
Abstract
Background:
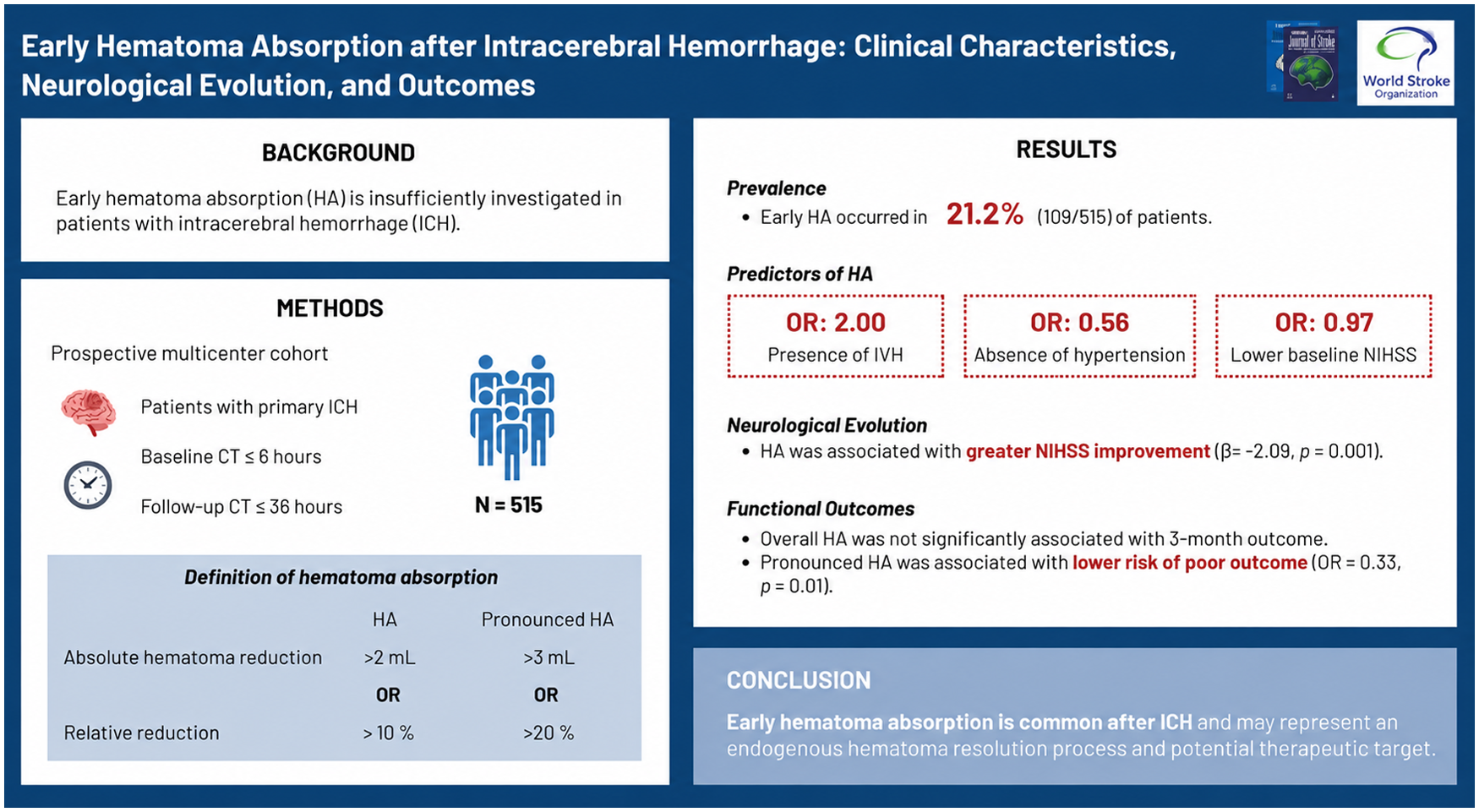
Early hematoma absorption (HA) has been insufficiently investigated in patients with intracerebral hemorrhage (ICH). This study aimed to determine the prevalence of HA and to evaluate its association with neurological and functional outcomes.
Methods:
We analyzed prospectively collected data from patients with primary ICH. Eligible patients underwent baseline computed tomography (CT) within 6 h of symptom onset and follow-up CT within 36 h. HA was defined as an absolute reduction in hematoma volume > 2 mL or a relative decrease > 10%. Pronounced HA was defined as an absolute reduction > 3 mL or a relative decrease > 20%. Early neurological deterioration (END) and early neurological improvement (ENI) were defined as an increase of ⩾ 4 points and a decrease of ⩾ 2 points in the National Institutes of Health Stroke Scale (NIHSS), respectively. Functional outcomes at 3 months were assessed using the modified Rankin Scale (mRS), with poor outcome defined as mRS 4–6.
Results:
Among 515 patients (median age, 60 years; 31.7% female), 109 (21.2%) exhibited early HA. END occurred in 65 patients (12.6%), and ENI in 93 patients (18.1%). In multivariable analyses, HA was independently associated with the absence of hypertension and with the presence of intraventricular hemorrhage (odds ratio (OR), 2.00; 95% confidence interval (CI), 1.19 to 3.36; p = 0.009). HA was also significantly associated with greater neurological improvement, reflected by a larger reduction in NIHSS score (β = −2.093; 95% CI, −3.369 to −0.816; p = 0.001) in adjusted linear regression models. While HA was not associated with 3-month functional outcome overall, pronounced HA was independently associated with a reduced risk of poor outcome (OR, 0.325; 95% CI, 0.133 to 0.795; p = 0.014).
Conclusion:
Early hematoma absorption occurs in approximately one-fifth of patients with acute ICH and is associated with favorable early neurological evolution. These findings suggest that HA may reflect endogenous hematoma resolution processes and represent a potential therapeutic target in ICH.
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.