
Abstract
Objective
Concussion is a common injury in ice hockey, and previous research suggests some misconceptions and unsafe attitudes amongst players. The purpose of this study was to assess sport concussion knowledge, attitudes and the effect of sport concussion history in UK-based male ice hockey players across three levels of competition: professional, semi-professional and amateur.
Methods
Sixty-one participants across a number of UK ice hockey teams completed the Rosenbaum Concussion Knowledge and Attitudes Survey and reviewed a series of statements to assess knowledge (concussion knowledge index), attitudes (concussion attitude index) and misconceptions of concussion.
Results
Level of competition and concussion history had no significant effect on concussion knowledge index or concussion attitude index. A positive significant relationship exists between playing experience and concussion knowledge index and concussion attitude index. Statements identified common misconceptions and areas of accurate knowledge regarding concussion symptoms suggesting that male ice hockey players have a higher level knowledge compared to a sample of the UK general public. Playing experience was associated with increased knowledge and increasingly safe attitudes towards concussion.
Conclusion
Despite knowledge relating to loss of consciousness and correct management of symptoms being generally accurate, there are worryingly unsafe attitudes regarding aspects of concussion. Such attitudes may well pose significant threats to players’ safety and long-term health.
Introduction
The Consensus Statement on Concussion in Sport indicates that concussion is a complex pathophysiological process affecting the brain as a result of traumatic biomechanical forces. Symptoms such as loss of consciousness to nausea, headaches, dizziness and general disorientation usually appearing rapidly, though in some cases symptoms are delayed by several minutes to hours. 1 However, it is only recently that concussion has been acknowledged as a traumatic brain injury and more care given to those with concussion. 2 Knowledge of the indicators of concussion and how to manage concussion is essential for key personnel (i.e. athletes, coaches and family) to help prevent injury and aid recovery. The latter may involve encouraging the return-to-play protocols, which are often dismissed by athletes once they feel ‘back to normal’. 3 Such beliefs highlight the importance of accurate knowledge and safe attitudes towards concussion held by the athlete themselves.
There is a lack of epidemiological data; however, at the highest level of ice hockey (the National Hockey League), the concussion rate in the 2011–2012 season was 10.24 per 100 games (Actual Concussion 6.83, Suspected Concussion 3.41); 64.2% of the concussions were caused by body-checking, whilst only 28.4% of the concussions (and 36.8% suspected) were caused by illegal incidents. 4 In a description of concussion in international ice hockey between 2006 and 2015, Tuominen et al. identified that 66% of the concussions were caused by illegal contact. 5 The most common situation leading to concussion was contact with another player (89%), with checking to the head (42%) and body checking (23%) accounting for the majority of these. These statistics highlight that concussion is currently an inevitable part of the game and consequently, there is a need for effective knowledge amongst those involved. Previous research into athletes’ understanding of concussion has typically shown poor knowledge regarding injury mechanisms and symptoms, post-injury vulnerabilities and recovery time. 6 For example, Sye et al. 7 found that high school rugby athletes typically consider loss of consciousness necessary for a concussion injury. Research by Hänninen et al., however, shows that loss of consciousness is only one of a number of diverse clinical presentations. 8 As an example, high school American football coaches’ concussion knowledge of symptom recognition is reasonable and they possess good awareness of their athletes’ reluctance to report concussions. 9 Jorgensen et al. 10 suggested that increased knowledge of concussion reporting and behaviours did not necessarily correlate to better attitudes in 72 varsity soccer, hockey and basketball athletes. However, in agreement with the findings by Sye et al., 7 a significant number of youth sport coaches considered loss of consciousness as necessary for a concussion injury. 11 Studies have also shown significant misconceptions relating to recovery from and symptoms of concussion in the general population. 12
A recent study by Weber and Edwards 3 assessed concussion knowledge of 227 members of the UK general public (aged 18–76), with participants rating the truthfulness of a series of statements relating to concussion with a choice of four responses (true, probably true, probably false and false), to determine the difference between a lack of knowledge and clear misconceptions. The results identified widespread lack of knowledge and misconceptions around the most frequent indicators of concussion within the general public. Participants expressed definite ‘incorrect’ responses to a subset of statements, e.g. trouble remembering events from before the concussion, but not having trouble learning new things, which is in fact false, and the increased vulnerability to concussion after a previous concussion which is true. The non-definite results for these statements showed that the majority (more than 50%) of participants were unsure of their responses. The seriousness of concussion is clearly underestimated, for example, most participants rejected the idea of increased vulnerability to and likelihood of re-injury following concussion. The general public also showed a lack of knowledge of injury mechanisms and recovery assessment. Participants’ history of concussion had no influence on their knowledge. However, Weber and Edwards 3 suggested previous experience may have created a false sense of understanding evidenced through increased certainty of, but not accuracy in their knowledge.
More recently, Williams et al. 13 examined English professional soccer players’ concussion knowledge and attitude by implementing the Rosenbaum Concussion Knowledge and Attitudes Survey (RoCKAS) and semi-structured interviews. The RoCKAS provides a comprehensive measure of concussion knowledge and attitude and has proved to be valid and reliable. 6 The results evidenced some accurate knowledge: the majority (88.5%) knew that loss of consciousness was not required for a concussion and recognised that concussions will affect sport performance (88.5%). However, some concerning misconceptions included only 3.8% knowing that there is an increased likelihood of repeat concussions after a player has sustained one, and only 46.2% aware of long-term risks to health from multiple concussions. Participants expressed safe attitudes towards concussion including: athletes who lose consciousness should be taken to hospital (80.8%); managers should not let players with concussion play (80.8%) and it is the physiotherapists who make the return to play decision (69.3%). But 64% of players stated they would continue to play even if they believed they had suffered a concussion, with 96% indicating that the importance of the match would influence their reporting and action towards the injury. To the best of our knowledge, there is no current literature relating to knowledge and attitudes within ice hockey players, which is concerning given the prevalence presented above.
Education about concussion within ice hockey is relatively new, with educational programmes focusing particularly on symptom recognition and reporting procedures14–16 as an injury prevention intervention. For example, Cook et al. 14 had 11–12-year-old male hockey players in Canada viewing a concussion and spinal cord injury prevention video. The video included medical information and personal experiences of recognised professional players, team doctors, coaches and trainers. Knowledge significantly improved and did not decay over a three-month period. Rule infringements of crosschecking and checking from behind both showed a decline in number of calls against the players who had viewed the video. Smart Hockey, Heads Up and Heads Up Hockey (USA Hockey) are the main programmes in North America; however, none of these programmes have been systematically evaluated, meaning conclusions on their effectiveness cannot definitely be made. Hockey Canada has also developed a concussion awareness app that is available to provide detailed information on concussion as an injury, how to manage symptoms and recovery, and returning to play. In the UK there is currently only one educational programme: Headcheck, launched in 2015 to raise awareness of concussion. The initiative includes information about the symptoms of concussion, the potential consequences of the injury and advice on how to manage the injury, and information about the return to play protocol. Posters and leaflets are available to download from the website for all individuals involved, i.e. managers, coaches, medical staff, players and parents.
Despite an increase in research and professional interest in sport concussion, the application of the known facts (causes, symptoms, recovery) does not appear to be transferring to those most involved, i.e. players, coaches and parents – as highlighted by the widespread lack of knowledge within the general public 3 and the concerning attitudes of footballers who would continue to play even if they suspected a concussion. 13 Current educational approaches such as Smart Hockey (Canada), Heads Up Hockey (USA) and Headcheck (UK) are attempting to address the concerns of insufficient knowledge of concussion. Given the increased incidence of concussion in ice hockey, the present study aims to replicate the work of Williams et al., 13 and Weber and Edwards 3 to examine the current knowledge about and attitudes towards concussion in a group of adult male UK-based ice hockey players. To date, there is no known research addressing UK-based ice hockey players. It is anticipated that (a) based on previous research in the UK, there will be misconceptions and a lack of knowledge and unsafe attitudes within the male ice hockey player population and (b) attitude and previous experience of concussion may influence athletes’ knowledge and behaviour regarding concussion.
Method
Participants
Sixty-one male ice hockey players within the UK volunteered to participate in the study, ages ranged from 19 to 48 years (M = 27.25). All players were competing at one of three leagues (low to high): Laidler Conference, Moralee Conference or the English Premier League. Players represented professional (N = 19), semi-professional (N = 28) and amateur (N = 24) playing standards. The study was approved by the University Institutional Review Board, and full compliance of the Helsinki Convention, 1964 and Declaration of Tokyo, 1975, as revised 1983 was adhered to at all times. All participants provided informed consent and were debriefed upon completion of the task.
Measures
Knowledge of and attitude towards concussion
Concussion knowledge and attitudes were assessed using the previously validated 55-item RoCKAS (Rosenbaum and Arnett, 6 Chapman et al. 17 ), which generates two scores: a concussion knowledge index (CKI) and concussion attitude index (CAI). The CKI contains 14 basic and 3 applied true and false questions graded 1 (correct) or 0 (incorrect), and recognition of 8 common concussions symptoms (with 8 distractor symptoms) for a total possible score 25. The CAI contains 15 Likert scale (1: strongly disagree; 5: strongly agree) questions. Safer answer receives 5 points and the least safe answer receives 1 point resulting in a score range of 15–75. High scores on CKI (e.g. 25) and CAI (e.g. 75) indicate better knowledge of and attitudes towards concussions.
Concussion knowledge misconceptions
The second measure consisted of 24 true or false statements adapted from Weber and Edwards 3 to explore sport concussion knowledge. For example, ‘An SC can cause brain damage even if the sports person is not knocked out’ (True). Two original statements were removed from the original 26 statements due to their lack of relevance to the study and sample population: ‘in sport, sport concussion never happens’ and ‘a sports concussion affects men’s and women’s brains differently’. The remaining 24 statements required responses of true, probably true, probably false and false; with the original researchers 3 suggesting indefinite answers highlight uncertainty. Misconception percentages were calculated as misconceptions in collapsed responses (true/probably true; false/probably false) and percentage of participants making definite and non-definite responses. The measure was appropriate for this setting as it has been used with UK general population 3 and a UK athletic sample (English Professional Football 13 ) to illucidate misconceptions.
Player characteristics
Basic demographics of each participant were also collected, including their playing experience (the length of time individuals have played competitively), current level of competition (professional, semi-professional, amateur) and concussion history (how many known concussion individuals have suffered).
Procedure
UK-based ice hockey teams were initially contacted regarding access to their players and participation in the study as well as individual players through direct contact. To conduct the study, the lead author travelled to participating team training sessions during the 2015–2016 season. Participating players provided written informed consent and were debriefed upon completion. After receiving written informed consent from the participants, the instruments were completed individually and privately.
Statistical analysis
SPSS V22 (IBM, Chicago, USA) was used for final data analysis (significance p < .05). A one-way analysis of variance (ANOVA) was used to examine any difference in CKI, CAI and concussion knowledge misconceptions across the three competition levels (professional, semi-professional, amateur). An independent t-test examined differences in concussion knowledge or attitude based on previous concussion history. The normality and homogeneity of variances within the data were confirmed with the Kolmogorov–Smirnov test and Levene’s tests, respectively. No missing values were identified. Finally, Pearson correlations assessed relationships between years of playing experience, concussion knowledge and attitude.
Results
RoCKAS
Mean and standard deviations for concussion knowledge index (CKI) and concussion attitude index (CAI) scores.

Note: CKI scores range from 0 to 25 and CAI scores range from 15 to 75, with higher scores represented greater knowledge and safer attitudes about concussion, respectively.
Mean and standard deviation for concussion history.
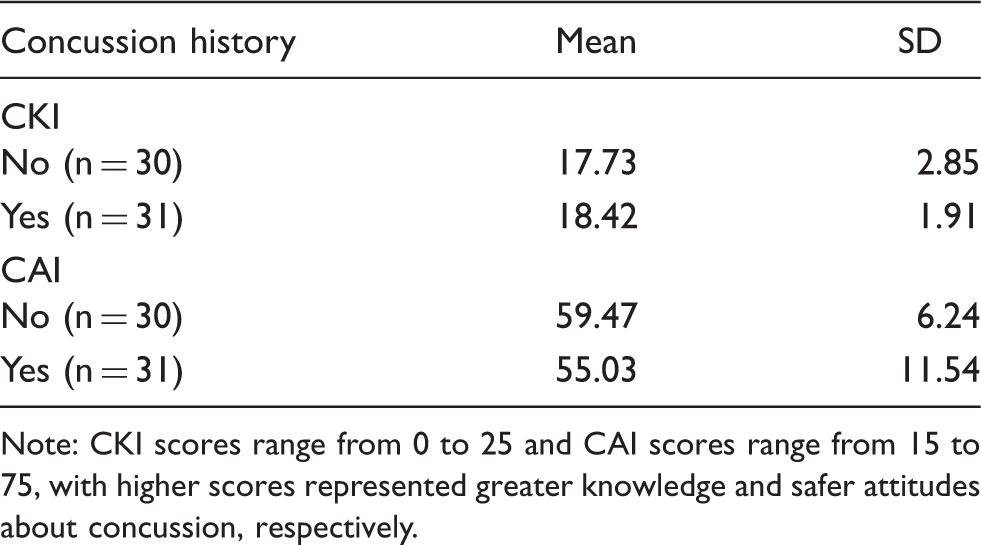
Note: CKI scores range from 0 to 25 and CAI scores range from 15 to 75, with higher scores represented greater knowledge and safer attitudes about concussion, respectively.
Symptom recognition
The 16-item symptom recognition list.

The percentage (%) of respondents who correctly identified the correct symptom are bolded.
Concussion knowledge misconceptions
Knowledge statement responses.
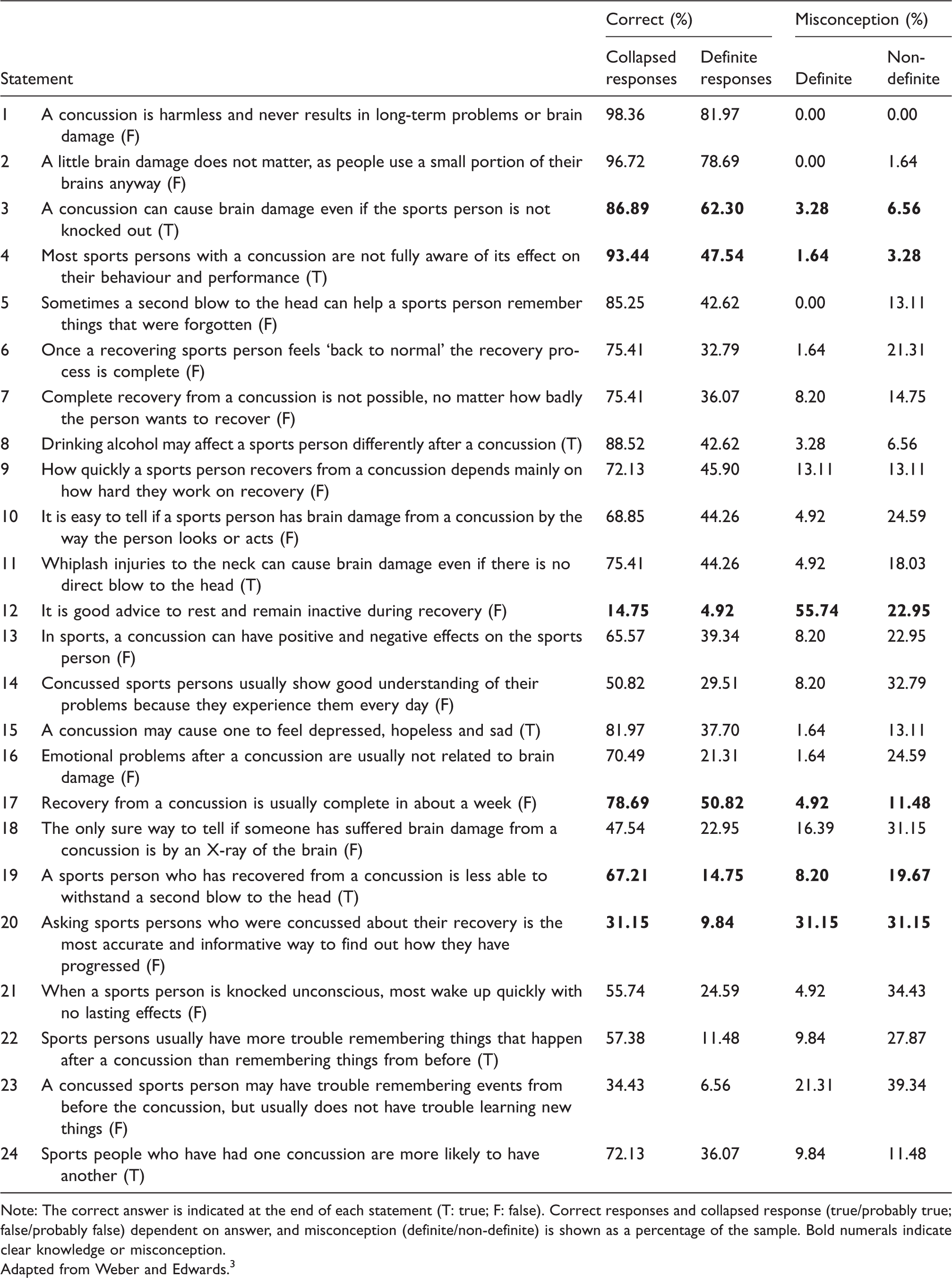
Note: The correct answer is indicated at the end of each statement (T: true; F: false). Correct responses and collapsed response (true/probably true; false/probably false) dependent on answer, and misconception (definite/non-definite) is shown as a percentage of the sample. Bold numerals indicate clear knowledge or misconception.
Adapted from Weber and Edwards. 3
Discussion
Knowledge of and attitudes towards concussion within UK-based male ice hockey players were examined for the first time. Whilst the results of the study found no significant difference between knowledge of and attitude towards concussion across the three levels of competition (professional, semi-professional and amateur), the overall scores across the levels show clear limitations in both knowledge and attitude. Attitude was safest in the amateur level (mean CAI = 59.46) which could be due to a number of factors such as that players at this level generally participate as a hobby and have careers outside of the sport. Although professional and some semi-professional athletes may have the support of team doctors/medics to assess their condition and advise on correct procedures to follow, they may feel a pressure to continue playing, encouraging an unsafe attitude towards concussion.
A players’ concussion history had no significant impact on concussion knowledge or attitudes, suggesting exposure to the injury itself does not necessarily change perceptions of concussion. This supported Weber and Edwards 3 who found that personal experience of sport concussion did not impact the accuracy of concussion knowledge. Furthermore, this relationship partially supports the observations of Register-Mihalik et al. 18 who found no relationship between concussion history and knowledge, but a negative effect on attitudes. This relationship may be driven by multiple variables. For example, recognition of and concerns about concussion disclosure may have limited accurate self-report of concussion history in this study. As noted by Register-Mihalik et al., continued participation post-concussion with no experienced disabilities may negatively impact on perceived severity and importance of concussion itself. Indeed, Weber and Edwards concluded that personal experience of sport concussion might result in a false sense of security. A further note is that concussion history is only operationalised from a personal perspective, and does not consider the potential role of teammates’ concussion occurrences on knowledge and attitudes. The positive relationship between playing experience, CKI and CAI appears to indicate that players early in their career exhibit concerning knowledge and unsafe attitudes towards concussion compared with players with greater experience. Increasing exposure to the sport corrects these shortcomings, and thus highlights early career as a key intervention stage. That concussion history does not influence CKI and CAI suggests that increasing experience of the sport has a separate influence from personal exposure to concussion injury itself, potentially through social, cultural and normative processes.18,19 However, longitudinal data are required to ascertain the processes through which experience plays its role on these variables.
Specific statements from the RoCKAS survey were analysed and showed some accurate knowledge amongst the participants, for example, the majority (93.4%) knew that loss of consciousness was not required for a concussion, which was slightly higher than the knowledge of the football sample (88.5%) in the Williams et al. 13 study. Positively, 72.1% of the participants in this study knew that there is an increased likelihood of repeat concussions after a player has sustained one, as opposed to only 3.8% of the participants in the Williams et al. study. This knowledge is supported by the statement from Weber and Edwards 3 regarding athletes’ abilities to withstand a second blow to the head after previously sustaining concussion as 67.21% said this was true/probably true. Although only 14.75% responded definitely true, suggesting the certainty of knowledge is limited.
Following this trend in increased knowledge within the ice hockey sample, 68.8% were aware that there are long-term risks to health from multiple concussions, compared to the 46.2% in the football sample. Participants in the study indicated safe attitudes towards concussion regarding athletes who lose consciousness in that they should be taken to hospital (85.2%) which is similar to the football sample (80.8%). However, a significantly concerning attitude is that 65.6% of players would continue to play even if they believed they had suffered a concussion (similar to 64% of footballers in the Williams et al. 13 study). That knowledge and attitudes do not appear to mitigate against continuing to play when concussed demonstrates their limitations in explaining behaviour where strong social and normative values also play a critical role.18,19 After more detailed analysis of some of the statements included in the RoCKAS, the results further support the suggestion that the athletes have some accurate knowledge regarding concussion, but this seemingly does not promote a safer attitude towards playing when concussed. This further substantiates Register-Mihalik et al.’s 18 findings that accurate knowledge is not necessarily associated with positive attitudes in athletes. The most common symptoms selected from the list provided were headache, dizziness and difficulty concentrating. However, a low recognition rate was observed for ‘Feeling in a fog’. Some distractor items identified as potential symptoms, although at a low rate, included panic attacks and reduced breathing rate. Together, these results highlight the need for not only education but the development of interventions to encourage safer attitudes towards concussion.
The statements by Weber and Edwards 3 enabled a more in-depth analysis of the knowledge of concussion within the sample and facilitated the identification of correct knowledge, uncertainty and clear misconceptions. The results indicated a trend that collapsed correct responses were noticeably higher than definite correct responses, suggesting a lack of confidence in the respondents’ knowledge, as suggested by Weber and Edwards. 3 The areas that players showed correct definite knowledge were: concussion is harmless and never results in long-term problems or brain damage, 81.97% knew this was false, which is higher than the Weber and Edwards’ general public sample’s definite knowledge of this (74.4%). Another area where players expressed confident knowledge was that concussion can cause brain damage even if the sports person is not knocked out, 62.3% knew this was true, which is again better than the knowledge of Weber and Edwards’ general public sample (50.2%). This result coincides with the findings relating to the knowledge in the RoCKAS that loss of consciousness is not the only way a concussion can occur and that brain damage can occur without losing consciousness. However, clearly a significant proposition of these players did not confidently identify this statement as correct.
The highest level of misconception for these players concerned remaining inactive during recovery from concussion, with 55.74% stating this definitely true (22.95% non-definite). However, it is worth noting that although Weber and Edwards 3 mark this statement false, the efficacy of this approach has not been conclusively demonstrated regarding the relationship between cognitive rest and duration of concussive symptoms (e.g. Gibson et al. 20 ). It may well be inappropriate to conclude fully on the level of knowledge in this area within this sample, but there is still a clear difference in perspective on this statement.
Another misconception was that a concussed athlete may have trouble remembering events from before the concussion, but usually does not have trouble learning new things. This is in fact false, as a long-term effect of concussion is difficulty in learning. 2 In our ice hockey sample, 60.66% misconceived this statement overall (with 21.31% definite misconception) compared to 66% in the general public sample. Suggesting that ice hockey players’ knowledge of concussion is only marginally better than the general public. 3 Whilst 67.2% of the sample thought that once recovered from a concussion an athlete is less able to withstand a second blow to the head, only 14.75% knew it was definitely true. The uncertainty here is a concern given the danger repeated blows to the head (or repeated concussion) hold and the potential for long-term damage, such as chronic traumatic encephalopathy. 21 Regarding assessment of concussion, 62.3% of the sample thought that asking athletes who were concussed about their recovery is the most accurate and informative way to assess progression. Contrasting this, 93.44% of players agreed (47.54% definite; 45.90% non-definite) that athletes with a concussion are not fully aware of its effect on their behaviour and performance. Interestingly, only 36.1% of the general public thought this was true, emphasising the generally greater knowledge within this athletic sample.
A key limitation of the present study concerned accessing teams for participation, with only a limited number of teams available to the researcher resulting in a small sample size. In future, the opportunity to complete the form online could improve uptake. Similarly, the cross-sectional design limited conclusions made on the influence of player experience and concussion history. Longitudinal research is encouraged to assess changes in knowledge and attitudes across playing seasons and careers. Finally, whilst the CKI has been shown to have good reliability and validity, concerns have been raised regarding the CAI’s potential utility. From their data on collegiate athletes, Chapman et al. 17 suggest adding further attitude items focusing sporting, social and normative factors, reflecting the concerns raised above.
Conclusion
To conclude, whilst there are some areas of accurate knowledge and evidence of safe attitudes regarding concussion, there are some clear misconceptions within this male ice hockey player sample. Knowledge regarding loss of consciousness and the effects of this on concussion was better than expected. It can also be concluded that playing experience was positively associated with knowledge of and attitudes towards concussion. These ice hockey players generally had better knowledge of concussion than a general public sample 3 and a sample of professional English soccer players. 13 Attitudes, however, were similar across studies, suggesting that attitude towards concussion may not be specific to individual sports. However, in a worrying contrast to this, 65.6% of the players indicating they would continue to play even if they believed they had sustained a concussion. Such an attitude may undermine any other positive attitude and knowledge regarding concussion, particularly when game status may influence such decision-making in players. For educational programmes to be truly effective, these findings support Provvidenza et al.’s 22 study and highlight specific areas for behaviour and attitude change, encouraging adherence to return to play procedures by educating athletes and coaches on their importance and the potential consequences of non-adherence. Despite positive findings here, such an approach is critical given the existing attitudes towards playing when concussed. This specific attitude poses a significant risk to players’ safety and long-term health.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.