
Abstract
Background:
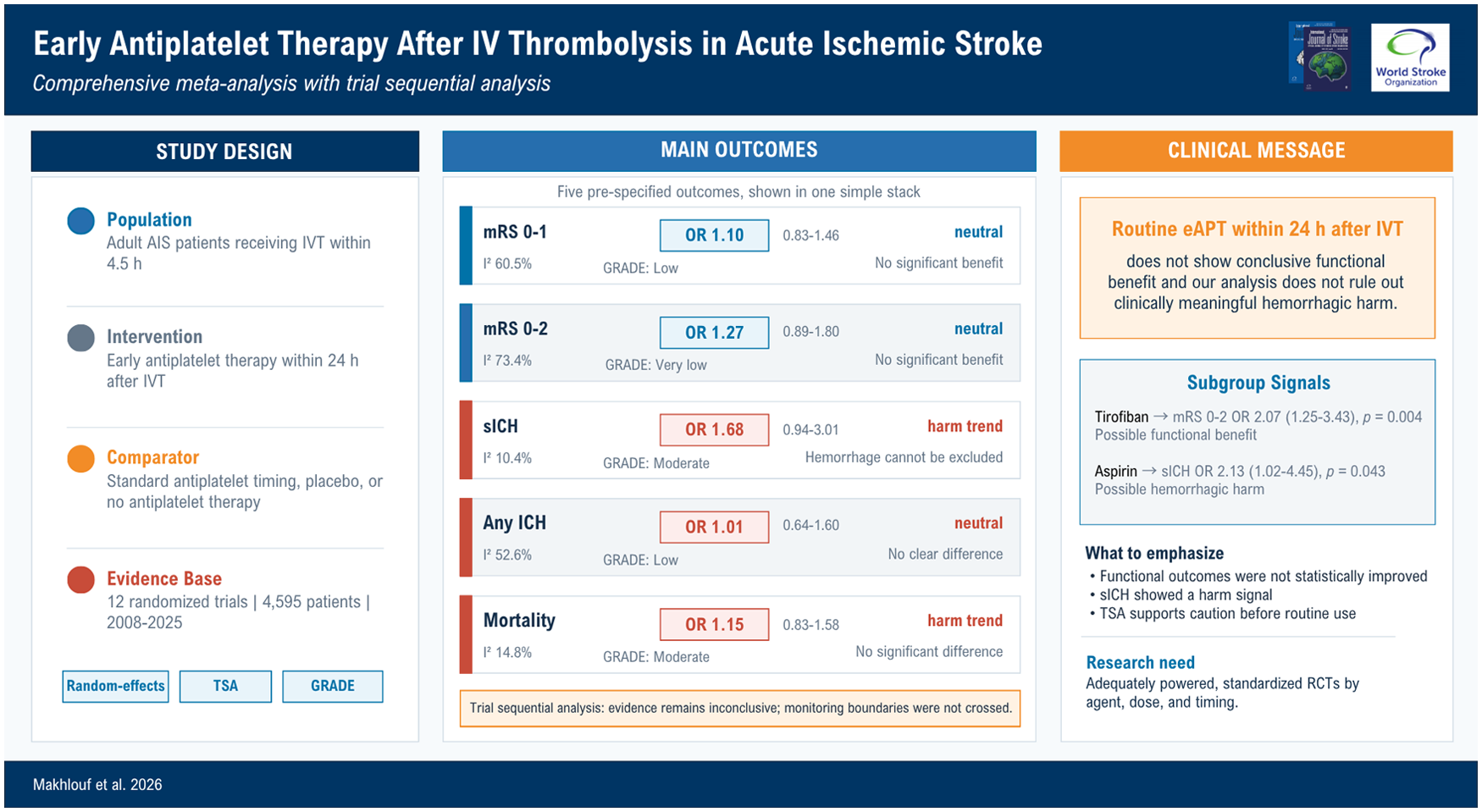
Early antiplatelet therapy after intravenous thrombolysis (IVT) in acute ischemic stroke (AIS) patients may prevent re-occlusion and early neurological deterioration, but it could increase hemorrhagic transformation. Evidence remains conflicting, particularly with emerging contemporary trials.
Methods:
We conducted a Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA)-guided systematic review of randomized controlled trials (RCTs) comparing early antiplatelet therapy (eAPT) initiated within 24 h after IVT (with or without thrombectomy) versus standard timing (>24 h), placebo, or no antiplatelet therapy (CRD420251276445). Random-effects models were used to estimate odds ratios (ORs) and mean differences (MDs) with 95% confidence intervals (CIs). Trial sequential analysis, subgroup analyses, meta-regression, and Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) certainty ratings were performed.
Results:
Twelve RCTs with 4595 patients were included. Early antiplatelet therapy led to higher non-significant odds of symptomatic intracranial hemorrhage (sICH; OR = 1.68, 95% CI = 0.94–3.01; I2 = 10.4%; GRADE moderate), and mortality (OR = 1.15, 95% CI = 0.83–1.58; I2 = 14.8%; GRADE moderate) but not intracranial hemorrhage (OR = 1.01, 95% CI = 0.64–1.60; I2 = 52.6%; GRADE low). Functional outcomes were not improved: Modified Rankin Scale (mRS) 0–1 (OR = 1.10, 95% CI = 0.83–1.46; I2 = 60.5%; GRADE low) and mRS 0–2 (OR = 1.27, 95% CI = 0.89–1.80; I2 = 73.4%; GRADE very low). Trial sequential analysis indicated evidence remains inconclusive. Agent-specific subgroup analyses suggested higher sICH with early aspirin (OR = 2.13, 95% CI = 1.02–4.45) and possible benefit for mRS 0–2 with tirofiban (OR = 2.07, 95% CI = 1.25–3.43).
Conclusion:
Routine early antiplatelet therapy within 24 h after IVT does not provide conclusive functional benefit, and our analysis cannot exclude clinically meaningful hemorrhagic harm. Further adequately powered RCTs are needed to define whether any selected regimen—especially tirofiban—has a favorable risk–benefit profile.
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.