
Abstract
Background:
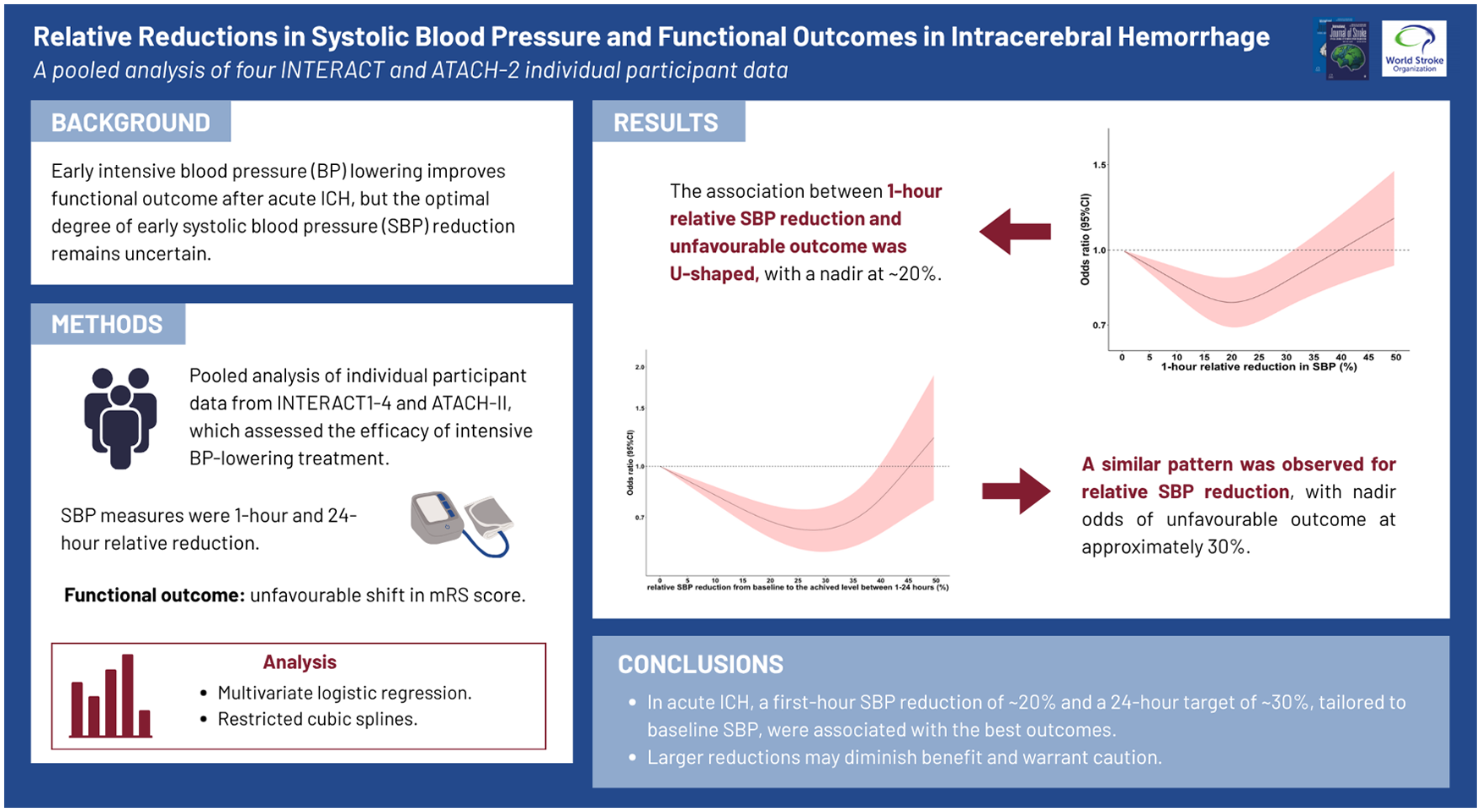
Early intensive blood pressure (BP) lowering improves outcome after acute intracerebral hemorrhage (ICH), but the optimal degree of early systolic blood pressure (SBP) reduction remains uncertain.
Aims:
We aimed to identify relative SBP reduction thresholds associated with the most favorable functional outcome after ICH.
Methods:
We performed an individual participant data meta-analysis of five randomized trials of acute BP lowering in ICH (INTERACT1–4 and ATACH-II). The relative reduction measurements in SBP were defined as the percentage decrease (a) from baseline SBP to the lowest SBP in 1 h (primary) and (b) from baseline SBP to the achieved mean of SBP between 1 and 24 h. Associations with functional outcome, assessed as an unfavorable shift in scores on the modified Rankin scale (mRS) at the end of follow-up (90 or 180 days), were examined in multivariable ordinal logistic regression models and tested for non-linearity using restricted cubic splines. Heterogeneity of associations between the 1-hrelative SBP reduction and functional outcome by age, sex, history of hypertension, history of diabetes, baseline SBP, and hematoma volume was further explored by including each interaction term into the models.
Results:
Among 11,283 participants (mean age, 62.6 years; 36.0% female; mean baseline SBP, 176.9 mmHg), the association between 1-h relative SBP reduction and unfavorable functional outcome was U-shaped with an inflection nadir at around 20%. Associations differed by sex, baseline SBP, and history of diabetes (all p for interaction <0.05). A similar U-shaped association was also observed in relation to the relative SBP reduction from baseline to the achieved level in 1–24 h, with the greatest apparent benefit at approximately 30%.
Conclusion:
In acute ICH, a first-hour relative SBP reduction of around 20% and a 24-h reduction target of 30%, individualized to the presenting SBP, were associated with the most favorable functional outcome. Larger reductions may attenuate the benefit and should be applied cautiously, particularly in patients with very high baseline SBP.
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.