
Abstract
Background:
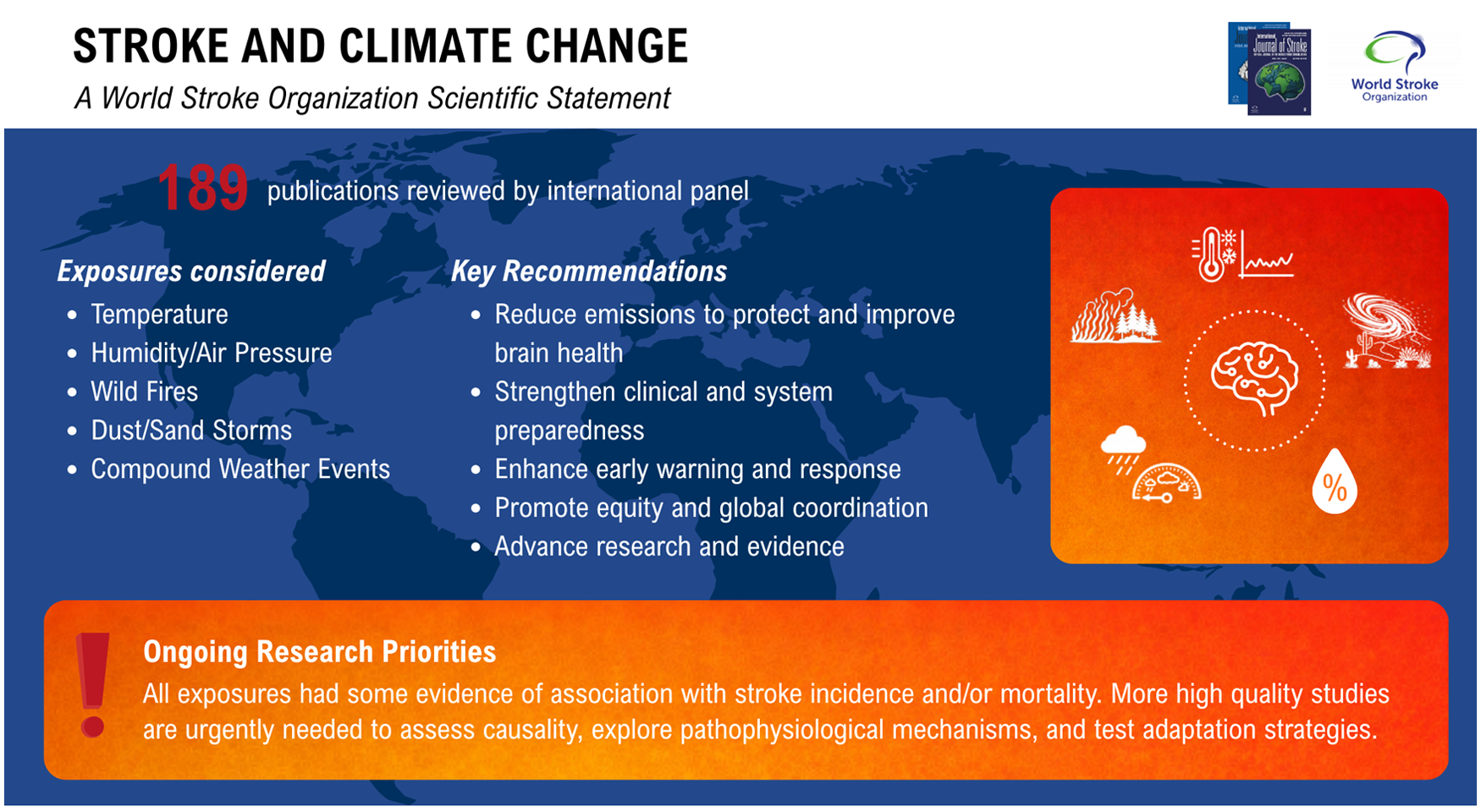
Climate change poses an escalating threat to global brain health and is increasingly linked to stroke incidence, outcomes, and inequities in prevention and treatment. This World Stroke Organization scientific statement summarizes current evidence on the associations between stroke and the environmental variables exacerbated by climate change, with a focus on risk and outcomes.
Methods:
We systematically identified and reviewed published studies assessing associations between stroke and environmental variables, including extreme temperatures, temperature variability, humidity, barometric pressure, wildfires, dust and sandstorms, and compound weather events. Air pollution, unrelated to wildfire exposure, was excluded, as a subsequent statement will focus on this. Paired reviewers screened titles and abstracts. Full texts were evaluated for study design, sample size, geographic context, and strength of evidence, with attention to impacts on vulnerable populations where data were available. Study type, exposure assignment, and strength of evidence were further confirmed by a team member with Master’s level qualification in epidemiology.
Results:
Most of the included studies were based on ecological designs. Cold exposure, temperature variability, and extreme thermal events were most consistently associated with increased stroke risk. Although cold effects were generally stronger than heat effects, heat effects have been increasing over time. Increased stroke incidence was also associated with low or varying barometric pressure, rapid humidity shifts, and exposure to wildfire smoke, dust, and sandstorms, particularly among older adults and those in low- and middle-income countries. Compound weather events, such as concurrent heat and humidity extremes, showed additive or synergistic effects on stroke incidence and mortality. Despite heterogeneity in definitions and methods and most evidence supporting associations rather than proving causation, the overall direction of evidence across exposures was positive, coherent, and biologically plausible.
Recommendations:
Advancing mitigation efforts that reduce greenhouse gas emissions is essential, since limiting further climate change directly decreases the environmental drivers of stroke risk and protects long-term population brain health, along with broader climate-related health risks. Stroke professionals and organizations can meaningfully contribute through local, regional, and global advocacy. Climate-related environmental variables already meaningfully increase stroke risk and exacerbate existing health inequities. To further counter these trends, stroke prevention and care systems should integrate climate risk awareness, patient education, and early-warning mechanisms into clinical practice and health system planning. Priority areas include targeted protection for vulnerable groups, standardized exposure metrics, longitudinal surveillance, systematized education on climate change’s impact on brain health, and expansion of research in underrepresented regions. Strengthening global collaboration and embedding climate resilience into stroke systems of care are critical for reducing both stroke-related morbidity and the wider health impacts of a climate-impacted world. This scientific statement has been reviewed and approved by the WSO Executive.
Keywords
Purpose
The purpose of this scientific statement is to inform the scientific and clinical stroke community on how environmental variables associated with climate change impact stroke risk and outcomes. Greenhouse gases, such as carbon dioxide and methane, drive global warming and indirectly increase climate-related stroke risk. Observational studies show that other climate-driven changes, including greater temperature variability, altered humidity and pressure patterns, more frequent extreme weather events, and increasing wildfire and dust and sandstorms also increase stroke risk. The interrelation of these factors can result in compound weather events that can have synergistic impacts. This statement aims to synthesize current evidence on these variables, support strategies to mitigate the climate-related stroke burden in the general population, address disproportionate effects on vulnerable groups, inform equitable adaptation measures at both individual and system levels, and guide future research.
Introduction
Stroke remains a leading cause of global morbidity and mortality, with 89% of this burden occurring in low- to middle-income countries (LMICs). 1 Climate change is a novel, yet widely recognized and modifiable environmental and social determinant of health per the World Health Organization, which is rapidly becoming the pre-eminent threat to global public health through a range of complex pathways. 2 Among environmental contributors to stroke, indoor and outdoor air pollution are already identified in the World Stroke Organization’s (WSO) Global Stroke Fact Sheet. Air pollution accounts for 28% of global stroke disability-adjusted life years (DALYs), second only to hypertension as the largest modifiable risk factor. 1 Climate change and air pollution share a common driver in the burning of fossil fuels, which produces both greenhouse gases and many of the pollutants that determine indoor and outdoor air quality.
Outdoor air pollution, also known as ambient air pollution, is a well-established, modifiable risk factor for both incident stroke and adverse stroke outcomes. 3 Short-term exposure to fine particulate matter (PM2.5) and gaseous pollutants such as NO2 and SO2 is associated with increased risk of acute stroke onset within hours to days, likely mediated through systemic inflammation, endothelial dysfunction, autonomic imbalance, hypercoagulability, and blood pressure elevation. Long-term exposure contributes to accelerated atherosclerosis, increased carotid plaque burden, and higher rates of both ischemic and hemorrhagic stroke. Air pollution is also associated with worse stroke severity, larger infarct volumes, higher in-hospital mortality, and poorer functional recovery, with disproportionate impacts observed in low-income populations and regions with higher baseline exposure levels.
In addition to worsening air pollution, several weather-related environmental exposures, including extreme heat, temperature variability, humidity and barometric pressure changes, and severe weather events, are becoming more frequent or intense as climate change alters the distribution of these conditions. 4 The public health literature aptly frames climate change as a “quintessential meta problem and threat multiplier.” 5 Studies exploring the association between stroke and environmental factors like temperature, barometric pressure, and humidity have rapidly increased in recent years within the scientific literature.6–9 This scientific statement summarizes and interprets the current evidence on climate change’s impact on stroke incidence and outcomes to apprise the stroke community and inform stroke advocacy campaigns, education, research, and systems of care in incorporating these growing risk factors into prevention and mitigation strategies.
A foundational understanding of the distinctions between weather and climate is critical for clinicians and scientists, as these environmental dynamics increasingly shape stroke risk. Weather refers to the state of the atmosphere at any point in time, whereas climate refers to the long-term average of weather conditions over the course of decades. In this context, climate may describe both the average temperature that a region experiences and the probability of specific weather events, such as heat waves. Climate change occurs when these long-term averages and probabilities are altered. Although natural variation exists within the climate system, this differs fundamentally from the large-scale changes currently being driven by human activity. The Intergovernmental Panel on Climate Change (IPCC) has concluded that it is “unequivocal” that the atmosphere has warmed due to human influence, particularly from greenhouse gas emissions. The use of such strong language reflects the weight of scientific evidence linking human activity to global warming.
For context, the decade 2011–2020 was approximately 1.1°C warmer than the 1850–1900 baseline. Projections estimate a 1.4°C–4.4°C increase in global mean temperature by the end of this century, depending on the emissions trajectory followed. 10 Although a few degrees of average warming may seem modest or even harmless from a health perspective, it drives substantial systemic changes in the climate, and the average masks the far more consequential extremes. A more energetic (i.e. warmer) climate system increases the frequency and intensity of extreme thermal events, with more extreme heat events and fewer extreme cold events already being observed and expected to increase over time. 11 Climate change is intensifying the extremes of both wet and dry conditions, raising temperatures, and increasing wind speeds, and together, these shifts are driving more frequent wildfires. These same forces are expanding the geographic range in which wildfires can occur and prolonging the duration of wildfire seasons, resulting in larger populations being exposed to its health impacts over longer periods of time.
In parallel, warming alters the global water cycle. A warmer atmosphere retains more water vapor and accelerates land-surface evaporation, producing greater risks of both drought and extreme rainfall events. Changes in humidity patterns have also been observed, with absolute humidity rising while relative humidity declines.12,13 Low barometric pressure systems are linked to storms, the intensity of which is considered likely to increase in some locations as a consequence of climate change. 10 Beyond these direct effects, a warming climate influences broader systems relevant to stroke risk. This ranges from changes in large-scale climate variability (e.g. the Indian Monsoon, El Niño Southern Oscillation), to worsened air quality (e.g. wildfire smoke and near-surface ozone production) and downstream impacts such as food insecurity, nutrition and diets, water-borne illness, and vector-related disease transmission. Collectively, these climate change-driven changes represent emerging amplifiers of existing diseases and modifiers of social determinants of health. For a comprehensive synthesis of climate change science, readers are encouraged to refer to the most recent IPCC synthesis report as well as a recent topical review on climate change and stroke. (IPCC 2023), 14
Methodology
An international panel was convened comprising expertise in climate change, climate medicine, and stroke specialists from Asia, Europe, Middle East and North Africa, North and South America, and Oceania. This approach was taken to bring together diverse perspectives and to show both the shared and region-specific pathways through which climate-related factors influence stroke incidence and risk, reflecting how climate conditions and the impacts of climate change differ across the world. Both the commonalities and disparities found in distinct regions highlight the importance of international perspectives and collaboration to advance research and inform policies that address how climate change will continue to influence global stroke risk. Several climate variables were identified for exploration: ambient levels, rapid variations, and extremes of temperature, humidity, and barometric pressure, along with compound weather events, wildfires, and dust storms as prominent climate-related drivers of stroke (Figure 1).
Potential climate change-related stroke risk factors.
Compound weather events are situations where multiple meteorological factors occur together or in close sequence, producing combined or amplified impacts that may be greater than any single factor alone (e.g. heat and low barometric pressure together). Dust and sandstorms (DSSs) are natural contributors to the particulate air-pollution mix, adding large amounts of coarse and sometimes fine mineral particles to ambient air. Dust consists of smaller particles that travel farther and penetrate deeper into the respiratory tract, while sand is heavier, more localized, and contributes mainly to coarse particle loads. Their health effects are thought to arise through airway inflammation, oxidative stress, and systemic inflammatory responses that increase thrombosis risk and cardiovascular strain.
We searched Embase and Medline on 3 January 2025, and Scopus on 21 January 2025 using the following search terms: (Ambient temperature*/temperature varia*/temperature extreme*) AND stroke; (Barometric pressure/atmospheric pressure/humidity) AND stroke; Wildfire* AND stroke; (Dust storm*/sandstorm*) AND stroke; (Compound weather event*/compound climate*) AND stroke.
Air pollution that was not related to wildfire exposure was excluded because it will be addressed in a separate statement. Atmospheric pressure and barometric pressure are synonymous, and so their data were combined. Given that several studies examined humidity and barometric pressure as co-variables, the literature from these two topics was combined. Due to the similarity and the very low number of studies on sandstorms and dust storms, they were also combined.
Titles and abstracts were assigned to two authors who separately selected papers first for abstract and then for full review; any discordant responses were adjudicated by a third author. Selected papers that were duplicated across topics or examined multiple variables, such as humidity and temperature, were assigned to the most relevant topic. Papers selected for full review were then categorized by reviewers as either (1) original research papers, (2) review papers, or (3) excluded.
Papers were excluded if the full article could not be sourced (n = 46), no stroke outcomes were reported (n = 15), were not about the designated risk factor (n = 15), were outdated (n = 6), had no quantitative data (n = 3), were not in English (n = 3), had sample sizes that were too small (n = 2), or were an opinion piece (n = 1). The study design of the original studies was ecological (n = 133), case cross-over (n = 28), case only (n = 4), cohort (n = 4) or randomized control (n = 1). Most reviews were systematic reviews (n = 8) or meta-analyses (n = 4). Studies came from many places around the globe, but predominantly from China and high-income countries (Figure 2).
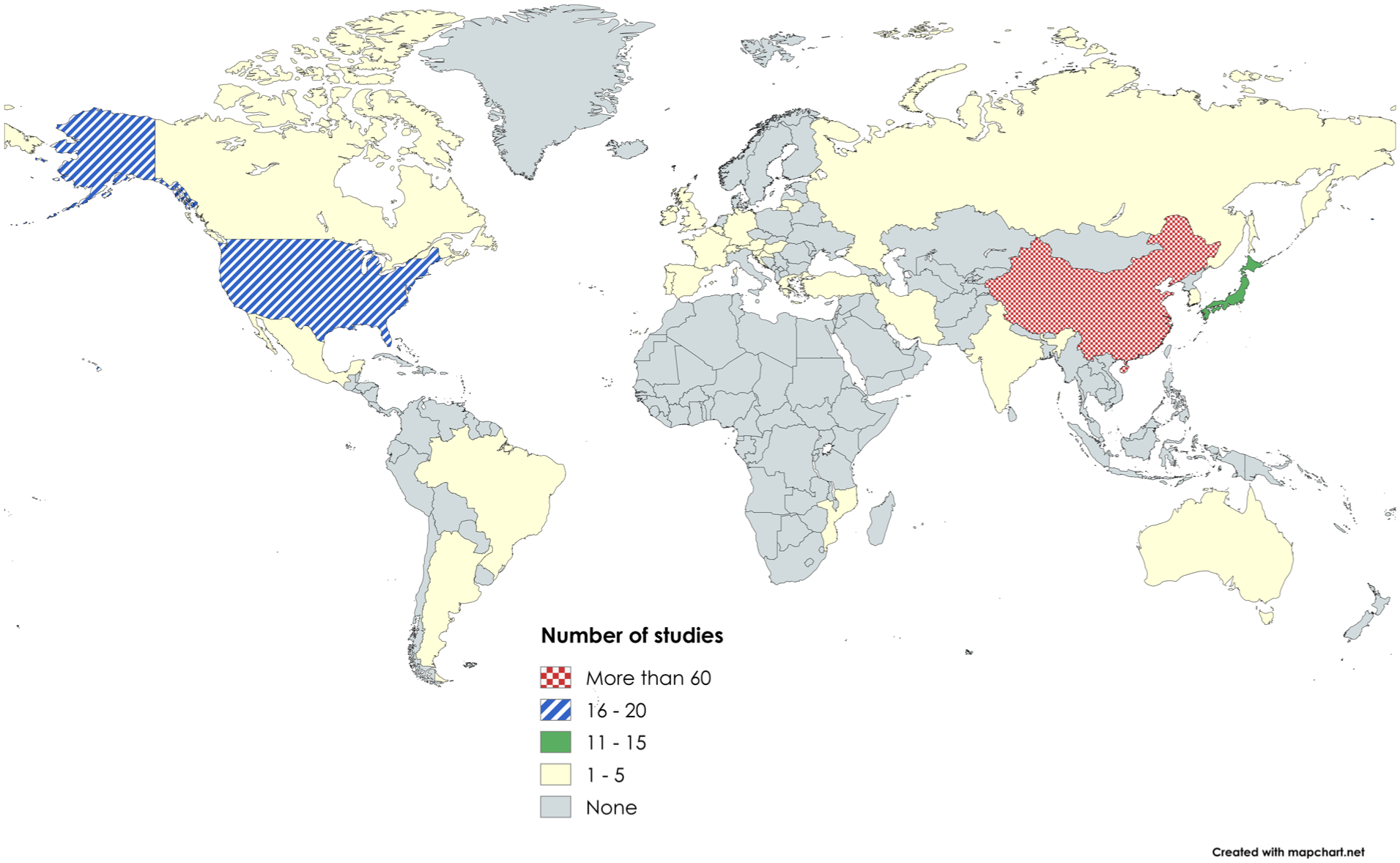
Countries where original studies were conducted (created by mapchart.net).
Paired reviewers screened titles and abstracts. Full texts were evaluated for study design, sample size, geographic context, and strength of evidence, with attention to impacts on vulnerable populations where data were available. All reviewers have expertise in study design, data analysis, and result interpretation. Study type, exposure assignment, and strength of evidence were further confirmed by a team member with Masters’ level qualification in epidemiology. The number of titles, abstracts, and full texts reviewed by topic are summarized in Table 1. Information about specific information extracted from original and review papers are summarized in Supplemental Tables 1 and 2, and all included full-text papers are summarized by topic in Supplemental Tables 3–12.
Number of papers selected for review.
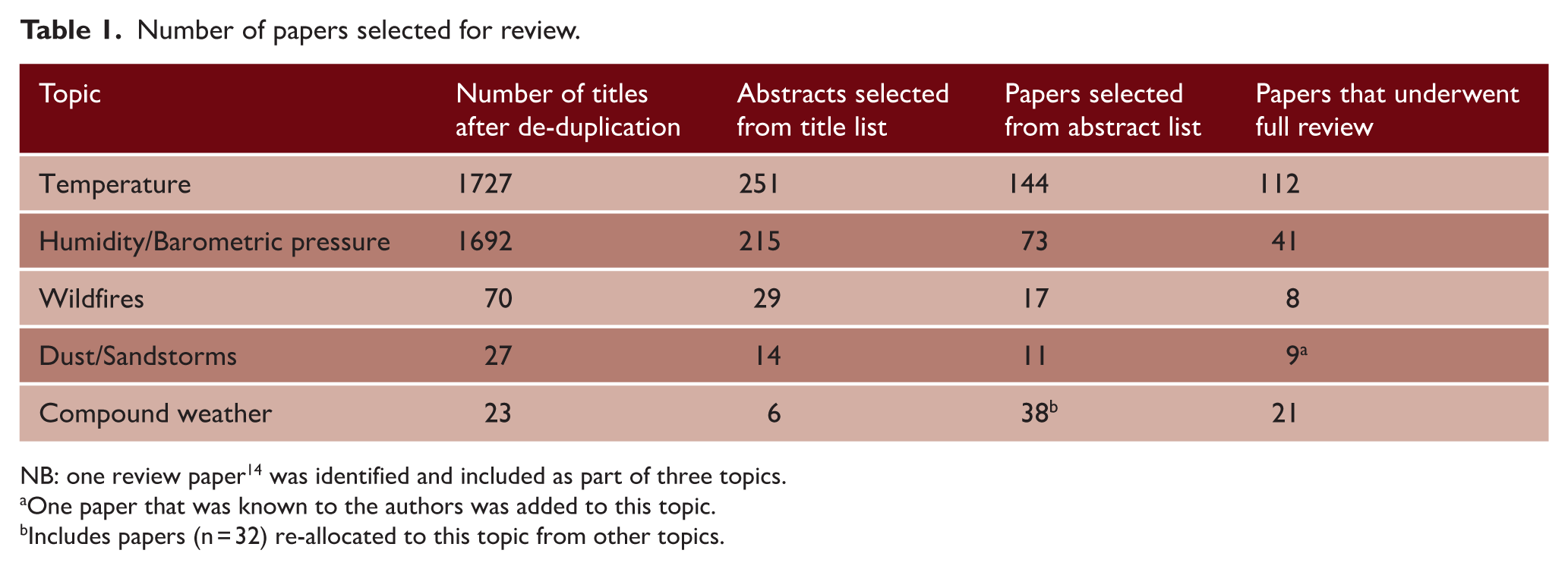
NB: one review paper 14 was identified and included as part of three topics.
One paper that was known to the authors was added to this topic.
Includes papers (n = 32) re-allocated to this topic from other topics.
The results are organized by five climate variables, each with subsections covering the suggested mechanism, total stroke findings, ischemic stroke findings, hemorrhagic stroke findings, and a brief synthesis of the evidence for that variable.
Results—climate variables and stroke
Temperature
Suggested mechanism
Cold exposure and rapid temperature swings increase blood pressure, sympathetic tone, hypercoagulability, and endothelial stress, while heat causes dehydration and hemoconcentration; together, these disrupt cerebrovascular stability and raise ischemic and hemorrhagic stroke risk.
Study characteristics
A total of 97 original studies evaluating the impact of temperature on stroke were reviewed. Among the included studies, 69 employed the ecological design, 21 used a case crossover design, seven were cohort studies, four were case-only studies, and one was a randomized controlled trial. Nearly half (44%) originated from China, followed by 12 from the United States, six from Japan, and four from Brazil, with only one or two studies from other countries. Four additional multi-national studies contributed particularly robust evidence because of their large sample sizes and diverse populations. Among these, 33 investigations assessed all stroke types combined, 23 examined ischemic and hemorrhagic stroke together, and 21 focused solely on ischemic stroke. Another 11 studies included ischemic, hemorrhagic, and subarachnoid hemorrhage, while the remainder evaluated various combinations of ischemic stroke, hemorrhagic stroke, and TIAs. Collectively, these studies explored a broad range of cerebrovascular outcomes, including stroke incidence, hospital admissions, emergency visits, mortality, onset timing, severity, and years of life lost, to characterize how heat, cold, and temperature variability influence both acute stroke events and overall stroke burden.
Studies including multiple or unspecified stroke subtypes
Across large-sample studies, stroke risk was linked to cold, heat, and temperature variability, with the most consistent patterns showing higher admissions during colder conditions and periods of marked temperature variation. In a multi-city analysis from China, non-optimum temperatures accounted for a substantial share of total stroke mortality (12.41%, 95% confidence interval (CI) = 8.81–15.07), including 5.75% attributable to cold and 6.67% to heat, both statistically significant. 15 A Japanese meta-regression of more than 4.5 million hospitalizations found that colder ambient temperatures increased total stroke admissions (risk ratio (RR) = 1.107, 95% CI = 1.062–1.155) using a percentile-based cold metric. 16 National Brazilian data involving more than 1.4 million hospitalizations similarly showed higher admission rates at lower temperatures (Spearman ρ ≈ 0.49). 17 In Ontario, an analysis of more than 355,000 admissions reported elevated total stroke hospitalizations on cold days (RR = 1.11, 95% CI = 1.01–1.20), with no significant heat-related effect. 18
In Jiangsu Province, China, heat waves defined by high percentile thresholds over consecutive days were associated with substantially elevated stroke mortality, yielding odds ratios (ORs) around 1.19 (95% CI = 1.17–1.21) for typical definitions and similarly increased risks for more intense multiday events. 19 A large London time series found a marked increase in stroke admissions at the 99th percentile of nighttime temperature, with a relative risk of 1.70 (95% CI = 1.32–2.19) compared with the optimum. 20 A systematic review reported that men and older adults in Central Asia bore a disproportionate burden of stroke mortality attributable to extreme cold, although this burden has declined over the past three decades, 21 and that low-GDP countries faced higher mortality risks from both extreme heat and cold, with cold contributing the greatest excess deaths. 22
Temperature variability independently contributed to risk. In a 272-city analysis in China, each unit increase in temperature variability was associated with small but consistent increases in cause-specific stroke mortality (0.86%, 95% CI = 0.55–1.18). 23 These effects may have been stronger in vulnerable groups; for example, a cold-temperature study enriched for women and individuals older than 70 found amplified risk of stroke mortality among those under 80 and among people with hyperglycemia (OR) = 1.076, 95% CI = 1.023–1.131). 24 Evidence from Maputo, Mozambique reinforces this pattern in sub-Saharan Africa, where 10-day drops in minimum temperature were linked to a 31% rise in stroke admissions (RR = 1.31, 95% CI = 1.09–1.57) and 5-day drops to a 22% rise (RR = 1.22, 95% CI = 1.01–1.46). 25 In Yancheng, China, stroke risk increased sharply at both temperature extremes, with extreme cold (−1.3°C) associated with a relative risk of 1.88 (95% CI = 1.28–2.78) and extreme heat (30.5°C) with a relative risk of 1.48 (95% CI = 1.26–1.74) compared with an optimum of 24.4°C. 26 Importantly, there was evidence that mitigation measures may be effective. One study found that every additional 10 days of central heating was linked to a small reduction in cold-related mortality risk (RR = 0.98, p < 0.001). 27
Ischemic stroke
For ischemic stroke specifically, the largest and most informative data sets indicated increased risk from both cold exposure and temperature variability, with the clearest signals appearing in hospital-based outcomes. In a nationwide US sample of roughly 170,000 admissions, each 2.8 °C rise in diurnal temperature variation increased hospitalization odds by 5–37% in adults ages 18–64 (OR = 1.05–1.37) and by 9–20% in those 65 or older (OR = 1.09–1.20), with spring showing the strongest effects. 28 A multi-country analysis reported substantial contributions of extreme temperatures to ischemic stroke mortality, estimating 9.1 and 2.2 excess deaths per 1000 ischemic stroke deaths from cold and heat, respectively. 29 Large multi-city time-series studies in China likewise identified elevated ischemic stroke mortality at both temperature extremes,23,30 and considerable attributable fractions linked to non-optimum temperatures were concentrated in moderate cold. 15
For acute care specifically, temperature variability was associated with higher emergency department (ED) visits in a US data set comprising 12 million encounters (RR = 1.03, 95% CI = 1.02–1.05 per variability unit). 31 Additional regional analyses showed similar patterns: in California, ischemic stroke ED visits increased by about 2.8% per −12.22°C rise in ambient temperature; 32 in Boston, a 5°C drop in apparent temperature over 2 days yielded an incidence rate ratio of 1.09 (95% CI = 1.01–1.18), with slightly stronger effects under high-humidity conditions (Incidence Rate Ratio (IRR) = 1.11, 95% CI = 1.00–1.23). 33
Hemorrhagic stroke
For hemorrhagic stroke, large mortality data sets consistently implicated non-optimum temperatures, with cold exerting the stronger effect. In a previously cited study, hemorrhagic events showed marked cold sensitivity, with relative risks near 1.50 (95% CI = 1.07–2.09) compared with about 1.32 (95% CI = 0.98–1.78) for ischemic stroke. 34 Another analysis estimated 11.2 excess deaths per 1000 hemorrhagic stroke deaths attributable to cold and 0.7 attributable to heat, with heat effects most pronounced in low-GDP countries. 29 A Chinese study that analyzed ischemic and hemorrhagic subtypes separately similarly found that cold accounted for a larger share of hemorrhagic stroke mortality than heat, with attributable fractions of roughly 11% versus 1%. 35 Short-term analyses from New York showed a contrasting pattern, with ischemic stroke rising by about 5.1% per 10°C increase over 7 h, while hemorrhagic stroke fell by roughly 6.2% per 10°C increase over 5 h. 36
Summary
Taken together, the largest and most methodologically rigorous studies showed that cold exposure has the most consistent and substantial impact on hemorrhagic stroke, particularly mortality. Heat-related effects, in contrast, are smaller, less stable across settings, and highly context dependent. Temperature variability may contribute additional risk, although its influence on hemorrhagic events was generally weaker than on ischemic outcomes. Overall, hemorrhagic stroke demonstrated stronger and more consistent associations with cold exposure, rapid temperature declines, and temperature instability than ischemic stroke.
Humidity/barometric pressure
Suggested mechanism
Low or varying barometric pressure and rapid humidity shifts destabilize cerebral hemodynamics, alter vascular tone, and increase blood pressure variability, creating conditions that favor thrombosis or vessel rupture.
Study characteristics
A total of 39 original studies examining the effects of humidity and/or barometric pressure were identified. All of these were ecological studies. These investigations spanned a broad geographic range, including China, Taiwan, Japan, several European countries, the United States, and the Middle East, with only one or two studies from most regions. Most studies assessed all stroke types combined, while some focused on one subtype. The outcomes evaluated were similarly diverse, ranging from daily stroke incidence and hospital admissions to emergency calls, mortality, and stroke subtype-specific patterns.
Studies including multiple or unspecified stroke subtypes
Multiple, large, population-based studies reported higher rates of overall stroke hospitalization during periods of low absolute barometric pressure and barometric pressure variability. In one study of more than 4000 patients, days with pressure departures from the monthly mean were associated with a 49% increase in stroke hospitalizations (RR = 1.49, 95% CI = 1.14–1.96). 37 Another study involving 607 patients found nearly a threefold increase in admission odds under low-pressure conditions (OR = 2.95, 95% CI = 1.42–6.14; p = 0.012). 38 Humidity effects were also positively associated; a Japanese analysis showed a 50% rise in ambulance transports with large humidity shifts (RR = 1.50, 95% CI = 1.08–2.11). 39 Consistent findings from Spain reported about a 6.5% rise in all stroke admissions for each 20% decrease in relative humidity, again highlighting the vascular impact of rapid humidity changes. 39 In Shenzhen, China, heat and low barometric pressure together accounted for an estimated 1.95% of first-ever strokes (95% empirical CI = 0.63–3.20%). 40
One study found that low pressure-related stroke admissions were stronger in younger adults, with RR = 1.027 (95% CI = 1.008–1.047) for patients <65 years versus RR = 0.966 (95% CI = 0.936–0.997) for those ⩾65 years. 41 Similarly, older hypertensive outpatients ⩾65 years with no prior stroke had markedly higher rates under low air pressure, with HR = 2.831 (95% CI = 1.752–3.232) for the composite outcome, including stroke hospitalizations. 42 Collectively, stroke incidence and hospitalizations rose during low-pressure conditions and pressure variability and when humidity is high or rapidly changing. Time-series data from Moscow found that a 10°C rise in daily mean temperature increased stroke risk by 16% (RR = 1.16, 95% CI = 1.02–1.30), and large barometric pressure swings 5 days earlier were associated with a relative risk of 1.65 (95% CI = 1.06–2.56). 43
Ischemic stroke
Ischemic stroke appeared most sensitive to barometric pressure variability rather than absolute pressure level. A study reported a 5% increase in ischemic stroke admissions per unit of same-day pressure change (RR = 1.049, 95% CI = 1.007–1.092). 41 Another analysis found a statistically significant association between barometric pressure and stroke-related ED visits (p < 0.01). 44 High-acuity ischemic events, such as large-vessel occlusions requiring thrombectomy, were more common during rising pressure trends, with an estimated marginal effect of 0.38 (95% CI = 0.13–0.64). 45 In contrast, another study found fewer ischemic strokes were observed on days with extreme pressure variations, suggesting population- or climate-specific heterogeneity. 46 Humidity generally acted as a co-risk factor to barometric, with higher absolute humidity or rapid changes contributing to increased ischemic stroke presentations. 46 Among subgroups, medium Framingham-risk patients also had markedly higher odds during >10 hPa pressure rises (OR = 4.56, 95% CI = 1.26–16.43). 47
Hemorrhagic stroke
Hemorrhagic stroke showed a strong and consistent association with absolute barometric pressure extremes and variability. Deep hemorrhagic stroke incidence rose following barometric pressure drops, with significant associations at 2- and 3-day lags (p = 0.006 and p = 0.012, respectively), whereas lobar hemorrhage was not associated with pressure changes. 48 Another study similarly reported that low pressure modestly increased hemorrhagic stroke risk (OR = 1.02; p < 0.05). 49 Humidity effects in hemorrhagic stroke were directionally similar to those seen in total stroke, with larger 24-h humidity shifts associated with more hemorrhagic events, and several analyses suggesting stronger warm-humid effects for hemorrhagic than for ischemic events. 49 In a Portuguese study, each 1°C drop in diurnal temperature range was associated with a 12% increase in primary hemorrhagic stroke (RR = 1.12, 95% CI = 1.04–1.20, p = 0.003), reinforcing the sensitivity of stroke to short-term meteorological variability. 50 For aneurysmal subarachnoid hemorrhage, higher maximum daily pressure significantly increased risk (IRR = 1.022, 95% CI = 1.001–1.042; p = 0.014). 51
Summary
Across regions, stroke incidence tended to rise during low barometric pressure, pressure instability, and rapid humidity shifts, with several large studies showing notable increases in admissions under these conditions. Ischemic stroke was more strongly associated with pressure variability, whereas hemorrhagic stroke showed clearer sensitivity to absolute pressure extremes and short-term meteorological changes. Humidity often amplified these effects, and susceptibility varied by age, vascular risk, and stroke subtype. Overall, stroke incidence and hospitalizations increased during low-pressure or unstable pressure periods and when humidity was high or rapidly fluctuating, although findings remained heterogeneous.
Wildfires
Suggested mechanism
Wildfire smoke, rich in fine particulates and reactive compounds, promotes systemic inflammation, oxidative stress, and impaired vasodilation, leading to heightened thrombotic risk and short-term increases in ischemic stroke.
Study characteristics
A total of six studies evaluated the impact of wildfire exposure on stroke. Of these, four were ecological, one was cohort, and one was a case crossover study. These investigations were conducted across Brazil, Australia, the United States, and China. Three studies examined stroke without specifying subtype, while the remainder focused on either ischemic stroke or all stroke types combined. Outcomes varied across studies and included stroke mortality, emergency department visits, hospital admissions, and short-term stroke risk following wildfire exposure (ranging from day 0 to day 4 after smoke events). Collectively, this small but growing body of evidence provided initial insight into how wildfire-related air pollution may acutely influence stroke presentations and short-term stroke risk.
Studies including multiple or unspecified stroke subtypes
Across studies that assessed total stroke outcomes, wildfire smoke exposure, especially at medium and high smoke density levels, was consistently linked with short-term increases in stroke-related ED visits and hospitalizations. In Brazil, annual wildfire-related PM2.5 was linked to higher stroke mortality (RR = 1.020, 95% CI = 1.002–1.038). 52 Australian time-series studies similarly reported elevated cerebrovascular admissions during smoke events, although not all estimates were statistically significant. 53 A US case-crossover analysis found small but positive increases in cerebrovascular emergency visits with wildfire smoke PM2.5 (OR = 1.001, 95% CI = 0.994–1.007) (Li et al., 2024). 54 Hasnain et al. 55 provided multiple acute estimates, including a same-day RR = 1.52 (95% CI = 1.01–2.29, p = 0.04) with additional lagged IRRs showing similar directionality despite wider CIs. Review syntheses described consistent increases in total stroke outcomes across medium- and high-density smoke days, with effects often larger in older adults and regions with poorer baseline air quality. 56 The direction and magnitude of effects were consistent across geographic and analytic frameworks, and results remained robust after adjusting for temperature, humidity, and background air pollutants.
Ischemic stroke
Ischemic stroke outcomes showed clear and consistent associations with wildfire smoke exposure. In China, same-day ischemic stroke admissions rose by 0.25% (95% CI = 0.02–0.47) per 1 µg/m3 increase in wildfire-related PM2.5 across an estimated 59 million individuals. 57 Importantly, these associations remained after adjusting for PM2.5 from non-wildfire sources, suggesting that wildfire-specific PM2.5 contributed independently to stroke risk, although this analysis alone does not demonstrate that its chemical composition confers additional hazard beyond other PM2.5 sources. In a smaller study, increased ischemic stroke risk was observed across several lags, including a significant same-day RR = 1.52 (95% CI = 1.01–2.29, p = 0.04), but only on days with high concentrations of wildfire exposure. 55 Review articles emphasized that ischemic stroke findings were notably more robust than for hemorrhagic stroke, with clear acute-lag effects, dose responsiveness in some analyses, and stronger associations among old adults and socioeconomically disadvantaged regions. 15
Hemorrhagic stroke
Evidence for hemorrhagic stroke were more limited and less consistent. Some analyses reported no or borderline associations, while others identified modest but significant increases following high-density smoke exposure. 54 In a population-based study of the western United States, heavy smoke days were associated with a 4.2% rise (95% CI = 0.1–8.6) in hemorrhagic stroke ED visits within 0 to 3 lag days, although medium density exposure showed no significant effect (RR = 1.02, 95% CI = 0.98–1.06). 56
Summary
Wildfire smoke consistently elevated short-term stroke ED visits and hospitalizations, with stronger effects at higher smoke densities and among older adults, and long-term analyses similarly linked wildfire-related PM2.5 to increased stroke mortality. Ischemic stroke findings were particularly robust, showing clear dose–response relationships and short lag periods that persisted after accounting for non-wildfire pollutants, with older and lower income populations experiencing the greatest vulnerability. Evidence for hemorrhagic stroke was comparatively sparse and mixed, although several studies noted small increases in events during periods of heavy smoke.
Dust and sandstorms
Suggested mechanism
DSSs deliver particulate matter that triggers systemic inflammation, oxidative stress, autonomic imbalance, and endothelial dysfunction, accelerating prothrombotic processes and increasing stroke vulnerability.
Study characteristics
A total of eight studies examined the effects of DSSs on stroke; seven of these were ecological time-series studies, and one was a case crossover study. These investigations were conducted across Australia, Japan, Taiwan, Turkey, China, and Iran, with most regions represented by a single study. Four studies evaluated all stroke types combined, two focused exclusively on ischemic stroke, and two included both ischemic and hemorrhagic stroke. Reported outcomes included stroke mortality, emergency department visits, and hospital admissions for stroke or ischemic stroke, as well as short-term mortality following exposure.
Studies including multiple or unspecified stroke subtypes
Across ecological time-series studies, DSSs were associated with higher stroke admissions overall. In Taipei, DSS days were linked to higher total stroke admissions (RR = 1.05 [0.99–8.05]). 58 In another Taiwanese study, admissions rose significantly on post-DSS days 1–2 (β ≈ 19–25). 59 In Beijing, hospitalization risk increased during DSS periods for total stroke with particularly high risk reported in men (RR = 1.0301 [1.0067–1.496]). 60 In Iran, DSS-related mortality modeling suggested small short-term relative risks (RR = 1.007–1.013) and sizable attributable proportions (AP 5.67% short-term; 67.94% long-term), although CIs and p values were not reported. 61 In another Iranian study, DSS exposure was associated with higher stroke hospitalizations in men (RR = 1.0301 [1.0067–1.496]) but not women, and risk was elevated in adults >60 years (RR = 1.079 [1.014–1.040]). 62
Ischemic stroke
Evidence indicated short-term increased ischemic stroke events following DSS exposure, with mixed mortality findings. In Turkey, DSS days (AOD > 0.5) were linked to higher ED visits for ischemic stroke, while stroke mortality showed no association. 63 In Taiwan, increased admissions on post-DSS days were specifically observed for ischemic stroke. 59 In Japan, ischemic stroke admissions showed neutral associations across multiple lag windows (e.g. days 0–1 RR = 1.07 [0.94–1.23]; days 0–2 RR = 1.03 [0.91–1.17]). 64 For mortality, a multi-county analysis in China estimated excess ischemic stroke deaths of +7.49% (95% CI = 3.12–12.05) during DSS events. 65 In another Chinese study, DSS periods were associated with increased hospitalizations for ischemic stroke (p < 0.001). 60
Hemorrhagic stroke
Associations for hemorrhagic stroke appeared less consistent. In Taiwan, DSS days were associated with increased hemorrhagic stroke admissions (RR = 1.15 [1.01–10.15]). 58 In contrast, another Taiwanese study found that post-DSS day admission rise was not observed for hemorrhagic stroke. 59 In Japan, analyses did not show overall hemorrhagic stroke admission associations either. 64 A Chinese analysis estimated excess hemorrhagic stroke deaths of +5.40% (95% CI = 1.25–9.73%) during DSS events, 65 while another Chinese study found that hemorrhagic stroke hospitalizations showed did not increase during DSS periods. 60
Summary
DSSs were broadly linked to higher total stroke admissions, with several studies showing stronger effects in men and older adults, although estimates varied in magnitude and precision. Ischemic stroke generally showed short-term increases in admissions or deaths following DSS events, although a few studies reported neutral findings, reflecting some geographic heterogeneity. Evidence for hemorrhagic stroke was mixed, with modest increases observed in certain settings but no consistent pattern across studies.
Compound weather events
Suggested mechanism
Simultaneous exposures such as heat plus drought, or cold with humidity and wind, create synergistic physiological strain that overwhelms autonomic and vascular regulation, amplifying hemodynamic instability and substantially increasing stroke risk.
Study characteristics
A total of 20 studies examined the effects of compound weather events, and of these, 14 were ecological, five were case crossover designs and one was a cohort study. Most studies were conducted in China, followed by Europe and Japan, with one study each from Taiwan, Korea, Canada, and one multi-national study. Most studies did not specify the type or investigated both ischemic and hemorrhagic strokes. Reported outcomes included stroke incidence, mortality, emergency department visits, hospital admissions, and volume of endovascular thrombectomy cases.
Studies including multiple or unspecified stroke subtypes
Across studies that evaluated all stroke types, several compound weather patterns were associated with higher stroke incidence or hospital utilization. During compound drought-and-heat events, total stroke risk rose (RR = 1.18, 95% CI = 1.01–1.38), whereas moderate or low-severity droughts alone showed no association. 66 With regard to wind-related compound events, faster wind speed, greater daily wind-speed range, and wind-chill were each associated with higher total stroke incidence after multi-day lags; for example wind-speed OR = 1.18 (95% CI = 1.06–1.31) and wind-chill OR = 1.22 (1.07–1.39), with stronger effects in winter (wind-speed OR = 1.32 [1.10–1.60]). 67
Ischemic stroke
Multiple compound exposures were associated with increased ischemic stroke. In Taiwan, colder temperatures and 24-h changes in apparent temperature and humidity were linked to higher first-ever ischemic stroke admissions. For example, lower temperature at lag day 3 was associated with an OR of 1.134 (95% CI = 1.056–1.21), with subgroup elevations among older adults and women. 68 Consistent with this, a regional data set from Hunan Province found that extreme cold combined with high humidity produced a relative risk of 5.32 (95% CI = 3.40–8.34) for stroke compared with 2.82 (95% CI = 1.08–7.32) for extreme cold alone, underscoring the amplifying effect of concurrent moisture stress. 69 In Germany, a case-crossover study of first-ever ischemic strokes found women to be more sensitive to weather shifts than men (female OR = 1.39, 95% CI = 1.01–1.90). These shifts were defined as changes in a combination of ambient temperature, relative humidity, and atmospheric pressure. Large-artery atherosclerotic strokes showed the greatest risk increases (up to OR = 3.11, 95% CI = 1.28–7.53) with weather shifts. A time-series study similarly found sex-specific weather–stroke associations, with significant effects in men (temperature β = −0.01156, p < 0.001; humidity β = −0.00143, p < 0.01) and parallel coefficients for women. 70
In Japan, lower temperature bands and larger day-to-day pressure variation were associated with higher daily counts of alteplase-treated ischemic strokes (low temperature RR = 1.40, 95% CI = 1.05–1.86; p = 0.022; pressure variation RR = 1.45, 95% CI = 1.08–1.94; p = 0.012). 71 Large-vessel occlusion treatment cases also tracked with monthly meteorological compounds: lower barometric pressure and temperature correlated with higher endovascularly treated case volumes, while higher humidity showed a positive association (temperature β = −0.08 [95% CI = −0.10 to −0.06; p < 0.001], pressure β = −0.04 [95% CI = −0.07 to −0.03; p < 0.001], and humidity β = +0.07 [95% CI = +0.05 to +0.09; p < 0.001]). 72 Wind-related compound events were likewise associated with ischemic stroke incidence (wind-speed OR = 1.20 [95% CI = 1.08–1.34]; daily range OR = 1.09 [95% CI = 1.03–1.15]; wind-chill OR = 1.22 [95% CI = 1.07–1.39]). 67 During compound drought-and-heat events, ischemic stroke risk specifically increased (RR = 1.20, 95% CI = 1.03–1.40). 66 In Jiangsu Province, heat waves were associated with ORs between 1.17% and 1.50 (95% CI up to 1.57) for ischemic stroke deaths, and ozone increases across an interquartile range contributed an additional 3.7–4.2% of ischemic stroke deaths, about half to two thirds of which occurred under combined heat wave and ozone exposure. 73
Hemorrhagic stroke
Findings for hemorrhagic stroke outcomes were mixed. In Japan, a time-series analysis reported that lower temperature combined with falling barometric pressure was strongly associated with hemorrhagic stroke admissions, with a 35.57% increase per 1°C temperature drop (95% CI = 15.59–59.02) and a 3.25% rise per 1 hPa pressure decrease (95% CI = 0.94–5.51). 74 A Swiss observational study that jointly assessed temperature, relative humidity, barometric pressure, and wind gusts found no statistically significant or meteorologically meaningful deviations in any parameter for overall hemorrhagic stroke incidence. 75 During compound drought-and-heat events, admissions for hemorrhagic strokes were elevated, but nonsignificant. 66
Summary
Several combined weather conditions, such as drought-heat events, cold with wind or wind-chill, and rapid multi-variable shifts, were linked to higher stroke incidence, with some of the strongest effects seen in winter and during more intense compound exposures. For ischemic stroke, multiple compound patterns including cold plus humidity, rapid temperature and humidity changes, pressure variability, wind-related extremes, and dry–hot events consistently increased risk, often with amplified effects in older adults, women, and large-artery atherosclerotic stroke subtypes. Hemorrhagic stroke findings were inconsistent, with some analyses reporting strong associations during specific compound conditions while others showed no meaningful meteorological effects.
Discussion
Rising temperatures remain one of the most widely documented and immediate manifestations of climate change, with well-established impacts on human physiology, health systems, and population health outcomes. 10 Across studies assessing temperature and stroke, evidence consistently links colder conditions and large variations in temperature with elevated stroke risk, particularly for ischemic events, while heat-related effects are smaller and more variable, but do increase the risk of stroke and poor stroke outcomes overall. Cold exposure appears to increase hospitalizations, ED visits, and mortality across regions, with the most robust findings in large multi-country data sets. Temperature variability itself also contributes to higher risk, underscoring the potential vascular stress of rapid ambient changes. Strengths of this literature include large sample sizes, multi-city and international designs, and stratified analyses by stroke subtype, which improve external validity and comparability. Vulnerability appears greatest among older adults, those with metabolic disorders, and populations in colder or low-income settings, where both cold and heat extremes contribute disproportionately to stroke burden. Overall, the body of evidence supports temperature-related effects as a significant driver of stroke risk, particularly in cold and variable conditions. Recent multi-province and city-level data also indicate that heat waves also carry increasingly measurable stroke risks, with several large-scale studies showing effect sizes comparable to, and in some settings approaching, those of cold exposure. These findings reinforce emerging evidence that heat-related stroke risks are strengthening over time as global temperatures rise.
Humidity and barometric pressure are expected to shift in magnitude and variability as the climate warms, and these changes are emerging as important pathways through which climate change can affect human physiology and health outcomes. 10 We identified high-quality data sets showing quantifiable contributions of humidity and barometric pressure, independent of temperature, to first-ever stroke, hemorrhagic stroke, and ischemic stroke, with several studies reporting attributable fractions in the 2% to 4% range. Both low barometric pressure and pressure variability have been linked to increased stroke hospitalizations, while humidity, particularly rapid or high absolute variations, emerges as a contributing factor. Evidence suggests that ischemic stroke is more sensitive to short-term barometric pressure variability and humidity shifts, whereas hemorrhagic stroke shows stronger associations with absolute pressure extremes and delayed effects following drops in pressure. These findings support a plausible biological mechanism involving vascular reactivity and hemodynamic instability under abrupt weather changes. Strengths of the evidence include the use of large, time-series, and case-crossover designs with objective meteorological data and consistent directionality across diverse climates. Limitations include residual confounding by season. Vulnerable groups appear to include older adults, individuals with hypertension, and possibly younger adults exposed to acute pressure changes, reflecting differing susceptibilities across vascular phenotypes. Because humidity and barometric pressure were frequently modeled together, but their interaction terms were seldom significant, current evidence cannot determine whether these exposures exert independent or overlapping physiological effects. This limitation reflects methodological heterogeneity rather than evidence of absence and highlights the need for standardized, joint-exposure frameworks. These pressure- and humidity-related instabilities are projected to increase as climate change drives more frequent variations in heat, moisture, and atmospheric circulation, suggesting that stroke events linked to rapid meteorological shifts may rise in future decades. Interpretation of barometric pressure findings is further constrained by heterogeneity in stroke subtypes examined, pressure metrics used (absolute levels vs daily change), and the wide climatic contexts in which studies were conducted, limiting comparability of effect sizes.
Wildfire severity and frequency have and are expected to further increase with global warming, especially in regions such as North America, South America, the Mediterranean, southern Africa, and central Asia.10,76 We found consistent evidence that wildfire smoke exposure increases stroke risk from both time-series and ecological studies, mainly in the western United States, showing short-term and dose-dependent rises in ED visits and hospitalizations, particularly for ischemic stroke, within 1 to 3 days of exposure. Risk increases remain significant after adjustment for temperature, humidity, and background pollution, specifically non-wildfire PM 2.5. Biological plausibility stems from smoke-derived fine particulate matter and reactive compounds that promote systemic inflammation, oxidative stress, and vascular dysfunction. However, most studies are confined to high-income or major metropolitan regions, often from more temperate non-tropical climates, use ecological designs with variable exposure metrics, and underrepresent hemorrhagic outcomes, limiting generalizability. Despite these limitations, the consistency of findings, observed dose–response patterns, and biological plausibility collectively indicate that wildfire smoke meaningfully contributes to short-term stroke risk and that the evidence is consistent with a causal effect in the context of a warming climate.
DSS exposure is becoming increasingly common with desertification induced by climate change. 77 Compared with temperature, humidity, or barometric pressure, far fewer studies have assessed wildfire smoke or DSSs, resulting in narrower geographic coverage and greater uncertainty around the magnitude of effect. Across the reviewed studies, we found an association with higher short-term stroke admissions and possibly mortality, particularly for ischemic events. Most studies originate from East Asia and the Middle East and employ ecological or time-series designs that control for major air pollutants. Mechanistic plausibility stems from particulate-induced inflammation and vascular dysfunction. However, findings for hemorrhagic stroke are inconsistent, and data from other regions are sparse. Mortality data are also sparser and less conclusive, reflecting gaps in temporal resolution and case verification. Heterogeneity in storm definitions, exposure metrics, and confounder adjustment (especially for PM 2.5 and ozone) limits synthesis, although short lag temporal consistency across data sets lends credibility to the observed associations. In a departure from the other climate variables examined, men appeared to have a higher risk of poor stroke outcomes from DSS compared with women. It is possible that the data were skewed toward men being particularly vulnerable as they may have been more likely to be working or spending time outdoors, and therefore, disproportionately exposed to DSS compared with women who were underrepresented in these studies, but the authors of these articles do not expressly state this.
Compound weather events are projected to increase in frequency and severity as the climate warms, with the IPCC concluding that interacting extremes such as concurrent heat, drought, heavy rainfall, and high winds are already becoming more common and are expected to intensify under continued warming. (IPCC 2023) New data highlight that compound exposures often exceed the sum of their individual components. For example, extreme cold combined with high humidity can more than double the stroke risk seen with cold alone. These findings suggest an association in which stroke vulnerability in a destabilizing climate may be shaped not only by isolated extremes but also by compounding meteorological variables. Studies reveal that concurrent cold, wet, and windy conditions, or heat combined with drought, amplify admissions and mortality, particularly for ischemic stroke and among older adults and women. While analytic designs and definitions vary widely, and most data derive from East Asia, the recurring observation that simultaneous environmental stressors heighten stroke risk underscores the need for models accounting for interacting exposures. Gaps include inconsistent lag definitions, neglect of pollutant or socioeconomic modifiers, and exclusion of many world regions, but the convergence of findings across diverse data sets strengthens confidence in linking compound weather events and stroke. Standardized definitions and multi-region replication are needed to strengthen inference.
Common limitations across the climate–stroke literature include its heavy reliance on ecological study designs. Ecological studies are considered among the weakest epidemiological designs, because they measure associations at the group or population level, meaning that observed trends may not necessarily reflect individual-level effects. There is also often limited ability to control for potential confounding factors, imprecision in exposure or outcome measurement, and inherent challenges in establishing causal relationship. Even among non-ecological studies, outcome measures are heterogenous and adjustment for key confounders such as air pollution and behavioral factors is frequently incomplete, and although many studies report co-exposures, many do not examine their interactions, leaving synergistic or modifying effects largely untested. Compounding these issues is the relative scarcity of case crossover studies, a design that offers stronger methodological control for short-term environmental exposures by using individuals as their own controls and inherently accounting for time-invariant confounders. The limited use of this approach reduces the overall robustness of the literature in evaluating acute exposure–outcome relationships and weakens causal inference regarding the short-term effects of environmental factors on stroke.
Another limitation is that the evidence base is disproportionately weighted toward China, constraining global generalizability, and most analyses focus on adults, with limited pediatric data. Short lag periods of one to several days are common, yet lag structures vary widely, making cross-study comparison difficult and suggesting that some climate-related stroke events may be underestimated. Finally, because hemorrhagic strokes are generally less common than ischemic strokes, many studies lack sufficient power to detect stroke subtype-specific effects.
Populations at highest risk appear to be older adults, individuals with metabolic disease, and communities with limited adaptive capacity or incomplete infrastructure, including many low- and middle-income regions. Several studies also identified greater susceptibility among women in certain compound-exposure settings and among people with hypertension or hyperglycemia under rapid temperature shifts. Together, these findings indicate that both biological vulnerability and structural inequity shape the populations most affected by climate-related stroke risk.
This review did not specifically consider air pollution. Due to the well-established strong link between air pollution and stroke per the 2025 WSO Stroke Fact Sheet (Feigin et al., 2025), an upcoming WSO statement will be dedicated to this topic. However, while primarily a driver rather than a sequela of climate change, air pollution clearly has high relevance to the topic of climate change and stroke and the two statements should be viewed as complementary.
Implications
The evidence collectively shows an association between a rise in stroke risk and poor outcomes in response to climatic instability from both the absolute changes and variations in temperature, barometric pressure, and humidity; patterns that mirror the very shifts projected to intensify under climate change. Rather than being driven by static temperature or single-weather extremes, stroke vulnerability reflects dynamic environmental volatility; abrupt transitions, interacting stressors, and compounding exposures as evidenced in the wildfire, DSS, and compound weather events data. Climate change magnifies these dynamics by increasing temperature variability, altering pressure and humidity cycles, extending wildfire seasons, and expanding DSS from droughts and desertification, thereby extending both the duration and geographic reach of increased stroke risk. Notably, despite global warming, seasonal cycles will continue, and cold extremes will still occur in a warming climate.78,79
The geographic distribution of findings parallels climate trends, with stronger associations in LMICs or high-exposure settings where adaptation infrastructure is limited. These regions face the dual burden of increasing climatic instability and constrained health system capacity, amplifying the inequality of climate-related stroke risk. With the exception of DSS, stroke risk in women is often disproportionately affected by the examined climate variables in several studies. The disproportionate effects seen in many studies among older adults and individuals living with metabolic conditions suggest that physiological resilience to rapid environmental shifts is already strained and may deteriorate further as extremes become more frequent that may further exacerbate current health inequities.
Taken together, the data suggest that stroke is an under-recognized contributor to the health burden of a destabilizing climate and merits consideration alongside other climate-sensitive diseases such as heat-related illness, ischemic heart disease, chronic obstructive pulmonary disease, acute kidney injury, and vector-borne infectious disease. 80 The convergence of these climate variables and their interactions are associated with worsened stroke incidence and outcomes, underscoring that climate change acts through multiple overlapping pathways in biologically plausible mechanisms: thermal stress, hemodynamic fluctuation, inflammation, and systemic oxidative load. Stroke thus exemplifies how the changing climate is not only reshaping environmental exposure profiles but is also directly translating those shifts into measurable, population-level disease patterns.
Recommendations
While stroke sits at the intersection of brain and vascular health, it is also shaped by the air people breathe, the food they eat, the environments they inhabit, and the policies that govern access to essential resources. Stroke clinicians and researchers, therefore, work at the interface of medicine and a rapidly changing climate, with emerging evidence showing that climate-driven environmental instability is becoming an increasingly relevant contributor to stroke risk and outcomes. As these climate-related determinants of health intensify, the scope of stroke care is broadening beyond clinical encounters to include an understanding of how environmental conditions influence vulnerability and outcomes. This growing recognition also positions stroke clinicians to join other health professionals in advocating for policies that mitigate climate change and promote cleaner air, safer built environments, and resilient health systems that protect people from climate-related stroke risk.
Evidence indicates that climatic drivers relevant to stroke, including temperature extremes, humidity variations, droughts, and compound weather events, are increasing in frequency, intensity, or both as global temperatures rise. 81 Cold-related events are generally becoming less common. However, the overall burden of temperature-related vascular stress is expanding, driven mainly by rising heat-related events and their indirect effects on humidity, barometric pressure, and natural disasters. These changes amplify existing risks, reinforcing inequities in exposure, vulnerability, and capacity to adapt.
Communities already facing socioeconomic disadvantage, systemic inequity, or chronic disease bear disproportionate impacts. Disruptions to food and water security, medication access, and healthcare continuity during extreme weather further heighten stroke risk and worsen outcomes. Together, these interrelated challenges strain clinical care delivery and the sustainability of stroke systems, with especially pronounced effects on people living with post-stroke and other neurological disability. 82
Adapting clinical practice to these realities involves integrating climate considerations into patient care. This includes discussing heat safety plans, ensuring reliable access to cooling, air quality, and medications during weather disruptions, and recognizing how environmental stressors interact with side effects from antihypertensive or diuretic therapies. Medication reviews should include thermoregulatory risk and storage stability during heat events. Clinicians can promote individualized acclimatization strategies, including cooling, hydration, and rest during high-heat periods, particularly for older adults and those with limited mobility. Raising these topics and their links to climate change can also help raise public awareness of the importance of climate change mitigation. Addressing climate anxiety through supportive counseling or community engagement can further strengthen patient resilience. 83 Hospitals and rehabilitation centers should prioritize access to greenspace and thermal comfort as measurable components of recovery and health equity, recognizing their protective effects against vascular and neurodegenerative disease. 84
System-level responses are equally important. Health systems can embed climate resilience into accreditation standards and emergency preparedness. Hospitals may integrate weather alerts to anticipate seasonal surges in admissions, coordinate with public health authorities for early intervention, and ensure energy-efficient, climate-ready infrastructure. 85 The evidence for harm from compound weather data underscores the importance of incorporating multiparameter environmental alerts that track compound exposures (temperature, humidity, pressure shifts, wildfire smoke, and air quality indices such as ozone) into hospital triage and surge preparation systems. Built-environment adaptation, including passive cooling design, flood resistance, and renewable energy generation, should be part of all new hospital and rehabilitation construction. Community participation as part of health systems can also support the detection of potential weather-related conditions and provide caring attention during or after emergencies. This is particularly important in contexts where Indigenous medicines and traditional practices can inform response efforts.86,87 Policymakers can promote equitable access to safe indoor environments, clean air, and thermal comfort through incentives and building codes that align health and climate goals. Finally, clinicians should counsel high-risk patients on heat-wave preparedness, emphasizing high-risk periods of the year, including hydration, cooling plans, medication review for heat sensitivity, and identification of indoor safe spaces.
Research and education should evolve accordingly. Collaboration between stroke researchers, climatologists, and epidemiologists can refine exposure–response models, identify differential risks across demographic and geographic groups, and improve data on indoor exposures. The Neuro Climate Working Group brings together such experts from over 17 countries, advancing research on climate change and brain health through monthly webinars and interdisciplinary educational and research collaborations. 88 Other groups include the World Federation of Neurology (WFN) Environmental Neurology Specialty Group and the Australian and New Zealand Association of Neurologists (ANZAN) Climate Group. However, global stroke-specific groups are yet to emerge and could be prioritized. 89 Expanding studies in LMICs is needed to inform adaptation strategies. Professional organizations can integrate environmental neurology and climate-health literacy into continuing education, training, and certification programs so that neurologists develop the competence and confidence to recognize and address these emerging climate-related threats. 90 Existing global knowledge-sharing networks, such as Climate ECHO, can serve as models to facilitate these efforts. 91 Sustainable research practices, such as minimizing travel-related emissions, adopting virtual conferencing, and evaluating the carbon footprint of laboratory and data-intensive modeling, can reduce the environmental impact of scientific inquiry.92,93
Many of the existing medical society guidelines on stroke prevention already emphasize lifestyle measures that, if implemented thoughtfully, can also advance climate mitigation. Plant-dominant diets, active travel through walking and biking, and phasing out fossil fuels all foster cleaner air and healthier environments while supporting both planetary and brain health. Preventing avoidable hospitalizations through healthy lifestyles simultaneously reduces healthcare system utilization and the carbon footprint associated with it. 26 This is particularly relevant given that more than 80% of healthcare emissions arise from hospital operations, the production of medical equipment and other purchased goods, employee commutes, and institutional investments. 94 Climate change thus represents not only an environmental issue but also an exacerbation of broader systemic determinants of health and inequity.
Addressing these linkages requires advocacy, systems thinking, equity-oriented practice, and coordinated action. By advancing sustainable food systems, resilient healthcare infrastructure, and evidence-informed policies, stroke clinicians and researchers can strengthen the social and environmental foundations that support neurological health. Stroke professionals and societies can also join others in the health sector in their efforts to advocate for more general climate change mitigation. The task at hand is substantial but essential to ensure that stroke prevention and care remain effective, equitable, and resilient for people living in a changing climate and for the neurologists committed to their care.
Key recommendations
Reduce Emissions While Improving Brain Health ● Promote clean energy, plant-rich diets, and active transport (walking, biking) to cut emissions and stroke risk at institutional, municipal, national, and international levels. ● Advocate for the preservation and restoration of green spaces to revitalize air, water, and land.
Strengthen Clinical and System Preparedness ● Educate patients on heat/cold and other climate/weather-related impacts and safety. ● Integrate climate-sensitive risk into hospital disaster plans
Enhance Early Warning and Response ● Embed temperature, pressure, dust, and sandstorms alerts into hospital electronic health records (where available) and public messaging. ● Implement heat-health plans with cooling centers, wellness checks, and outreach to vulnerable groups. ● Integrate compound-exposure warnings (heat + ozone, cold + humidity, pressure drops, wildfire smoke) into early-warning systems and public health messaging, as these combinations carry disproportionately high stroke risks. ● Integrate environmental-risk alerts (extreme temperatures, heat or cold waves, humidity shifts, DSSs, wildfire smoke) into prehospital triage algorithms and EMS routing to anticipate periods of elevated stroke risk and reduce delays in timely care
Advance Research and Evidence ● Expand research from LMICs and pediatric populations. Standardize definitions, measurements, and reporting of environmental exposures ● Promote standardized climate and climate-health metrics and cross-sector collaboration. ● Test the economic and health impacts of interventions and adaptation strategies. ● Increase the use of robust individual-level study designs, particularly case crossover and prospective cohort studies, to improve control for confounding and strengthen causal inference
Promote Equity and Global Coordination ● Support equitable access to clean air, heating/cooling, green spaces, and resilient infrastructure. ● Prioritize vulnerable populations and align global efforts through WHO, WSO, and mainstream stroke and neurological organizations. ● Strengthen interdisciplinary cooperation among meteorological agencies, environmental scientists, urban planners, and emergency services to develop coordinated policies for preparedness, early warning, and response to climate-related stroke hazards.
A summary of these recommendations is displayed in Figure 3.

Key recommendations.
Supplemental Material
sj-docx-1-wso-10.1177_17474930261436535 – Supplemental material for Stroke and climate change: A World Stroke Organization scientific statement
Supplemental material, sj-docx-1-wso-10.1177_17474930261436535 for Stroke and climate change: A World Stroke Organization scientific statement by Ali Saad, Maria Khan, Conrado Estol, Mohammad Wasay, Tomoaki Kameda, Teresa Ullberg, Yannick Béjot, Serefnur Ozturk, Maria Epifania Collantes, Carol Zavaleta-Cortijo, Janice Kang, Alexandra Macmillan, Daniel G Kingston, Janet Stephenson, Jacques Reis and Anna Ranta in International Journal of Stroke
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Yannick Béjot reports personal fees from BMS, Pfizer, Medtronic, Boehringer-Ingelheim, Amgen, Servier, NovoNordisk, Novartis, and Argenx outside the submitted work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.