018; blind people, Iachini et al., 2014; Ruggiero et al., 2009, 2012; Ruggiero, Ruotolo, & Iachini, 2018), which demonstrated its efficacy in inducing the specific involvement of spatial reference frames.
Response time (RT, s) and accuracy measured the performance. RT analysis could provide us with further information on cognitive load in performing memory-based localisation tasks in populations with different levels of visual experience. Considering the decline due to ageing and the limitations linked to the absence of vision, we expected a difficulty in processing allocentric more than egocentric representations in elderly and blind people. In particular, this disruptive effect should be exacerbated in congenitally blind elderly participants who should perform worse than other groups independently of their age and visual status. As regards adventitiously blind people, we cannot put forward precise hypotheses, although in the literature their spatial performance is often in between that of congenitally blind and sighted people (Cattaneo et al., 2008; Millar, 1994). Finally, considering that we adopted a small-scale setting, we expected the eight groups to perform similarly in processing egocentric spatial information. These hypotheses should be verified by a significant interaction between groups and reference frames.
Material and method
Participants
A total of 160 participants, 72 females, took part in the experiment. On the basis of their age and degree of visual experience, they were assigned to 8 groups (20 participants for each group) as follows: young and old congenitally blind, adventitiously blind, blindfolded sighted and sighted adults. The number of males and females within each age group was balanced (see Table 1).
Age and sex distributions for the different groups of participants. Onset of blindness for blind groups.

C Blind: congenitally blind; A Blind: adventitiously blind; B Sighted: blindfolded sighted.
The sample size was determined with the software G*power 3.1.9.2 (Faul et al., 2009). With an α = .05, a Power (1 − β) = .80, eight groups of participants, and two repeated measures (correlations among measures = .20), results showed that 152 participants were sufficient to detect an effect size, Cohen’s f = .20. According to J. Cohen’s (1962, 1988) two large replication studies of published findings (i.e., Camerer et al., 2018; Open Science Collaboration, 2015) and meta-analyses (Bosco et al., 2015; Gignac & Szodorai, 2016; Stanley et al., 2018; for a review article, see Brysbaert, 2019), a Cohen’s f = .20 represents a reasonable estimate of a theoretically meaningful effect size. Furthermore, the correlation between repeated measures was calculated on the basis of previous studies (Iachini et al., 2014; Ruggiero et al., 2016). The total final sample was 160 participants (i.e., 20 per group).
As for sex effects, the Chi-square test showed that females and males were equally distributed in the eight groups: χ2(7) = 2.42, p = .93. No age differences were found between the young groups, F(3, 76) = 1.260, p = .29, on the one hand, and between the elderly groups, F(3, 76) = 1.110, p = .35, on the other hand. Sighted and blindfolded sighted participants were matched to blind persons in terms of sex and age (see Table 1 for details). Congenital and adventitious participants were totally blind and were enrolled with the help of the UIC (Association of Italian blind people) located in Naples and Caserta (Italy) and surrounding areas. Congenital participants were blind from birth. Adventitious participants became blind later in life (at least after the age of 10 years, mean age of onset of blindness = 15.3 years, SD = 3.9, range = 10–27 years). Blindness was due to the following aetiologies: congenital retinitis pigmentosa, optic nerve atrophy, and congenital glaucoma. All visually impaired individuals provided for their daily needs without the need for assistance were active and well integrated in their community. They were recruited on the basis of the following criteria: (1) visual handicap was never associated with central nervous system dysfunctions and/or psychiatric disorders; (2) they were able to move independently in their community (by walking with a white cane/led by dogs, by public transportation or both) and received formal orientation and mobility (O&M) training; (3) they had at least 13 years of formal education; and (4) none reported a cognitive deficit assessed by their own general practitioner or by the UIC neurologist of reference (Naples and Caserta, Italy) through semi-structured clinical interviews following the MoCa protocol for blind people (Wittich et al., 2010). Older sighted people included in the sample had a mini mental state examination (MMSE) score of at least 28. Sighted participants were enrolled from public places through advertisements and by word of mouth. They were randomly assigned to the groups called “Sighted” and “Blindfolded Sighted” and matched for sex and age. All sighted participants had normal or corrected-to-normal vision. All participants were free from neurological and psychiatric disorders. With regard to congenitally blind participants with optic nerve atrophy, there was no presence of other comorbid neurological diseases. All participants gave written consent before taking part in the study. The study was approved by the Research Ethics Board of the Department of Psychology (Vanvitelli University) and was conform to the ethical principles of the Helsinki Declaration (2013).
Setting
The experiment took place in the Laboratory of Cognitive Science and Immersive Virtual Reality (CS-IVR) of the Department of Psychology (University of Campania L. Vanvitelli, Italy) and the UIC of Naples and Caserta (Italy). The experiment was carried out in soundproofed rooms where there was only a small table supporting the panels in front of a blank wall. In this way, sighted groups could only focus on the table and one triad at a time, and all groups were not disturbed by unwanted noise.
Stimuli
The stimuli comprised 12 well-known 3D geometrical objects (pyramid, parallelepiped, cone, cube, sphere, and cylinder) of small and big sizes. The objects had bases of the same dimensions, i.e., the perimeter of the quadrangular stimuli was 6 × 6 cm2 for the small size and 8 × 8 cm2 for the big size; the diameter of the circular stimuli was 6 cm for the small size and 8 cm for the big size. The height was the same as the dimensions of the bases, except parallelepiped and cylinder whose heights were 9 cm for the small size and 11 cm for the big size. The stimuli were combined in such a way as to obtain 12 triads. Based on previous studies with normally sighted individuals (Iachini & Ruggiero, 2006) and confirmed with visually impaired individuals (Iachini et al., 2014; Ruggiero et al., 2009, 2012), each triad was arranged on a desk according to the following criteria: (1) the inter-object and body-object metric distances were devised to allow participants to quickly and reliably distinguish relative distances, excluding errors due to metric confusion or overlap; (2) the metric distances were set such that the amount of metric difficulty was the same for egocentric and allocentric judgements.
The metric difficulty was related to the amount of distance between stimuli (see Figure 1). In this example, the inter-stimuli distances were cube–sphere = 11 cm, sphere–cylinder = 17 cm, and cylinder–cube = 28 cm. The cube and the cylinder were 12 and 6 cm far from the body, respectively. The target object (i.e., the point of reference) for the allocentric judgements was the sphere. The metric difference between the two objects closer to the body was 6 cm (12–6) and was the same as the metric difference between the two objects closer to the sphere (17–11). The arrangement of materials was based on pilot studies presented in previous reports (Iachini & Ruggiero, 2006; see also Iachini et al., 2014; Ruggiero et al., 2012). To ensure that all triads were presented in the same way, a 2-cm thick plasterboard panel (measuring 50 × 30 cm) was used. This panel was the same size as the desk. On this plasterboard panel, the shape forming the base of each object was engraved and the corresponding object was placed there.
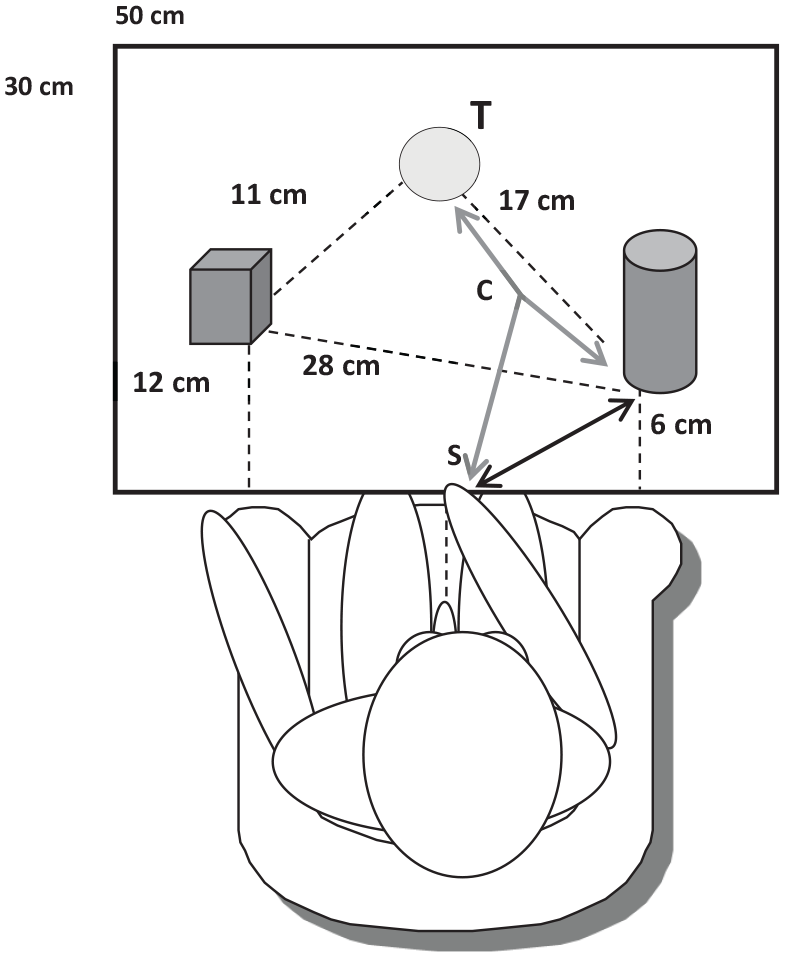
Example of stimuli and exploration modality for congenitally and adventitiously blind and blindfolded sighted participants. Objects placed on a panel covering a small desk. Black dashed lines indicate relative distances between objects (e.g., cube–sphere). Black bold arrows represent the trajectory along which the experimenter guided participants’ hand during the body-object exploration. Grey bold arrows indicate the trajectories along which participants’ hand was led during the object-to-object exploration. Objects were explored one by one, with participants’ hand being led along straight routes back-and-forth from the starting position to each object. To perceive the body-object distance, participants’ hand was guided from the starting position (“S”) towards one object (e.g., cylinder), then back to the starting point, and next to the other object (e.g., cube). The starting position, i.e., the position from which participants’ hands were led towards stimuli, corresponded to the middle of the board (25 cm on the bottom). To perceive the object-to-object distance, participants’ hand was initially led to the middle of a pair of stimuli (“C”), towards one object (e.g., sphere), then back to the point “C” and next to the other object (e.g., cylinder), and back again.
Procedure
Participants were first given written instructions (in Braille for blind participants) describing the experimental procedure. Then, there was a training session using three common objects (e.g., a glass, a cup, and a small box). Afterwards, all 12 experimental stimuli were presented one by one and participants had to recognise and name them correctly. This phase lasted approximately 2.30/3 min. In this way, difficulties due to naming, recognition, and recall problems could be excluded. After the familiarisation with the stimuli, there was a training phase. Blind and blindfolded participants explored the objects by touching them, whereas sighted participants who were not blindfolded simply observed the objects. Then participants provided egocentric/allocentric judgements, and the procedure was repeated until the task was performed without difficulty and they declared that everything was clear. Afterwards, the experiment started. The experiment was characterised by a learning and a testing phase.
Learning phase
All participants sat in front of a desk. The experimenter presented a triad of objects on the desk. All participants were instructed to memorise as accurately as possible the objects and their positions. Participants did not know in advance which judgements they would be asked. The way in which the identity of objects and their position was learned (10 s) differed for sighted and blind/blindfolded participants. While the first explored the triads by looking at them, the latter were conducted by the experimenter to explore the objects by touch. Specifically, to perceive the body-object distances (see Figure 1), participants’ hand was led along straight routes from the starting position close to their body towards one object (e.g., cylinder), then back to the starting point, and next to the other object (e.g., cube). To perceive the object-to-object distances (see again Figure 1), their hand was led to the middle of a pair of stimuli (point “C,” Figure 1), towards one object (e.g., sphere), then back to the middle and next to the other object (e.g., cylinder). A midpoint was used to allow blind participants to work out the object-to-object distance without using the body as a direct reference and to prevent them from simultaneously touching two objects with their hand, thus using it as a parameter to measure the distance independently of the reference frame (see Iachini et al., 2014; Ruggiero et al., 2009, 2012). This procedure allowed participants to explore the triad as thoroughly as possible and encode both body-object and object-to-object distances without disparities due to the exploration method. The experimenter guided the participants’ hand to each object. Each object was explored twice, and the order of haptic exploration was randomised. This sequential exploration procedure ensured effective stimulus memorisation (Iachini et al., 2014; Ruggiero et al., 2009, 2012, 2018). Once the triad was memorised, all participants were instructed to say “stop” and had to remove their hands from the panel, whereas sighted participants closed their eyes. Afterwards, the triad was removed and the testing phase started (5-s delay).
Testing phase
Participants were asked to verbally provide two kinds of spatial judgements for each triad, in a counterbalanced order (total judgements = 24). The questions were “which object was closest/farthest to you?” (egocentric); “which object was closest/farthest to a target object (e.g., cone)?” (allocentric). For each judgement accuracy (1 = correct; 0 = incorrect; score range = 0–12 for each spatial frame), RT (s) was calculated. The order of presentation of the questions was first randomised and then balanced across subjects. The time (s) required to provide each spatial judgement was recorded from when the experimenter announced the implied frame of reference (body or target object) until participants provided the response, i.e., the time between the end of the question and the beginning of the answer. A hand-held stopwatch was used to record the RT.
Data analysis
Two separate mixed ANOVAs with a eight-level between-factor “Groups” (young and old congenitally blind, young and old adventitiously blind, young and old blindfolded sighted, young and old sighted participants) and a two-level within-factor “Reference Frames” (egocentric and allocentric) were performed on mean accuracy (0–1) and RT (s). The mean accuracy of each participant was calculated in terms of percentage of correct answers by dividing the total correct answers by 12 (i.e., the maximum accuracy for condition; e.g., ego–allo). The same procedure was adopted to calculate mean RT for each condition. Moreover, separate ANOVAs were performed with sex as an added factor on performance (acc, RT). Correlation analyses were performed to check for speed–accuracy trade-off effects. Finally, the Tukey’s honestly significant difference (HSD) test was used to analyse post hoc effects and the magnitude of the significant effects was indicated by partial eta squared (ηp2).
Results
Accuracy
Descriptive statistics for each group as a function of egocentric and allocentric spatial judgements are shown in Table 2 and Box Plots a and b of Figure 4.
Means and standard deviations of accuracy (0–1) for egocentric and allocentric judgements as a function of age and visual status.
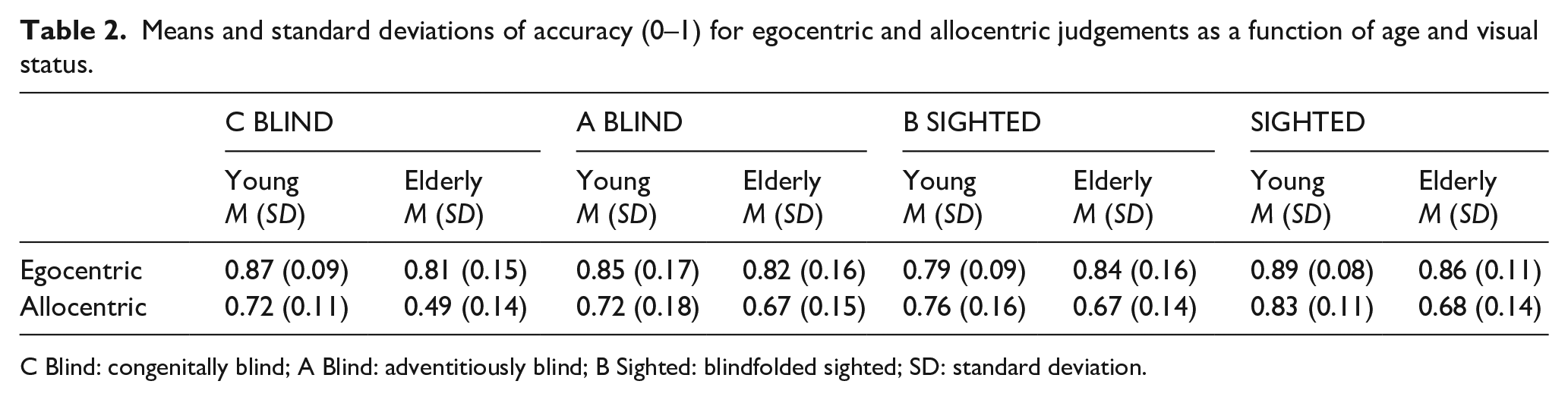
C Blind: congenitally blind; A Blind: adventitiously blind; B Sighted: blindfolded sighted; SD: standard deviation.
The results showed a main effect of the Reference Frames, F(1, 152) = 105.541, p < .001, ηp2 = .41, due to the egocentric judgements (M = 0.84, SD = 0.13) being more accurate than allocentric ones (M = 0.69, SD = 0.16). A main effect of the Groups was also observed: F(7, 152) = 6.480, p < .001,
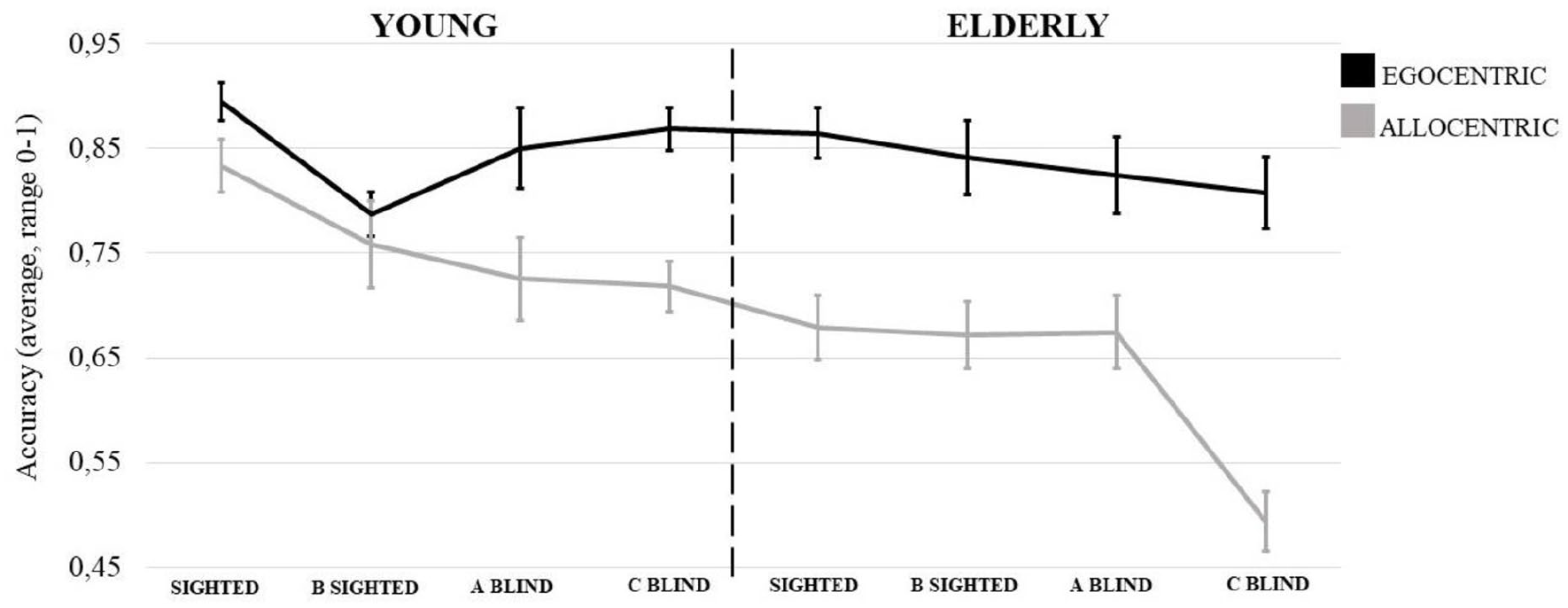
Mean of accuracy (0–1) for egocentric and allocentric spatial judgements as a function of age groups and visual status (Sighted; B Sighted: blindfolded sighted; A Blind: adventitiously blind; and C Blind: congenitally blind). Vertical grey thin bars denote standard errors.
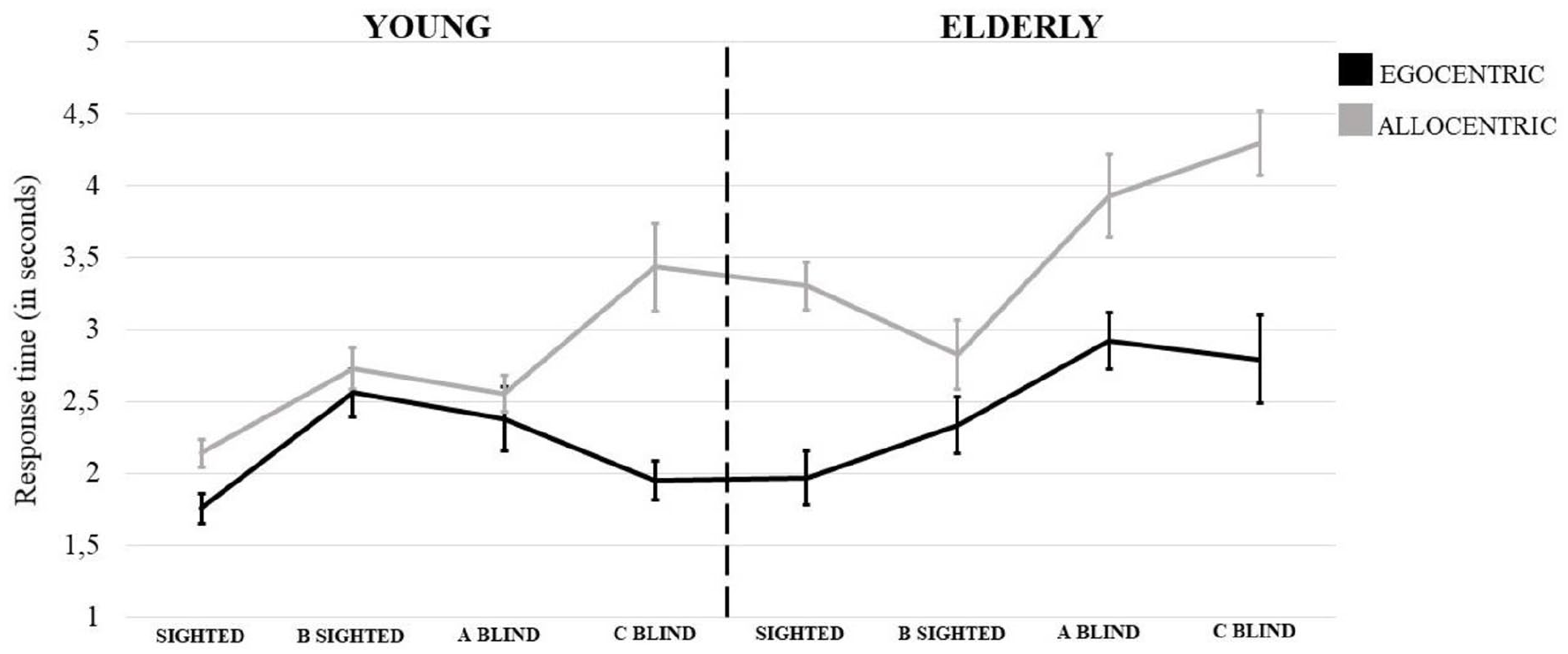
Mean of RT (s) for egocentric and allocentric spatial judgements as a function of age groups and visual status (Sighted; B Sighted: Blindfolded Sighted; A Blind: Adventitiously Blind; and C Blind: Congenitally Blind). Vertical grey thin bars denote standard errors.
RT
Descriptive statistics for each group as a function of egocentric and allocentric spatial judgements are shown in Table 3 and Box Plots c and d of Figure 4.
Means and standard deviations of RT (s) for egocentric and allocentric judgements as a function of age and visual status.

C Blind: congenitally blind; A Blind: adventitiously blind; B Sighted: blindfolded sighted; SD: standard deviation.
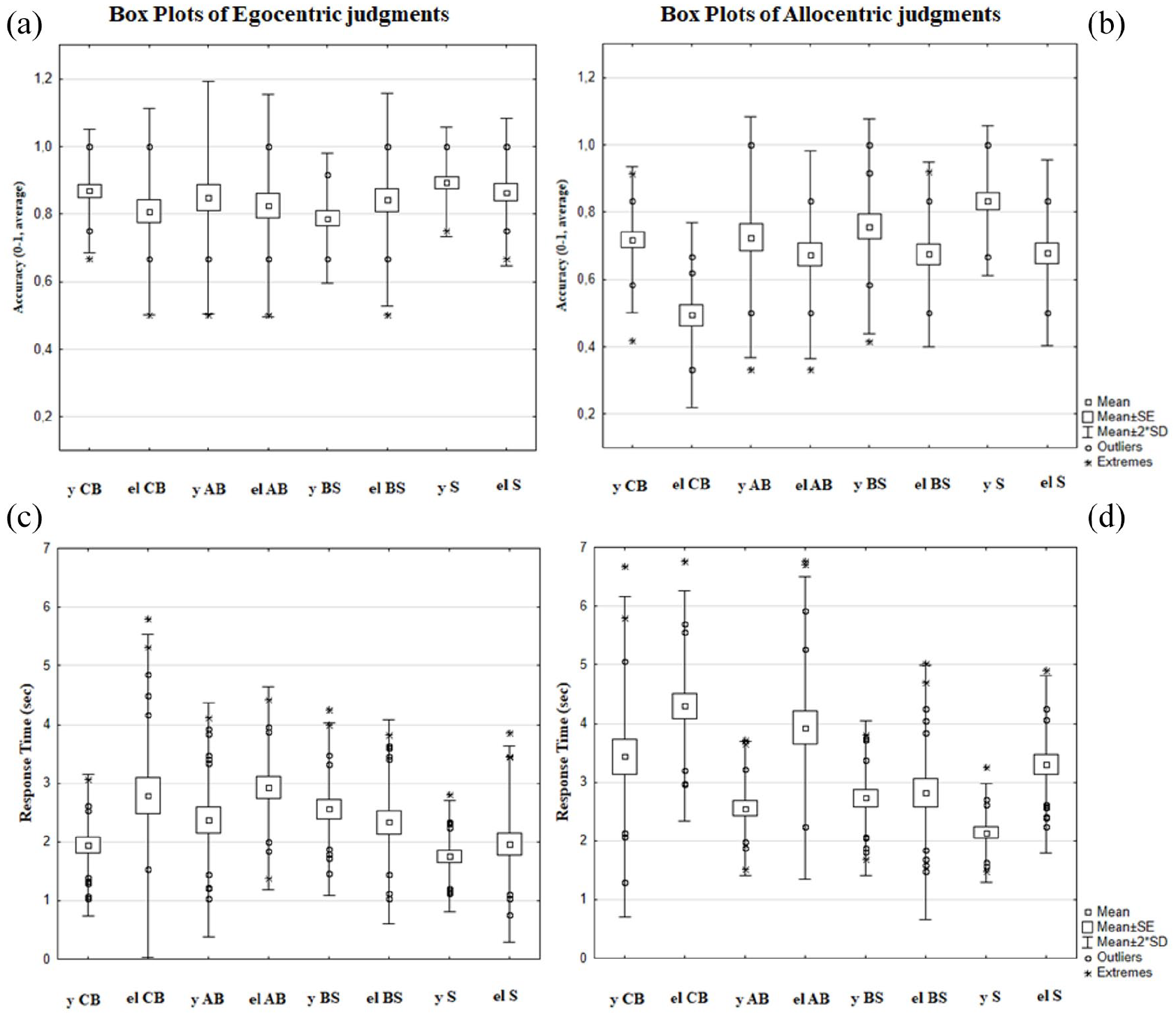
(a) Box plots of accuracy for egocentric spatial judgements; (b) Box plots of accuracy for allocentric spatial judgements; (c) Box plots of RT for egocentric spatial judgements; (d) Box plots of RT for allocentric spatial judgements. The plot shows mean, mean ± standard error, data within two SDs and data falling outside two SDs (extremes, outliers). y CB: young Congenitally Blind; el CB: elderly Congenitally Blind; y AB: young Adventitiously Blind; el AB: elderly Adventitiously Blind; y BS: young Blindfolded Sighted; el BS: elderly Blindfolded Sighted; y S: young Sighted; el S: elderly Sighted.
The results showed a main effect of the Reference Frames, F(1, 152) = 85.349, p < .001,
Correlation analyses
The analysis revealed no speed–accuracy tradeoff effect. In general, the more accurate both judgements were, the faster the processing time was (Egocentric: r = −.32, Allocentric: r = −.31, at least p < .05). Within each group, the only significant effects were due to negative correlations: the more accurate egocentric judgements were, the faster the processing time was for the congenitally blind elderly group (r = −.44), and for the young (r = −.71) and elderly (r = −.46) adventitiously blind groups.
Discussion
The ability to process efficiently egocentric and allocentric spatial representations is fundamental in our daily life activities. For theoretical and clinical reasons, separate lines of research have sought to understand how ageing and blindness can compromise their effective processing. In this study, we assessed the concurrent effect of these factors by comparing young and old people with different degrees of visual experience on a spatial memory task that required egocentric and allocentric reference frames (Iachini & Ruggiero, 2006).
The results confirmed that ageing and blindness negatively affected the processing of allocentric information. Importantly, there was a clear allocentric difficulty in congenitally blind people compared to all other individuals with varying degrees of visual experience. This difficulty was expressed in slower processing time and lower accuracy.
Moreover, the combination of age and the absence of any visual experience resulted in an interaction whereby the congenitally blind elderly people performed worse than all other groups. This confirms a specific allocentric difficulty due to the lack of visual experience (Millar, 1994; Ruggiero et al., 2012; Ruggiero, Ruotolo, & Iachini, 2018; Thinus-Blanc & Gaunet, 1997). Instead, the residual visual experience exploited by adventitiously blind people and the long-term visual experience (even when visual information was temporarily unavailable) of sighted people helped the allocentric processing. The important role of age, alongside visual status, is also demonstrated by the fact that sighted young participants were more accurate than all elderly participants, regardless of their visual experience.
In line with our hypothesis, ageing and visual status did not affect the accuracy of the egocentric processing. Indeed, the level of egocentric accuracy was similar (at least > 79%) in all groups. This may reflect the primacy of egocentric organisation of spatial information in humans that can be attributed to our natural egocentric perspective-mediated interface with the environment (e.g., Delius & Hollard, 1995; Millar, 1994). In this regard, the small-scale of the spatial array may have facilitated the performance, as also shown by previous studies (Iachini et al., 2014; Ruggiero et al., 2012). The short duration of hand-/body-centred sequential exploratory processes, the capacity to exploit Working Memory, and attentional resources to integrate piecemeal spatial information may help the spatial performance, in particular the egocentric one (Cornoldi & Vecchi, 2004; Iachini et al., 2014; Millar, 1994). In addition, contrary to large-scale spaces, the body could provide a stable anchor point. Indeed, while sighted participants could easily gather spatial information at a glance, blind or blindfolded sighted participants could haptically explore the arrays within reach and remain in the same position throughout the task. This may have been particularly beneficial for congenitally blind people who prefer egocentric encoding strategies due to the limited amount of distal information provided by the environment (Maurer et al., 2005; Millar, 1994).
One might argue that spatial memory for a small-scale environment can be weakly related to a large-scale environment. In fact, the encoding of spatial information in the latter case is more effortful due to the longer duration of exploratory processes and the limitations of the working memory and attentional resources needed to organise spatial information (Iachini & Ruggiero, 2010). Previous work using the same experimental task with blind and sighted people and comparing small- versus large-scale spatial arrays has shown a more difficult performance for the latter (Iachini et al., 2014). The allocentric limitation was more evident in large-scale space, but still present in its small-scale version (see also Pasqualotto & Newell, 2007). Even if our setting does not reflect the complexity of navigable environments, it has the advantage of helping to identify specific difficulties in the basic spatial components (Ruggiero et al., 2020). However, since the sector of space reveals different levels of cognitive decline during ageing (Lester et al., 2017; Moffat, 2009; Segen et al., 2021; Wiener et al., 2013; Wolbers et al., 2014), future studies should investigate the impact of ageing and visual impairment on spatial memory concerning near and far spaces.
Consistent with accuracy, ageing and visual status affected allocentric information processing time, slowing down older people compared to younger people and speeding up sighted people with full availability of visual information compared to all other groups. In fact, the time to process allocentric information was slower in congenitally blind elderly people than all other groups except their younger counterparts and adventitiously blind elderly individuals. A similar, though weaker, effect emerged when the onset of blindness was later. Finally, sighted young participants were faster than both young and elderly congenitally blind people, and also sighted (blindfolded or not) elderly participants.
Overall, the results confirm that representing spatial information allocentrically constitutes an effortful process that is worsened by the concurrent effect of blindness and ageing (Millar, 1994; Pasqualotto et al., 2013; Vecchi et al., 2004). Several studies have shown that the absence of any visual experience makes it difficult to effectively represent allocentric information (Cattaneo et al., 2008; Iachini et al., 2014; Pasqualotto et al., 2013; Ruggiero et al., 2012; Ruggiero, Ruotolo, & Iachini, 2018; Thinus-Blanc & Gaunet, 1997). Visual experience seems to be necessary to develop the ability to integrate and represent multiple spatial relations, as it is able to encode information in parallel compared to the sequential nature of non-visual modalities (e.g., Pasqualotto & Proulx, 2012). Therefore, non-visual modalities might not be able to fully compensate for the lack of visual experience, thus leading to a preference for egocentric encodings (Iachini et al., 2014; Noordzij et al., 2006; Postma et al., 2008; Vecchi et al., 2004).
The early onset of blindness produces an extensive cerebral reorganisation that can deeply affect the spatial mechanisms involved in allocentric spatial representation (Cattaneo et al., 2008; Iachini & Ruggiero, 2010; Merabet & Pascual-Leone, 2010; Pasqualotto & Proulx, 2012; Vecchi et al., 2004). This might explain a clear effect found in this study, namely the strong allocentric difficulty of congenitally blind people and, conversely, the similar performance of adventitiously blind (i.e., late visual deprivation), blindfolded sighted (i.e., short-term visual deprivation), and sighted people. While congenitally blind people have never experienced simultaneous visual encoding of spatial information, adventitiously blind people might still resort to their residual visual experience, along with non-visual sensory channels, to help represent reciprocal spatial relationships between external locations (Cattaneo et al., 2008; Iachini et al., 2014; Ruggiero et al., 2012; Thinus-Blanc & Gaunet, 1997). This is also in line with the evidence that adventitiously blind people perform better than congenitally blind participants and sometimes similarly to sighted controls on several spatial tasks (e.g., Millar, 1994; Pasqualotto & Proulx, 2012; Thinus-Blanc & Gaunet, 1997). Therefore, late vision loss would allow the integration of extensive haptic experience with residual visual capacity to effectively represent a spatial array as a whole (Cornoldi et al., 1991; Millar, 1994; Ruggiero & Iachini, 2010; Thinus-Blanc & Gaunet, 1997). As concerns blindfolded sighted adults, they can show a similar performance to sighted participants (Cattaneo et al., 2008; Iachini et al., 2014; Ruggiero et al., 2012). In fact, even if visual information is temporarily unavailable, blindfolded participants can exploit their long-term vision-based encoding modality that allows them to represent allocentric relations in a similar way to how sighted participants do (Ruggiero et al., 2009; Ruotolo et al., 2012; for reviews, see Pasqualotto & Proulx, 2012; Thinus-Blanc & Gaunet, 1997). The present findings add to the literature showing a reduced allocentric ability in elderly people (Colombo et al., 2017; Moffat, 2009; Montefinese et al., 2015; Ruggiero et al., 2016). Ageing is characterised by the natural decline of the medio-temporal structures of the brain and hippocampal formation that support the allocentric representations (Iachini, Ruotolo, & Ruggiero, 2009; Li & King, 2019; Moffat, 2009; Rosenbaum et al., 2012; S. Serino et al., 2014). Regarding the effect of blindness, even though the hippocampus can efficiently work with non-visual inputs (haptic, auditory, etc.), vision may be necessary for fine-tuning non-visual sequential information (Poucet et al., 2000) resulting in reduced performance in allocentrically based spatial tasks.
Conclusion
The concurrent effect of the absence of visual experience and ageing may lead to increased difficulty in representing spatial relationships between elements in space (Cornoldi et al., 1991; Ruggiero & Iachini, 2010; Vecchi et al., 2004). This limitation especially penalises congenitally blind elderly people in their capacity to effectively process allocentric frames. By contrast, blind people may sufficiently compensate the difficulties arising from the absence of sight when their body provides a stable anchorage. Finally, this study emphasises the necessity of investigating spatial memory and its links to daily life activities. It also provides insights for devising a cognitive intervention to maintain and rehabilitate the spatial abilities of blind people.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.