
Abstract
Obesity is a clinical condition that impacts severely the physical body. However, evidence related to the mental representation of the body in action is scarce. The few available studies only focus on avoiding obstacles, rather than participants imagining their own body. To advance knowledge in this field, we assessed the performance of 22 individuals with obesity compared with 30 individuals with a healthy weight in two tasks that implied different motor (more implicit vs. more explicit) imagery strategies. Two tasks were also administered to control for visual imagery skills, to rule out confounding factors. Moreover, we measured body uneasiness, through a standard questionnaire, as body image negativity could impact on other body representation components. Our findings do not show differences in the motor imagery tasks between individuals with obesity and individuals with healthy weight. On the other hand, some differences emerge in visual imagery skills. Crucially, individuals with obesity did report a higher level of body uneasiness. Despite a negative body image and visual imagery differences, obesity per se does not impact on the representation of the body in action. Importantly, this result is independent from the level of awareness required to access the mental representation of the body.
Introduction
When individuals are asked to imagine performing a movement or rotating a body part to match the position of the corresponding physical part, the mental simulation grounds on the cognitive representation of their body in action (Coslett et al., 2010; Rumiati et al., 2010; Schwoebel et al., 2001). This ability to imagine bodily movements is known as motor imagery, the active process of internally representing a motor act, without an overt movement (Parsons, 1987; 1994; Rumiati et al., 2010). The most traditional motor imagery task used in psychology is the Hand Laterality Task (Parsons, 1987; Sirigu et al., 1996), in which individuals judge if a visual stimulus represents a left or a right hand (i.e., laterality judgement) independently from its spatial rotation (i.e., the hand is shown without any rotation or rotated 180°) and view (i.e., the palm or the dorsum of the hand is shown). To perform such a judgement, individuals imagine to rotate the position of their real hand to match that of the shown hand, with no instruction about how to complete the task (Hétu et al., 2013). Thus, this strategy is used implicitly: individuals do not need to consciously access their representation of the body; in other words, they do not need to be aware of the imagery process (Longo, 2015). Laterality judgements are more accurate and faster when body parts are shown in a position which is easy and comfortable to reach, mirroring the physical body constraints (Parsons, 1987; Sirigu et al., 1996): this behavioural evidence, known effect of biomechanical constraints (Parsons, 1987), supports a tight link between our ability to carry out actions and the corresponding representation of the body. Similar evidence emerges when a less implicit motor imagery task is used, such as the Mental Motor Chronometry Task (Brusa et al., 2021; Scarpina, Magnani, et al., 2019; Schwoebel & Coslett, 2005). In this task, individuals are asked to imagine performing movements with their limbs. As such, they are consciously aware of the process required to solve the task (i.e., imagining their body parts performing a particular movement): they focus on the specific motor sequences that should be imagined in addition to the movements per se, as suggested by Hétu and colleagues (2013). Thus, because of such characteristics, the Mental Motor Chronometry is considered a more explicit task. The time required to mentally simulate the movements is strictly related to the time required to physically perform those movements, again supporting the link between moving and imagining to move.
Motor imagery is traditionally used to explore the mental representation of the body related to actions in different conditions, such as movement disorders (Fiori et al., 2013, 2014; Scarpina, Magnani, et al., 2019), pain (Coslett et al., 2010; Schwoebel et al., 2001), and congenital absence of body parts (Funk & Brugger, 2008). However, in some clinical conditions, the physical body is subject to changes that might impact on the ability to move, even in absence of motor or neurological impairments. An example of such conditions is obesity, that is a clinical condition characterised by an excessive accumulation of body adiposity (World Health Organisation, 2000), due to an energy imbalance between calories consumed and calories expended, with some limitations in functional mobility and thus decreased quality of life (Forhan & Gill, 2013; Wearing et al., 2006). The body mass index (BMI) is used to define if an individual’s weight in the range of obesity, with a threshold of the BMI being greater than 30. Obesity modifies body geometry, since it increases the mass of limb segments (Rodacki et al., 2005), as well as affected individuals perform fundamental daily activities, such as standing (Teasdale et al., 2007) and walking (Cimolin et al., 2011; Scarpina et al., 2017), as they tend to minimise joint movements, especially at knee and hip level, to avoid pain and musculoskeletal injury. Also, there is some even though scarce evidence relative to altered grasping or pointing to an object (Berrigan et al., 2006; D’Hondt et al., 2008). Moreover, some alterations in interoceptive perception, such as sensory attenuation (Scarpina et al., 2022), appetite response (i.e., Gluck et al., 2017), and heart rate variability (i.e., Godfrey et al., 2019), have been described in this condition with possible effect in shaping bodily experience (for a recent review, Robinson et al., 2021).
Previous evidence on the cognitive representation of the body in action in obesity is sparse and heterogeneous, despite the importance of this function to successfully interact with the environment as well as for treatment purposes. Some previous studies suggest a distorted mental representation of the body in this clinical population. For instance, when individuals with obesity walk through door-like apertures of different widths, their body-scaled motoric behaviour is similar to that reported by individuals with a healthy weight, despite the significantly larger bodily dimensions (Scarpina et al., 2017). Individuals with obesity tend to underestimate their bodily dimensions when they perform online movements, acting similarly to healthy-weight individuals. On the other hand, Guardia and colleagues (2013) describe a female patient who lost 60 kg (her initial weight was of 125 kg, for a height of 1.65 m; thus, the initial BMI being 45.9 kg/m2), and who suffered of a severe body dissatisfaction. According to the original description, this individual not only overestimated her bodily dimensions when she had to pass through door-like apertures, rotating her shoulder more than her physical dimensions should require, but also reported such a misjudgement when she estimated whether or not an aperture was wide enough for her to pass through, prior to actually performing the action. These two studies differ not only in the results (underestimation versus overestimation), but also in the methods used. While in Scarpina and colleagues (2017) participants were induced to think they were performing a memory task, and hence relying on a more implicit motor imagery strategy to perform actions, in Guardia and colleagues (2013) the participant explicitly imagined to perform the movement before the real action. Interestingly, the role of strategy in obesity is evident in other tasks involving the body, but not actions: as reported in a recent review (Tagini, Scarpina, & Zampini, 2021), affected individuals traditionally show an altered mental representation of their own physical dimensions when they are explicitly asked to judge them (i.e., Scarpina et al., 2014, 2017; Schwartz & Brownell, 2004); however, they describe the same features accurately when the processes are implicit (as in Tagini, Scarpina, Scacchi, et al., 2021). It is worth to note that both Guardia and colleagues (2013) and Scarpina and colleagues (2017) tested an obstacle-avoidance action, a walking through door-like openings). As such, both studies tested actions in relation to an external object (i.e., the doors) that must be avoided to prevent collisions. In such cases, the brain computes time-by-time the spatial position and the movement of the body in relation to the spatial positions of object (which change constantly since the body approaches it) that need to be avoided, adopting an external, environmental-centred frame of reference (Holmes & Spence, 2004). Because of this, the results provided by these two previous studies cannot be extend to include actions performed adopting an internal, observer-centred coordinates, when individuals plan, execute, and monitor their own actions, in absence of any external objects.
In this study, we investigated motor imagery in a sample of individuals affected by obesity, compared with a sample of normal-weight individuals. As previously stated, the tasks we have adopted, the Hand Laterality Task (Brusa et al., 2021; Scarpina, Magnani, et al., 2019; Scarpina et al., 2022) and the Mental Motor Chronometry Task (Brusa et al., 2021; Scarpina, Magnani, et al., 2019; Scarpina et al., 2022; Schwoebel & Coslett, 2005), implied different motor (more implicit vs. more explicit) imagery strategies in relation to the amount of the instructions furnished to the participants by the experimenter to complete the tasks (Hétu et al., 2013). If the mental representation of the body is preserved in obesity, no difference should be observed between samples in both the tasks. However, if obesity impacts globally on the representation of the body, participants affected by obesity and normal-weight individuals should show behavioural differences in both tasks. Nevertheless, given previous evidence, one could hypothesise that the impact is not widespread, and more related and more related to levels of awareness: as such, following the recent evident provided by Tagini, Scarpina, Scacchi, et al. (2021), one could expect a greater impact in the more explicit task (i.e., the Mental Motor Chronometry Task) compared with the more implicit one (i.e., the Hand Laterality Task).
Importantly, in this study we also included control tasks aimed at ensuring that any difference in the main tasks between samples is not due to a confounding effect of mental imagery (i.e., those cognitive processes consisting in retrieving, constructing and manipulating the mental representation of objects and/or events, Kosslyn et al., 1995). Difficulties across almost all cognitive domains (e.g., complex attention, verbal and visual memory, decision making) have been previously described in obesity (Liang et al., 2014; Prickett et al., 2015; Wang et al., 2016). Thus, as done in Scarpina, Magnani, et al. (2019), Scarpina et al. (2022), and Brusa and colleagues (2021), two control tasks, in which objects, instead of hands, were used as experimental target of the visuospatial mental rotation in the case of the Mental Letter Discrimination Task, and of the visual spatial movements in the case of the Mental Bars Movement Task.
As much as the focus of our study is on the mental representation of the body in relation to actions, we also included a measure for the individuals’ body image representation through a traditional questionnaire (Cuzzolaro et al., 2006). Irvine and colleagues (2019) recently suggested that body representation might be more distorted in those individuals who report negative bodily perceptions and attitudes, and as such the inclusion of this measure provides further information apt at explaining our findings, independently from which of our hypotheses is confirmed.
Methods
Participants
The study was approved by the Ethics Committee of the Istituto Auxologico Italiano (Italy), and it was performed in accordance with the Helsinki Declaration. Participants gave informed written consent before taking part in the experiment and were volunteers. They were free to withdraw at any point during the study and were naïve to the rationale of the experiment.
Only right-handed participants have been included in the study as previous studies suggested an influence of handedness in motor imagery (such as, Choisdealbha et al., 2011; Jongsma et al., 2013). Individuals with obesity were consecutively recruited at admission to the hospital. They were free from gastrointestinal, cardiovascular, psychiatric, metabolic disorders or any concurrent medical condition not related to obesity. Weight and height were measured to the nearest 0.1 kg and 0.1 cm, respectively. BMI was expressed as body mass (kg)/height(m)2. Any BMI over 30 kg/m2 (World Health Organization, 2000) was classified as obesity. Overall, twenty-eight individuals were enrolled (16 females, 12 males; age in years M = 46.92; SD = 9.88; education in years M = 11.5; SD = 2.92; BMI M = 44.68; SD = 6.47).
Thirty matched normal-weight participants (15 females, 15 males; age in years M = 46.23; SD = 10.45; education in years M = 14.16; SD = 3.7; BMI M = 22.89; SD = 1.81) were recruited outside the clinical institute through personal contacts of the researchers and word-of-mouth. The inclusion/exclusion criteria were the same as for the group with obesity, except for the BMI, for which the value had to be in a range of 18.5–25 kg/m2.
In obesity, modification in body geometry, as effect of the increased mass of limb segments (Rodacki et al., 2005), is observed. Thus, we might expect that the physical dimension of hands, which are the target of our experiment, was enlarged due to the presence of adipose tissue. Thus, we collected the anthropomorphic measures of our participants’ hands to ensure behavioural differences are not related to this physical factor. Hand width was quantified as the distance between the knuckles of the index and little fingers, and hand length as the length (knuckle-to-tip) of the middle finger. The hand shape index (SI), which reflects the overall aspect ratio of the hand, is computed according to the formula: SI = 100 × (width/length) (Longo & Haggard, 2012). Larger values indicate a wide hand, smaller values a slender hand. We also measured hand thickness, at the distance between the dorsum and the palm at the level of the knuckles of the middle finger. All the measures were performed using a standard calliper, on both hands.
Body uneasiness test
All the participants were required to fill out the Body Uneasiness Test (BUT; Cuzzolaro et al., 2006). This is a widely used clinical instrument to assess body uneasiness in obesity (Marano et al., 2007); specifically, the questionnaire has been designed to investigate the level of body dissatisfaction and the other dimensions of so called “negative body image,” such as perceptual, cognitive, emotional, relational, and behavioural components (Rosen, 1998). It consists of two parts. The BUT-A scores are combined in a global severity index and in five sub-scales: weight phobia (fear of being or becoming fat), body image concerns (worries related to physical appearance), avoidance (body image related avoidance behaviour), compulsive self-monitoring (compulsive checking of physical appearance), and depersonalization (detachment and estrangement feelings towards the body). BUT-B focuses on specific worries about specific body parts or functions; scores are combined in two global measures (positive symptom total, and positive symptom distress index). Higher scores for both parts indicate greater body uneasiness. This questionnaire has been validated in patients with obesity and has good internal consistency (Cronbach’s α coefficient > 0.7) (Marano et al., 2007).
Experimental tasks
To explore the more implicit and the more explicit components of motor imagery, the Hand Laterality Task and the Mental Motor Chronometry Task were used. Two control tasks, the Mirror Letter Discrimination Task and the Mental Bars Movement Task, were administered to explore visual imagery skills (respectively, for the more implicit and the more explicit component). The tasks are described in full in Scarpina, Magnani, et al. (2019), Scarpina et al., 2022, and Brusa and colleagues (2021). Each task was preceded by a practice block. A laptop with a 15.6 inches screen was used. The experiment was scripted through Psycho-Py 1.83.03 (Peirce, 2007).
Hand laterality task
Pictures of right back/palm and left back/palm hands are shown to participants in four different rotations: 0°; 90°; 180°; 270°. Hands oriented at 0° and 180° are considered to detect the effect of stimulus orientation. To extract the effect of biomechanical constraints, right hands oriented at 270° and left hands at 90° are used to compute the index for comfortable postures, while right hands oriented at 90° and left hands at 270° are used for awkward postures. Ninety-six trails are presented to participants, composed of 16 pictures (eight for the right hand, eight for the left hand) in back or palm perspective. Trials are divided into two blocks (48 trials for each block): each stimulus is presented six times (three in the first and three in the second block) in a randomised order. Pictures measured 1100 × 777 pixels to cover a 21 by 23 degrees visual angle when the images were displayed at a distance of 50 cm. Participants sat in front of the computer screen with their left and right index fingers on the “z” and “m” keys of the keyboard. They judged if the stimulus represented a right or a left hand by pressing, as quickly and as accurately as possible, the “z” key if the picture on the screen was a left hand or the “m” key if the picture was a right hand in one block, and the reverse in the other block. Block order was randomised between subjects. Each trial was preceded by a fixation cross lasting 1500 milliseconds. Each stimulus stayed on the screen since participants provided an answer or for a maximum time of 5000 milliseconds (if the participant did not answer).
For each trial, reaction time (RT) in milliseconds and the answer provided by participants were recorded. Average RT in milliseconds (correct answers only) and average Accuracy (the percentage of correct answers) were calculated for each combination of Orientation and Posture.
Mental motor chronometry task
During the task, individuals are blindfolded. Four movements are assessed: (1) index and thumb opposition; (2) thumb extension from the fist; (3) middle finger crossed on the index finger; (4) extension of the index and the little fingers. In the imagery condition, participants are required to imagine performing each movement as quickly and as accurately as possible, five times consecutively. Instead, in the execution condition, they are required to perform each movement, five times consecutively. The order of movements and conditions (the imagery condition presented first) is the same for all participants. The starting hand is counterbalanced between subjects. Both the right and left hand are tested. Overall, the task is composed of 16 trials: four gestures for two hands (right and left); two conditions (imagined vs. executed) were tested. During the task, participants sat in front of a computer screen with their left or right index finger (depending on the starting hand) on the spacebar. After the instructions indicating which movement participants were required to perform or imagine, participants closed their eyes and imagined or executed the target movement five times consecutively. When finished, participants pressed the spacebar. For each movement, time required to imagine and to execute the five repetitions of each movement was collected, in seconds.
Control task for the hand laterality task: mirror letter discrimination task
Participants judged if an alphanumeric character is shown in a canonical or mirror-reversed position. The visual stimuli were the letters “F” and “J” shown in canonical or mirrored-reversed positions (Type), in four different Orientations: 0°; 90°; 180°; 270°. Number of trials and blocks was the same as in the Hand Laterality Task. Participants sat in front of the screen (at a distance of 50 cm) with their left and right index fingers on the “z” and “m” keys, respectively. They were asked to press as quickly and as accurately as possible the “z” key if the picture on the screen represented a canonical letter or by the “m” key if the picture represented a mirror-reversed letter in one block, and in the reverse way in the other block. The block order was randomised between subjects, as for the Hand Laterality Task. Stimulus timing was the same of the Hand Laterality Task. For each trial, RT in milliseconds and the answer provided by participant are collected. Average RT in milliseconds and average Accuracy (the percentage of correct answers) are calculated for each combination of Orientation and Type.
Control task for the mental motor chronometry task: mental bars movement task
In this task, participants imagined four movements: (1) two bars getting close to each other; (2) one bar raising up from the other bars; (3) two bars crossing each other; and (4) two bars extending together from bottom to up. The order was the same for all participants. At the beginning of each trial, participants read written instructions relative to the movement; they also saw an example. They then closed their eyes and imagined the target movement five times, as quickly as possible. When finished, they immediately pressed the spacebar. Two blocks of eight trials were tested: in one block participants respond with the right hand and in the other block they respond with the left hand. The starting hand is counterbalanced between subjects, as in the Mental Motor Chronometry Task. For each bar movement, the time required to imagine the five repetitions is collected in seconds.
Experimental procedure
Following the procedure described in previous works (Brusa et al., 2021; Scarpina, Magnani, et al., 2019; Scarpina et al., 2022), the control task (i.e., the Mirror Letter Discrimination Task and the Mental Bars Movement Task) was always administered before the corresponded main task (i.e., the Hand Laterality Task and the Mental Motor Chronometry Task) in order to ensure consistent activation of imagery processes and to avoid carryover effects from the control tasks to the motor imagery tasks. Differently, the order in which components (implicit vs. explicit) were tested was randomised between participants. Thus, half of participants performed first the implicit tasks (i.e., the Hand Laterality Task and the Mirror Letter Discrimination Task), and then the explicit tasks (i.e., Mental Motor Chronometry Task and the Mental Bars Movement Task); the opposite order (first the explicit tasks, after the implicit tasks) was followed for the other half of participants. Finally, the completion of the psychological questionnaire and the measurement of body dimensions were performed at the end of the experimental tasks.
Data analyses
Pearson’s chi-square test was used to check for any difference in of Sex (male vs. female) distribution between samples. An independent sample t test was used to check for differences between the two groups in terms of all the other demographic features. A non-parametric Mann–Whitney U test was used to compare groups at the questionnaire.
Hand laterality task
We removed from this task and from the entire experiment participants who showed a level of accuracy below the threshold of 50% accuracy for stimuli displayed at 0° (the easiest stimuli, for which one should not expect errors), which might suggest that the participant was randomly guessing his or her responses. RT and Accuracy were analysed separately after data pre-processing for errors and outliers. RT for trials in which participants gave the wrong response was discarded from the analyses (error pre-processing). Outliers were removed using a cutoff of two standard deviations above and below the individual participant mean, as indicative of anticipation and lack of attention, respectively (outliers pre-processing). After pre-processing, RT and Accuracy for each orientation (0°; 90°; 180°; 270°), for the right and left hand separately, were calculated for each participant. Two effects were considered: the effect of stimulus orientation and the effect of biomechanical constraints (Parsons, 1987). The effect of stimulus orientation was investigated through a mixed analysis of variance (ANOVA), with Orientation (0° vs. 180°) as within-subjects factors and Group (individuals with obesity vs. healthy-weight controls) as between-subjects factor. A significantly higher level of accuracy and a faster reaction time for stimuli at 0° than those at 180° should be exepcted if the effect is present. The effect of biomechanical constraints was explored through a mixed ANOVA with Posture (comfortable vs. awkward) as within-subjects factors and Group (individuals with obesity vs. healthy-weight controls) as between-subjects factor. A significantly higher level of accuracy and a faster reaction time for stimuli showing hand in comfortable position rather than in awkward position should be exepcted, if the effect is present. Post hoc comparisons were carried out using estimated marginal means Bonferroni corrected for multiple comparisons, in case of a significant interaction.
For both the experimental effects, we also calculated and analysed the efficiency score (IES) (Townsend & Ashby, 1983) which combines accuracy and latencies as the average of correct RT divided by the proportion of correct responses. Indeed, attentional difficulties are described in obesity (Liang et al., 2014; Prickett et al., 2015; Wang et al., 2016); thus, some individuals may be significantly slower, but accurate in their judgement. IES scores were then submitted to a mixed ANOVA, with Orientation (0° vs. 180°) or Posture (awkward vs. comfortable), and Group (individuals with obesity vs. healthy-weight controls) as between-subjects factor.
Mental motor chronometry task
For each group, the relationship between the time required to imagine movements and the time required to execute movements, which is an index of motor imagery, was investigated through Spearman’s correlation, run independently for the right hand and the left hand. Indeed, hand dominance might unveil different effects in motor imagery task (Choisdealbha et al., 2011; Jongsma et al., 2013). A preliminary inspection of the raw data showed the presence of possible outliers. However, we decided not to remove the outliers, as done in Brusa and colleagues (2021) and Sirigu and colleagues (1996); indeed, for this task the correlation between acting and imagining shows up even if baseline times for participants are different. One participant might require more time to perform and imagine performing movements, but nonetheless show the correlation between the two components.
In case of statistically significant results in Spearman’s correlation, the coefficients were transformed into z scores to directly compare groups. This transformation is known as Fisher’s r to z transformation (Fisher, 1915, 1921) and can be performed on the following website: http://vassarstats.net/rdiff.html.
Mental letter discrimination task
As with the Hand Laterality Task, we excluded individuals who responded below the threshold of 50% accuracy for stimuli displayed at 0°. We then pre-processed data for errors and outliers. RT and Accuracy were computed for each orientation (0°; 90°; 180°; 270°) in mirror and canonical positions. The effect of stimulus orientation was investigated through a mixed ANOVA with Orientation (0° vs. 180°) and Type (canonical vs. mirror) as within-subjects factors and Group (individuals with obesity vs. healthy-weight controls) as between-subjects factor. Post hoc comparisons were carried out using estimated marginal means Bonferroni corrected for multiple comparisons, in case of significant interactions. A higher level of accuracy and faster RT for stimuli at 0° in comparison with those at 180° can be expected, as well as for stimuli in canonical format than in mirror format. Also for this task, we computed the IES (Townsend & Ashby, 1983), and we explored any difference between the groups with a mixed ANOVA with the within-subjects factors of Orientation (0° vs. 180°) or Type (canonical vs. mirror) depending on which effect was being analysed.
Mental bars movement task
For each group, the relationship between the time required to answer with the right hand and with the left hand was analysed using Spearman’s correlation. We used Fisher’s transformation (Fisher, 1915, 1921) to directly compare groups’ performance.
For experimental tasks, we computed and reported the 95% standard symmetric confidence intervals (CI), to quantify the uncertainty in our finding (Thomas, 1997): this value, computed according to the means and the standard deviations, represents the range of values around which the population value should be contained with 95% of probability.
Results
Two participants with obesity scored below 50% of accuracy for stimuli displayed at 0° in the Hand Laterality Task; as such, they were excluded from the experiment. Four participants with obesity were excluded from the entire experiment, since their performance was below the cutoff of 50% in the Mental Letter Discrimination Task. No controls were excluded in either tasks. The final sample is hence composed of 22 participants with obesity and 30 healthy-weight participants as controls.
Demographical and bodily description
All the results relative to the participants are reported in Table 1.
Demographical information, body characteristics as measured in this study, and score at the Body Uneasiness Test.
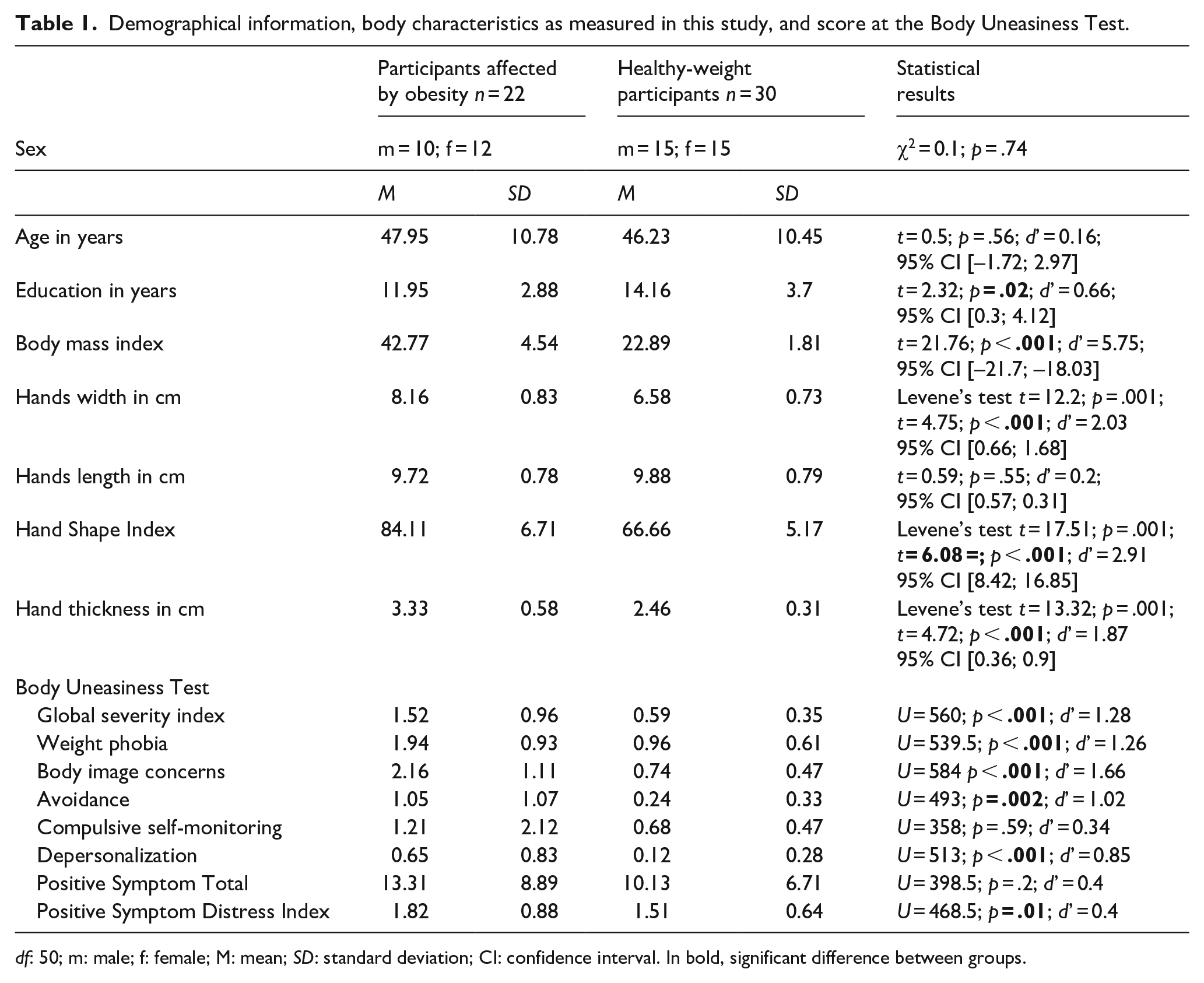
df: 50; m: male; f: female; M: mean; SD: standard deviation; CI: confidence interval. In bold, significant difference between groups.
The two groups did not differ in terms of Age, but they did for Education, in line with previous evidence (i.e., Scarpina et al., 2017; Tagini, Scarpina, Scacchi, et al., 2021). As expected, participants with obesity showed a higher BMI, as well as larger hand width and a larger hand shape index, as well as thickness, in comparison with controls. Thus, hand width and hand shape will be used in the analysis of motor imagery tasks as covariates if any difference between groups emerges.
Body uneasiness test
Scores at the questionnaire are reported in Table 1. Participants with obesity show higher scores in comparison with the normal-weight participants in almost all the scales, with the only exception of the Compulsive self-monitoring scale and the Positive Symptom Total. In other words, results suggested a higher level of body uneasiness in our participants with obesity.
Hand laterality task
In terms of outliers at the individual level, 4.36% answers of individuals with obesity and 4.61% of controls were removed as responses were above the cutoff of the two standard deviations, suggesting a lack of attention during the task. Means, standard deviations, and 95% CI are reported in the upper part of Table 2.
Mean (M), standard deviation (SD), and 95% confidence interval for the percentage of accuracy, reaction time in millisecond, and the efficiency score for the two groups (participants with obesity vs. healthy-weight participants) are reported for the implicit task (i.e., Hand Laterality Task) and the corresponding control task (i.e., Mental Letter Discrimination Task).
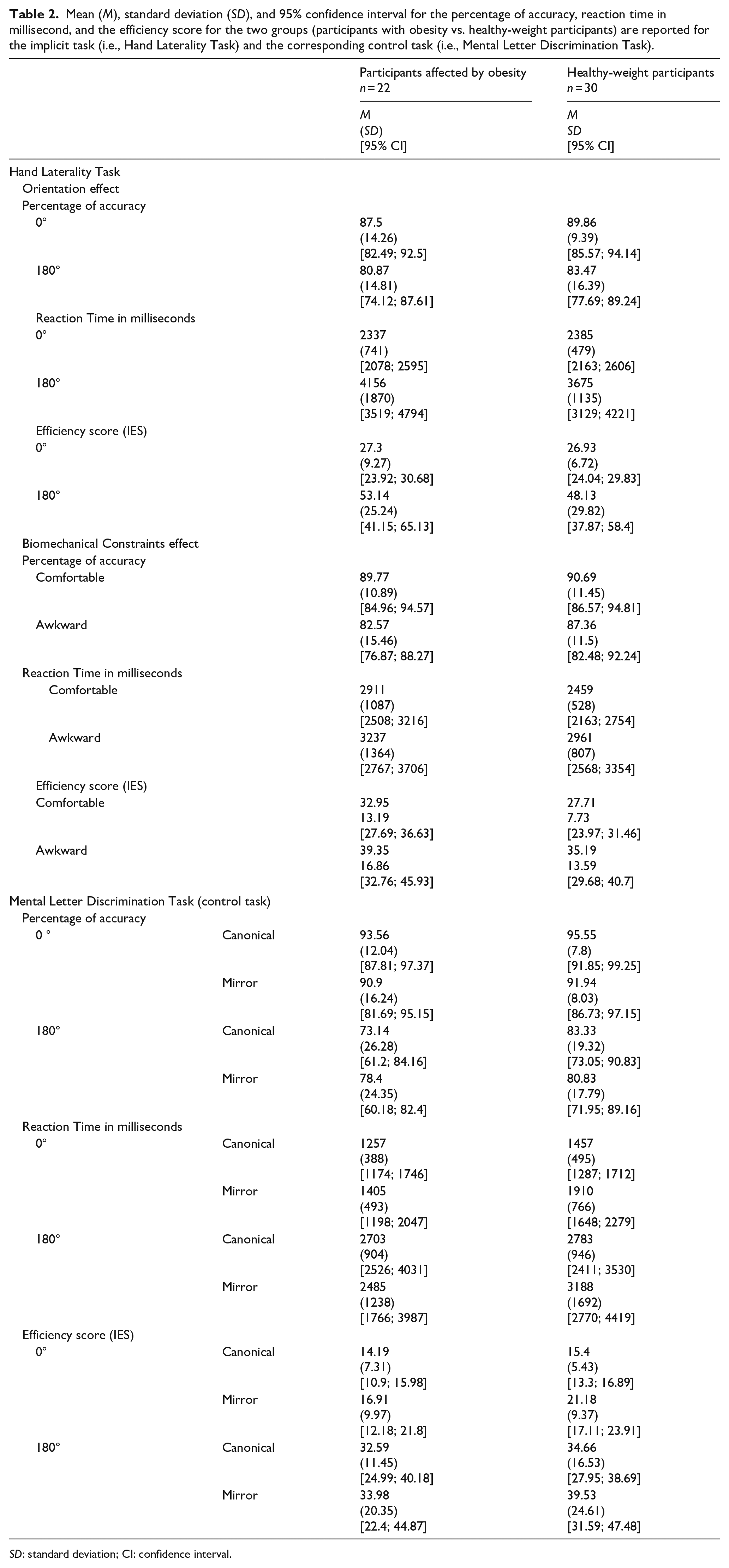
SD: standard deviation; CI: confidence interval.
Effect of stimulus orientation
For accuracy, a significant main effect of Orientation emerged, F(1,50)= 10.81; p = .002;
A significant main effect of Orientation emerged also for RT, F(1,50) = 96.34; p < .001;
When looking at the data considering the trade-off between accuracy and velocity, that is, the IES, the main effect of Orientation remained significant (stimuli at 0° M = 27.08; SD = 7.81; 95% CI [24.89; 29.34]; stimuli at 180° M = 50.25; SD = 27.83; 95% CI [42.70; 58.53]), F(1,50) = 46.1; p < .001;
Effect of biomechanical constraints
We found a significant main effect of Posture for accuracy, F(1,50) = 15.28; p < .001;
RT data showed a similar pattern, with a main effect of Posture, F(1,49) = 24.52; p < .001;
Considering the IES, a significant main effect of Posture emerged (comfortable M = 29.93; SD = 10.6; awkward M = 36.9; SD = 15), F(1,49) = 31.81; p < .001;
Mental motor chronometry task
Twelve percent of answers from the group affected by obesity and 5.02% from controls were removed because they were over or below the cutoff of the two standard deviations. Means, and standard deviations, and 95% CI are reported in the upper part of Table 3.
Mean (M) and standard deviation (SD) for the two groups (participants with obesity vs. healthy-weight participants) are reported for the Mental Motor Chronometry Task and the corresponding control task (Mental Bars Movement Task).
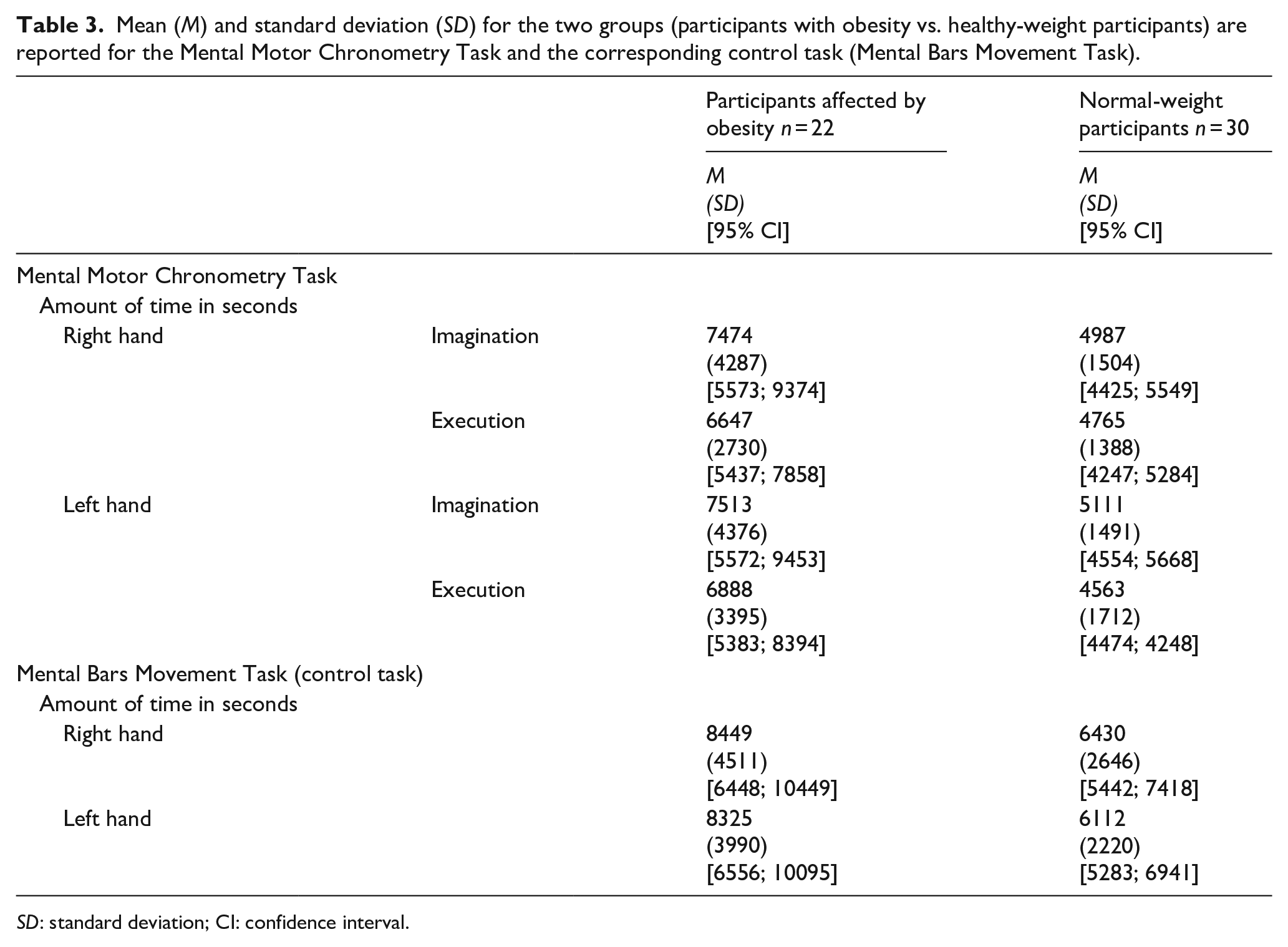
SD: standard deviation; CI: confidence interval.
Considering participants with obesity’s performance, a significant positive relationship between the time required to execute and to imagine the same movement emerged for the right, ρ(22)= 0.67; p < .001, and the left hand, ρ(22)= 0.58; p = .004 (Figure 1, upper part). Similarly, in healthy-weight participants, the significant positive relationship emerged for both the right, ρ(30)= 0.53; p = .002, and the left hand, ρ(30) = 0.88; p < .001 (Figure 1, lower part).
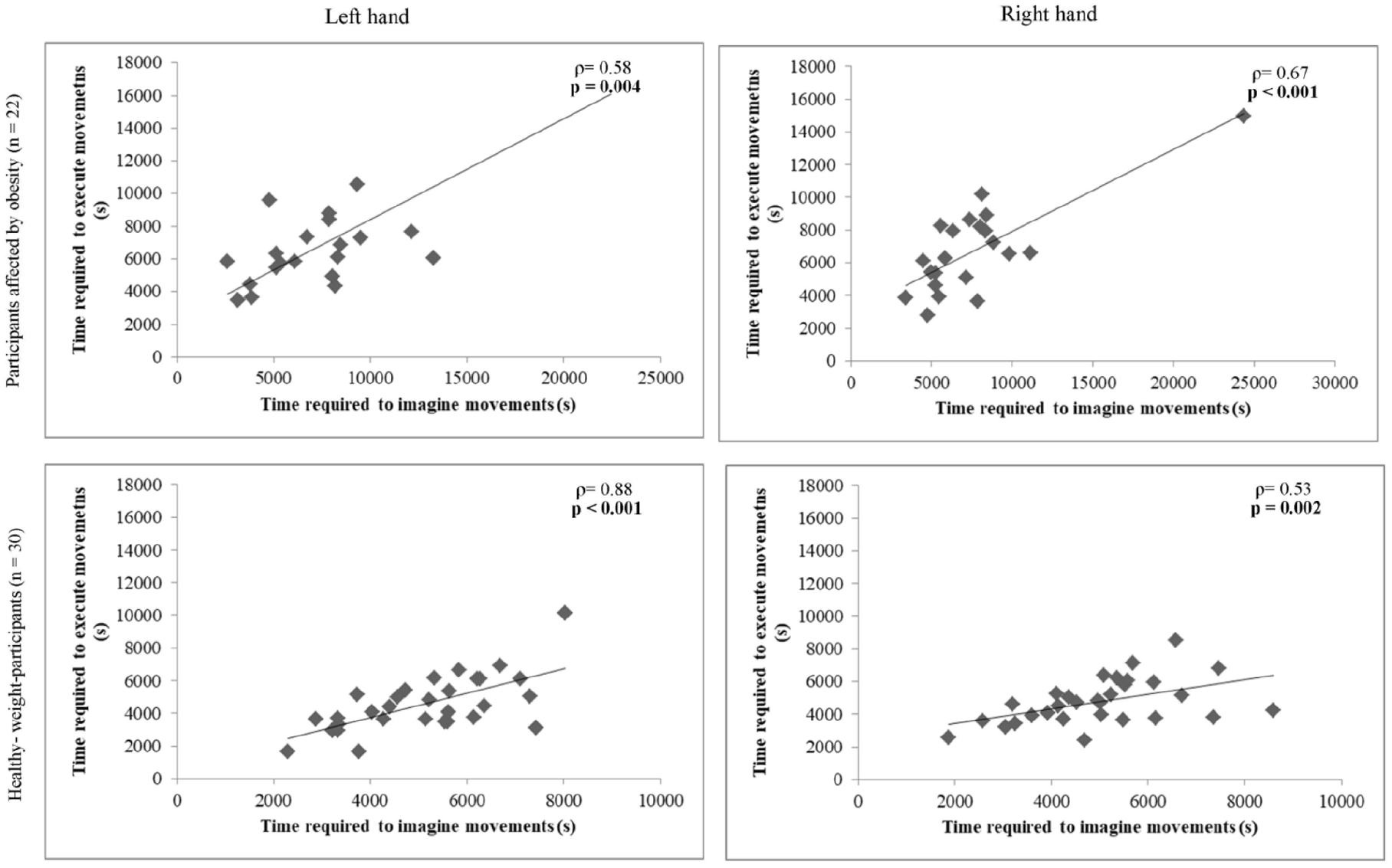
The relation between the time required to imagine movements (x-axis) and the time required to execute movements (y-axis) is shown for the right and the left hands for the two groups (participants affected by obesity vs. right-weight participants) for the Mental Motor Chronometry Task. Value of p in bold when <0.05.
According to Fisher’s analyses, there was not a significant difference between the two groups for the right hand (z = 0.74; p = .22). Differently, a significant difference emerged for the left hand (z =–2.38; p = .008): participants with obesity showed greater variability in the time required to imagine movements with the left hand (Figure 1).
Mental letter discrimination task
In terms of outliers at the individual level, 4.26% answers of individuals with obesity and 7.62% of controls were removed as responses were above the cutoff of the two standard deviations, suggesting a lack of attention during the task. Means, and standard deviations, and 95% CI are reported in the lower part of Table 2.
Considering accuracy, a significant main effect of Orientation emerged, F(1,46)= 22.08; p < .001;
About RT, we found a significant main effect of Orientation (stimuli at 0° M = 1535; SD = 614; 95% CI [1432; 1841]; stimuli at 180° M = 2826; SD = 965; 95% CI [2669; 3691], F(1,43) = 64.47; p < .001;
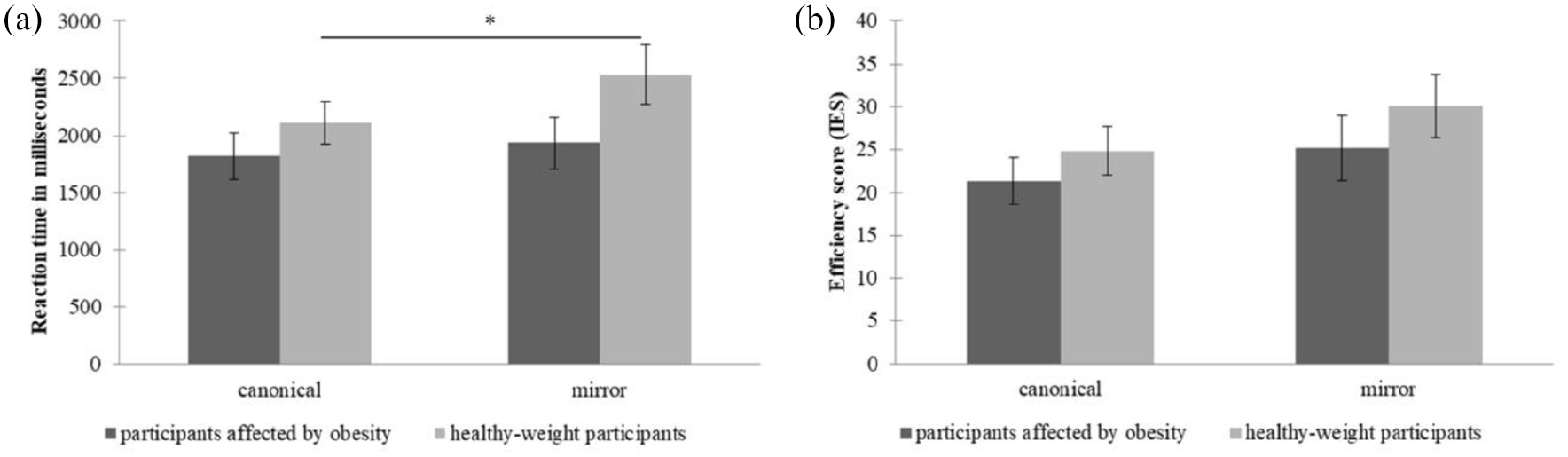
Mental letter Discrimination Task: mean (bars) and standard error (vertical line) for letters showed in canonical or mirror position (x-axis). (a) Reaction time in milliseconds (y-axis) is shown for the participants affected by obesity (dark grey bars) and healthy-weight participants (light grey bars). (b) Efficiency score (IES, y-axis) is shown for the participants affected by obesity (dark grey bars) and healthy-weight participants (light grey bars). * denotes a significant difference (p value < 0.05).
The interaction Group × Orientation × Type, F(1,43) = 1.5; p = .22;
Focusing on IES, we found a significant main effect of Orientation (stimuli a 0° M = 17.13; SD = 8.46; 95% CI [14.56; 18.75]; stimuli at 180° M = 35.67; SD = 19.51; 95% CI [29.64; 39.98]), F(1,40) = 83.65; p < .001;
Mental bars movement task
Means, and standard deviations, and 95% CI are reported in the lower part of Table 3. Both participants with obesity, ρ(22)= 0.87; p < .001 (Figure 3, upper part) and healthy-weight participants, ρ(30)= 0.98; p < .001 (Figure 3, lower part) showed a significant positive relationship between the time required to answer with the right hand and with the left hand.
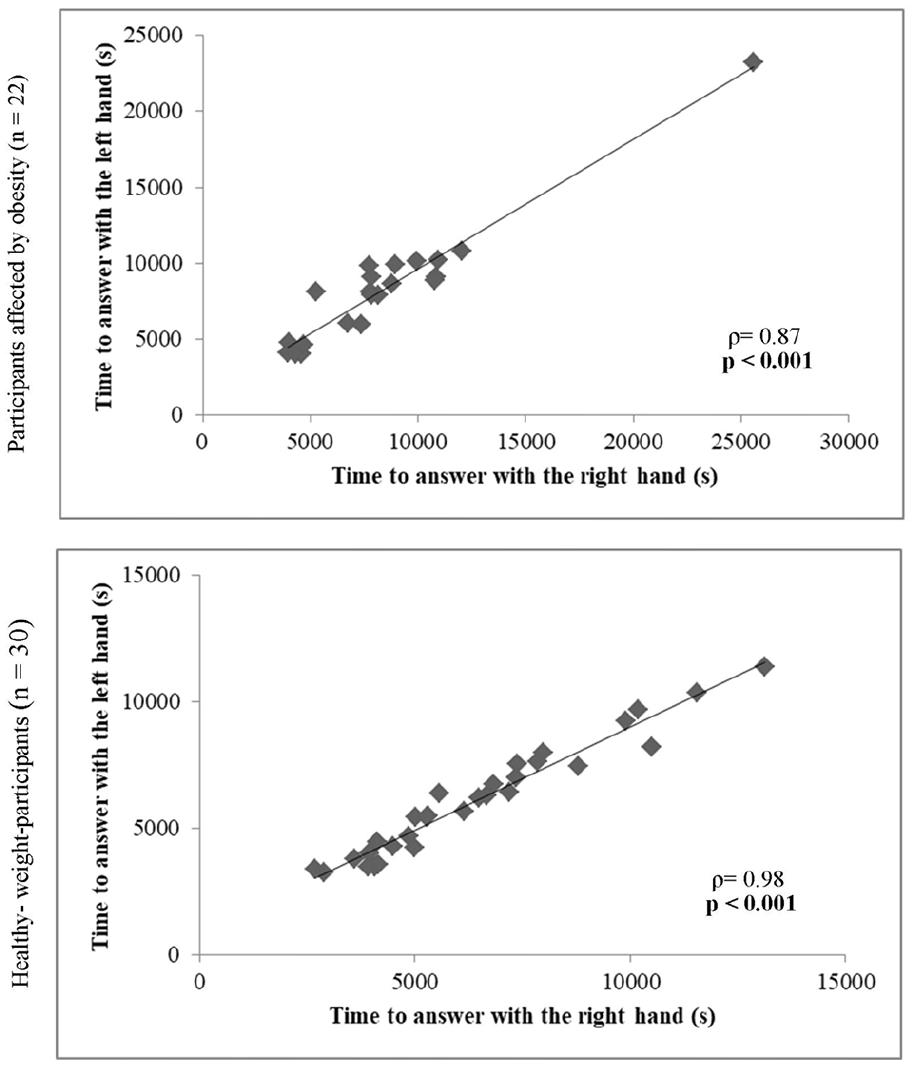
The relation between the time required to answer with the right hand (x-axis) and with the left hand (y-axis) is shown for the two groups relative to the Mental Bar Movements Task. Value of p in bold when <0.05.
According to Fisher’s analyses, a significant difference emerged between the two groups (z =−3.22; p < .001): a greater variability (i.e., larger time range) was shown by individuals with obesity (Figure 3).
Discussion
We aimed to investigate how participants with obesity perform at motor imagery tasks when different levels of awareness (Longo, 2015) are prompted by experimental instructions (Hétu et al., 2013), in comparison with participants with a healthy weight (Brusa et al., 2021; Scarpina, Magnani, et al., 2019, Scarpina et al., 2022). As an increased body weight seems to influence physical movement (i.e., Berrigan et al., 2006; Cimolin et al., 2011; D’Hondt et al., 2008; Scarpina et al., 2017; Teasdale et al., 2007), it is plausible that such an influence is mirrored in motor imagery. However, previous evidence available in the literature is not definitive and is scarce. Nevertheless, physical rehabilitation and motor activity, together with diet, play a crucial role in weight-loss treatment; thus, to what extent motor imagery skills are compromised in obesity might be a crucial component.
Differently from our hypothesis, we observed no difference between the two samples in the experimental tasks when hands were the target of the both more implicit and more explicit motor imagery processes. In more detail, in the Hand Laterality Task, both groups showed the effect of biomechanical constraints (Parsons, 1987; Sirigu et al., 1996): stimuli showing hands in a comfortable posture are processed faster and more accurate than in an awkward position. Interestingly, also in the Mental Motor Chronometry Task, both groups showed the expected effect: the time required to imagine a movement is correlated to the time required to perform the same movement. Overall, these results suggest an intact access to the representation of body in action in obesity.
In this study, we tested motor imagery in obesity considering the level of awareness (Brusa et al., 2021; Scarpina, Magnani, et al., 2019; Scarpina et al., 2022). Recently, Tagini, Scarpina, Scacchi, et al. (2021) showed that the distortions observed in individuals with obesity relative to the estimation of hand dimensions was comparable to normal-weight group, when such a judgement was performed implicitly. Although the authors did not test the explicit judgement, they hypothesise a role of awareness in accessing body representation to explain an altered body estimation in obesity according to Longo (2015). This hypothesis grounds on some previous evidence according to which individuals with obesity are generally less accurate in comparison with healthy-weight individuals in estimating the physical dimension of specific body parts, such as the abdomen or the shoulders (Scarpina et al., 2014; Schwartz & Brownell, 2004; Tagini, Scarpina, & Zampini, 2021). Following such a hypothesis, we might expect that any impact we had found of obesity on motor imagery would be more related would be more related to levels of awareness prompted by the task. However, we did not observe differences related to this component in our samples. Thus, these findings do not support the idea that motor imagery is impacted by awareness in obesity, or at least not in the tasks we used. In size judgements individuals are required to estimate a body part size by adjusting the space between two movable markers to match the estimated distance (Scarpina, Serino, et al., 2019), or between the hands/fingers (Kreitler & Kreitler, 1988); or they can be ask to draw a line (Scarpina et al., 2017) to mirror the physical extensions of body parts. Thus, not only the size judgements are explicit, since individuals are aware that they need to think of their own body representation to judge a body size (Longo, 2015), but also they require to use a non-bodily external reference: participants use an external support to make their estimations. On the other hand, in our tasks, both the (imagined or performed) movements as well as the laterality judgement rely on one’s own body perspective (Kosslyn et al., 1995), in an internal egocentric frame of reference. So, we might hypothesize that the different frame of reference (external vs. internal), more than the level of awareness required by the task enhances difficulties in obesity. This interesting hypothesis seems to be also supported by the fact that our results in this experiment contrasted with previous even though few evidence relative to the execution of real and imagined actions in obesity. In Guardia and colleagues (2013) and Scarpina and colleagues (2017), participants imagined to perform or performed, respectively, an obstacle-avoidance action (i.e., walking through door-like openings). Thus, as stated in the Introduction, authors tested actions in relation to an external object (i.e., the doors) that has to be avoided to prevent collisions. Instead, in our experiment, we tested exclusively an internal frame of reference, as the tasks did not require processing external objects. These fascinating results suggest us that in obesity altered body representation might emerge when actions are processed with an external frame of reference, when obstacles which are in the environment need to take into account.
A second interesting difference between our study and others is that we tested a single body part (i.e., the hand) action, although Guardia and colleagues (2013) and Scarpina and colleagues (2017) tested the whole-body actions. Previous literature, which focused largely on size estimation, is heterogeneous in terms of results on the whole body versus body parts. Individuals with obesity overestimate, underestimate, or are accurate in estimating whole body-size dimensions, although they are generally less accurate or show a comparable performance to healthy-weight individuals when they estimate the physical dimension of specific body parts (Schwartz & Brownell, 2004; Tagini, Scarpina, & Zampini, 2021). Our results seem to point towards a similar effect in individuals with obesity and healthy-weight individuals when body part actions are considered. One could then argue that testing hands movements is not sensitive enough to detect differences between the two groups. Notwithstanding that future research should explore motor imagery for the whole body to settle this debate, testing hands has been proven sensitive enough in other studies. For instance, paraplegic patients show an effect of a lower limb lesion on their upper body, as affordances effects are weaker and noisier for hands (Sedda et al., 2019). This is remarkable, as hands are not damaged in patients with paraplegia. Nonetheless, the effect is due to a different spatial frame of reference they are forced to adapt to. As such, the idea that testing hands does not provide enough sensitivity in obesity does not seem to hold. This is supported by the fact that this body part changes in its physical aspect because of the cutaneous fat, resulting in a higher shape in obesity, and it is evident also in our data.
In our study, participants with obesity have a preserved access to motor imagery, even though they scored significantly higher in terms of body uneasiness (Cuzzolaro et al., 2006). Specifically, our participants are highly worried of weight gain and of physical appearance; also they show avoidance behaviours. Our results do not support the idea of Irvine and colleagues (2019), who showed that the passability judgement between two sliding doors, similarly to what proposed by Guardia and colleagues (2013), is altered in healthy-weight individuals with more negative bodily attitudes and low self-esteem. The authors hypothesised that negative feelings, associated to an overestimation of the physical body size (especially for those body parts that are more susceptible to be enlarged because of adiposity) impact the sensory and proprioceptive input, influencing the updating of the stored body representation for movements (Irvine et al., 2019). However, the authors did not test real movements: participants performed a judgement about an imagined movement. On the other hand, Glashouwer and colleagues (2019) showed that in the case of real passing through an aperture performed by healthy-weight individuals, the negative body image was unrelated to the behaviour (i.e., the aperture/shoulder width turning ratio), mirroring the results obtained by Scarpina and colleagues (2017) about obesity. Our findings as well as those from Glashouwer and colleagues (2019) and Scarpina and colleagues (2017) suggest that the link between body satisfaction and actions (imagined or performed) is not so crystal clear. One could argue that the link lies in imagining; however, since we tested both components, this seems an unlikely explanation.
In addition to motor-related tasks, we also tested visual imagery, in which objects instead of hands are the target (Brusa et al., 2021; Scarpina, Magnani, et al., 2019; Scarpina et al., 2022). Previous studies investigating mental imagery in obesity are very rare and focus on children (Jansen et al., 2011) and adolescents (Kaltner et al., 2017), but they agree in reporting cognitive difficulties in spatial tasks. No previous study investigated mental imagery in adults; however, previous evidence has indicated that obesity is associated with decreased cognitive performance (Liang et al., 2014; Prickett et al., 2015; Wang et al., 2016). For example, among the cognitive difficulties investigated, affected individuals show reduced visuo-spatial-constructional performance (Boeka & Lokken, 2008; Lokken et al., 2010). This evidence, even though limited to neuropsychological tests, suggests to verify visual imagery abilities in this population, as motor imagery is related to visual imagery skills and can be influenced by deficits in the latter function. Thus, in our control tasks, individuals were required to perform an object-based transformation, in an allocentric reference frame, with no bodily reference. When we focused on the explicit control task, the Mental Bars Movement Task, both groups of participants showed the expected experimental effect, meaning that the time taken to answer with the right hand and with the left hand matched (Brusa et al., 2021; Scarpina, Magnani, et al., 2019). In the more implicit Mental letter Discrimination Task, the experimental effect according to which stimuli showed in a canonical position should be recognised faster than those showed in mirror position was present only for our healthy-weight controls, while participants with obesity showed the same reaction time for mirror and canonical stimuli. Interestingly, their reaction time was overall faster in comparison with the performance of normal-weight participants. We might interpret our data as a result of cognitive comprising: a faster reaction time linked to the difficulties in cognitive impulsivity and response inhibition reported in obesity (Guerrieri et al., 2009; Kollei et al., 2018; Nederkoorn et al., 2006). However, considering that no difference emerged between groups in the IES analysis (Townsend & Ashby, 1983), we can conclude that such an impulsive behaviour cannot be the underlying cause of the difference. As our study was not designed to rule out the mechanism or process responsible for any difference in visual imagery in obesity, we provide the first evidence of an overall efficient visual imagery process in obesity but highlight a difference that is worth further investigation.
The status of our physical body impacts how we see it in our mind. Obesity is a condition that dramatically impacts on the physical body. Moreover, difficulties in mobility and motor disability experienced by affected individuals are generally associated with reduced health-related quality of life (Forhan & Gill, 2013). On the other hand, physical activity together with a correct eating behaviour is crucial in preventing obesity (Fogelholm & Kukkonen-Harjula, 2000; Wareham et al., 2005). Despite these challenging elements of obesity, our study provides the evidence that not every aspect of body representation is impacted. Accessing the representation of bodily-centred actions, or motor imagery, is spared in individuals with obesity, in both its explicit and implicit cognitive components. As such, our findings suggest that treatments for mobility and motor disability based on motor imagery exercises should not be avoided in individuals with obesity, as they have the necessary cognitive resources to benefit from such an approach.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.