
Abstract
Due to the nature of rugby, concussions are a frequent occurrence and can go undetected by different stakeholders. Knowledge regarding identification of symptoms, management and prevention of re-injury is crucial for the welfare of players. The aim of the study was to determine the concussion knowledge and attitudes among different community club rugby stakeholders. The study gathered quantitative information by utilizing the Rosenbaum Concussion Knowledge and Attitude Survey-Student Version (RoCKAS-ST). Of all the participants (N = 434), medical staff (79 ± 10%) provided the highest Concussion Knowledge Index scores followed by referees (78 ± 8%) and players (67 ± 13%). The stakeholders scored 76% overall for Concussion Attitude Index. Across the scenarios the different participants believed to have safer attitudes compared to that of others within their team. Statistical differences were found between stakeholders when asked if concussion is less important than other injuries, as players, coaches and administrative staff all indicated an unsafe response in contrast to that of referees (p < 0.01). Players indicated an unsafe attitude towards returning to play, while symptomatic as a result of a concussion whereas coaches indicated a safer response (p < 0.01). Only two out of eight legitimate symptoms, headaches and dizziness, were correctly identified by 80% or more of participants, which warrants concern that identification of symptoms could be lacking on this level. Investigating the knowledge and attitudes of concussion at community club rugby level could identify which areas are to be further targeted by the South African Rugby Union.
Introduction
Concussions are a frequent occurrence in rugby union (hereafter referred to as rugby),1–3 which is the world’s most popular team contact sport.4,5 Initial and subsequent concussions have been found to be associated with cognitive, behavioural and physical impairments in affected players. 6 Concussion management should be a shared responsibility across various individuals with specifically assigned tasks or functions within a sport and are referred to as stakeholders. 9 Nevertheless, the concussion knowledge of these stakeholders specifically players,10,11 medical staff, 12 coaches 13 as well as referees 14 have been found to be lacking.
Inadequate knowledge regarding symptoms and/or to intentionally hide subjective symptoms for the purpose of continuing playing may be the rationale for not disclosing concussion symptoms.15,16 Investigations have found that players did not believe the symptoms were serious enough.17,18 The under-reporting of concussions in rugby is not isolated to players only, because it has been linked to the lack in symptom-focussed knowledge in all stakeholders.19,20 A previous study 9 indicated that coaches, out of all the stakeholders (players, coaches, parents, team management, medical staff, administrative staff and referees), perceived themselves to have the greatest responsibility in concussion education. At various levels of play, coaches are responsible for concussion management because of inadequate on-site healthcare personnel. 21 When stakeholders have greater knowledge regarding the consequences of concussion it increases the adherence to post-concussion return-to-play (RTP) protocols. 10 Likewise, concussion attitudes relate to the willingness of players to report symptoms and adhere to the RTP protocol. 22 Attitudes in players towards concussion have also been found to be influenced by numerous factors such as parents, teammates and perceived match importance. 16
In the South African context, amateur (i.e. adult community) players constitute the majority of the playing population and at this level medical assistance could be lacking. 10 Kraak et al. 23 investigated the abovementioned population and found that players scored 67% for concussion knowledge and 62% for concussion attitude. Previous research indicated that 65 to 70% was deemed a moderate level of knowledge and attitude, whereas above 75% was considered sufficient.10,24 Because of the challenges at this level, all the stakeholders within the structure have a part to play in the prevention of concussions. 9 Surprisingly, coaches were among the participants found to have the lowest concussion knowledge in comparison to players, medical staff and referees.12,13 Consequently, if symptoms go unreported and unnoticed the best medical practice for this injury may not be implemented. 25 Walker et al. 11 also found that as many as 79% professional rugby players were not aware that they needed to be cleared by a doctor before returning to play post-concussion.
Education on the symptoms and potential risks to recognize a concussion and to allow for accurate reporting are needed. 7 When looking at concussion education initiatives, many programs have been introduced, but have been met with challenges and mixed results. 11 The purpose of these programs are to reduce the quantity and severity of injuries in community sport. 26 World Rugby’s Rugby Ready, New Zealand’s RugbySmart, Australia’s SmartRugby and South Africa’s BokSmart are all examples of rugby education initiatives. 13 The aim of the BokSmart National Rugby Safety Programme in South Africa is to provide rugby coaches and referees with the knowledge and technical skills to ensure that safety and best practice principles (including concussion management) are incorporated into all aspects of the game.
Numerous tools have been developed to measure the concussion knowledge of stakeholders within sport. One of these measures is the Rosembaum Concussion Knowledge and Attitude Survey-Student Version (RoCKAS-ST) designed by Rosenbaum and Arnett. 27 In 2016, Williams et al. 25 used the same measurement to assess adult football players’ (age: 23.4 ±4.5 years) concussion knowledge and found players scored on average 66% (score: 16.4 ± 2.9 out of a possible 25). The same study by Williams et al. 25 regarding concussion attitude yielded a score of 80% on average (59.6 ± 8.5 out of a possible 75). In 2016, Eagles et al. 28 utilized the RoCKAS-ST, with minor adaptations, to measure the effects of an education program on youth hockey players. 27 The baseline scores were on average 75% for concussion knowledge and 81% for concussion attitude. Kraak et al. 24 assessed hostel rugby players at Stellenbosch University (South Africa) using the RoCKAS-ST and found that in four questions relating to concussion knowledge the players scored less than 50%, indicating apparent misconceptions. 24 The players scored overall 75% for the knowledge section and 81% for the attitude section. As mentioned previously, Kraak et al. 23 also investigated concussion knowledge and attitudes amongst club rugby players in the Western Province Rugby Union (WPRU). Therefore, the aim of the study was to determine the concussion knowledge and attitude among different community club rugby stakeholders.
Methodology
Study design
This cross-sectional study design made use of a questionnaire to collect information on concussion knowledge and attitudes of various stakeholders, i.e. players, coaches, administrative staff, medical staff and referees. The current study included all men and women stakeholders from WPRU club rugby who participated within the annual league. Ethical approval (REC 050411-032) was obtained from the Research Ethics Committee: Human Research at Stellenbosch University.
Participants
Four hundred fifty-seven participants agreed to participate in the study; however, only 434 returned completed questionnaires. The response rate for each stakeholders was established for clubs in Super League A, B and C, where 90 registered players are required, whereas clubs in the remaining zones only require 80 registered players. The response rate for players was 5% (346 out of 7560 players). For coaches, it is estimated that within each club, there are on average 10 coaches, as well as an additional 10 administrative staff. The response rate of coaches and administrators was 4% and 2%, respectively. Referees had a response rate of 18% and medical staff could not be determined because numerous medical staff are assigned by organizations such as ER24. Out of the possible 89 clubs within WPRU club rugby structure, 16 clubs responded to the request to participate in the study, yielding a club response rate of 18%.
The mean age of participants was 27.1 ± 11.1 years, with an average 11.7 ± 7.6 years of experience in the respective roles. The data were collected during the 2018 club rugby season. The aim, purpose and data collection procedures of the study were explained to the participants by the primary researcher. Those who agreed to participate in the study completed an informed consent form, demographic information survey and the RoCKAS-ST questionnaire. Club representative arranged a time and date, which would suit club participants to complete a questionnaire. The participant completed the questionnaires in person (paper based) enabling them to ask questions or electronically. In both cases, they could withdraw from the study at any time during the data collection process.
Data collection procedure
The RoCKAS-ST questionnaire content and subsections were previously described by Rosenbaum and Arnett. 27 The questionnaire is a psychometrically sound scale for measuring concussion knowledge and attitude in high school sport persons. Legitimate questions answered correctly in Sections 1 and 2 received one point, whereas incorrect answered received no points. Eight out of the 16 symptoms were classified as legitimate and made-up a portion of the Concussion Knowledge Index (CKI). The participant with a higher score in the CKI (ranging between 0 and 25) revealed a higher level of concussion knowledge. 26
The Concussion Attitude Index (CAI) was used to determine the views of the participants regarding concussion situations. The range of the answers were between 15 and 75, with a higher tally representing a safer attitude towards concussion. 27 Of the 18 questions which comprised the CAI, three questions were in Section 3 held no index (Questions 3,4,8), and did not contribute to the score. Chapman et al. 29 investigated the reliability of the RoCKAS-ST questionnaire in collegiate sport persons (over 18 years of age) and found the CKI section to be valid and reliable; however, the CAI indicated poor reliability between items in this population. 29 The CAI was subsequently reported as a whole across the entire populations as well as according to the response from each stakeholder as with Sections 3 and 4.
Section 4 was divided into two separate categories namely ‘self’ and ‘others’. The ‘self’ score (SS) related to questions as perceived by the participant themselves, whereas ‘other’ score (OS) was identical questions and asked the participant how they believed a teammate would answer the question. All the uneven question numbers (1, 3, 5, 7, 9) in Section 4 related to scenarios of participants themselves, whereas the even numbers (2, 4, 6, 8, 10) related to how the participants perceived others to react. This concept enables researchers to determine the variation between how the participant would answer and how he/she would perceive others to answer the same question. Finally, Section 5 reports on the concussion symptom checklist.
Data analysis
Statistica 13 Data Processing package (DELL INC version 13.0.159.8) was used to process the data. The data were analysed using descriptive statistics (standard deviations, means, frequencies and percentages). Categorical variables were assessed with chi-square (χ2), whereas mixed model ANOVA’s were used for independent variables with Fisher's least significant difference (LSD) post-hoc analysis. A significance level of 5% was used as guideline for determining significant differences. To determine the CKI and CAI scores, the correct answers were tallied together and divided by the total achievable score of 25 and 75, respectively, and then multiplied by a 100 to provide a percentage score. The 15 questions which made up the CAI were scored on a Likert scale; thus, a minimum score of 15 was required to ensure all questions were answered. Consequently, a score less than 20% indicated an incomplete questionnaire and was disregarded.
Results
Demographic information
The majority 98% (n = 425) of the participants were men, 65% reported involvement on senior level, whereas 21% were at junior level and the remainder were unreported. Out of the 434 participants, 80% (n = 346) were players, 8% (n = 37) coaches, 3% (n = 15) administrative staff and 2% (n = 8) medical staff and 6% (n = 28) referees. Four hundred and fifty-seven participants in total completed the informed consent, 6 players were excluded due to incomplete questionnaires and 17 participants failed to indicate their primary role within the club.
Concussion Knowledge Index
The results of each individual question of the RoCKAS-ST is presented in supplementary Addendum A. Table 1 presents the mean CKI score for all the stakeholders. There was a statistically significant difference overall between the CKI scores of the stakeholders (p < 0.01). Post-hoc analysis indicated that players demonstrated significantly lower concussion knowledge compared to coaches (p < 0.01), referees (p = 0.01) and medical staff (p = 0.01). Administrative staff demonstrated the second lowest concussion knowledge score, reporting significant differences in comparison to referees (p = 0.02), as well as medical staff (p = 0.04).
Concussion Knowledge Index (CKI; %) of the different stakeholders.
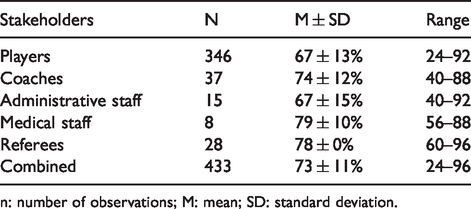
n: number of observations; M: mean; SD: standard deviation.
Interestingly, in Section 1, Question 7, ‘Being knocked unconscious always causes permanent damage to the brain’, coaches reported unsafe responses in scoring only 62%, which was the lowest of all stakeholders. While only 38% of both coaches and medical staff correctly answered Question 17 in Section 1, ‘An athlete who gets knocked out after getting a concussion is experiencing a coma’. Question 13 in Section 1, ‘After 10 days, symptoms of a concussion are usually completely gone’, was reported the lowest by administrative staff (27%).
Concussion Attitude Index
On average, the stakeholders scored 76% for the CAI, with specific responses to the questions highlighted in Table 2. Significant differences (p < 0.03) were apparent between specific stakeholders in Questions 1, 2, 4, 5, 6 and 7. Question 1 presented with statistically significant differences for responses between players and medical staff (p < 0.01) as well as referees and players (p = 0.02), with players indicating the highest willingness to continue play while symptomatic. Question 2 demonstrated statistically significant difference between player and coaches (p < 0.01), where coaches demonstrated a more conservative approach to return-to-play in contrast to players. Question 5 held the widest array, as statistical differences were found between coach and player (p < 0.01) as well as referee and administrative staff (p = 0.01), coaches (p = 0.04) as well as players (p < 0.01). For both Questions 6 and 7, differences were found between players and coaches (p < 0.01 and p = 0.02, respectively) as well as players and referees (p < 0.01 for both Questions 6 and 7).
Concussion Attitude Index (CAI) expressed as a percentage.
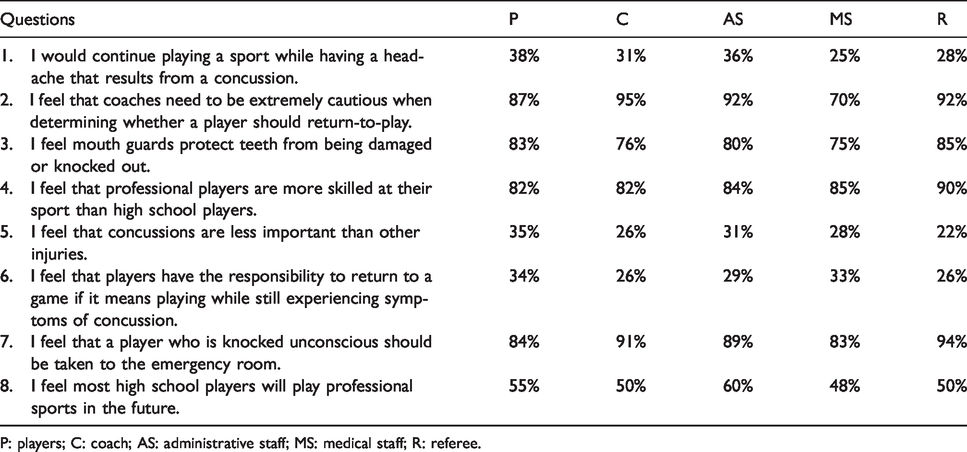
P: players; C: coach; AS: administrative staff; MS: medical staff; R: referee.
The responses by the various stakeholders is represented in Tables 3 and 4, allowing us to compare the responses for ‘self’ versus ‘others’. In Table 3 for Scenario 1, a significant difference was reported in others-score (OS) between both referees and administrative staff (p < 0.01), as well as between referees and players (p < 0.01). Scenario 2 yielded significant differences for both the SS (p < 0.01) and OS (p = 0.04). For Scenario 2, as shown in Table 3, the stakeholders that demonstrated significant difference for SS were between players and coaches (p < 0.01) and between players and referees (p < 0.01). The OS for Scenario 2 was, however, only found to be significant between players and administrative staff (p = 0.03), medical staff and coaches (p = 0.02), as well as administrative staff and medical staff (p = 0.01).
Concussion attitude for self and others for Scenarios 1 and 2.

n: number of observations; M: mean; SD: standard deviation.
Concussion attitude for self and others for Scenarios 3 and 4.

n: number of observations; M: mean; SD: standard deviation
Significant differences for the SS were reported in Scenario 3. The coaches reported the highest score, and significant differences were reported between both coaches and players (p = 0.02), as well as between coaches and medical staff (p = 0.02). Scenario 4 investigated whether players should disclose symptoms of a concussion to coaches regardless of being withdraw from participating. Scenario 4 (Table 4) presented significant differences for both the SS (p = 0.05) and OS (p = 0.02). The significant differences were found in the SS between players and referees (p < 0.01), coaches and referees (p < 0.01), as well as between administrative staff and referees (p = 0.04). The OS reported significant differences between players and medical staff (p = 0.01) with the medical staff reporting the lowest score.
Concussion symptom checklist
By viewing the concussion symptom checklist of Section 5 in isolation, the results indicated that headaches (93%), dizziness (86%) and difficulty remembering (72%) were the most commonly selected (Table 5). A low proportion of participants selected weight gain (3%), hair loss (2%) and arthritis (2%) as possible symptoms. The above-mentioned items were categorized as distractor items; however, the participants still selected them. Difficulty speaking (p < 0.01), sensitivity to light (p = 0.01), difficulty remembering (p < 0.01), drowsiness (p < 0.01), feeling in a ‘fog’ (p = 0.02), difficulty concentrating (p < 0.01) and dizziness were found to be statistically significant symptoms among the various stakeholders.
Concussion symptom checklist for the different stakeholders.
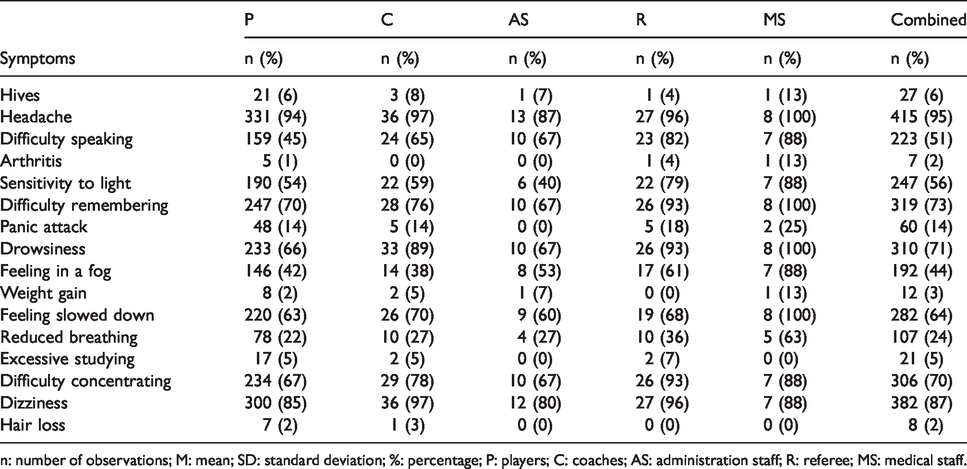
n: number of observations; M: mean; SD: standard deviation; %: percentage; P: players; C: coaches; AS: administration staff; R: referee; MS: medical staff.
Discussion
The aim of the study was to determine the concussion knowledge and attitude among different WPRU club rugby stakeholders. The main findings of the study were that players demonstrated the lowest concussion knowledge and the greatest risk-taking (unsafe) attitude in comparison to medical staff and referees who demonstrated the highest concussion knowledge scores and most cautious attitude towards concussion. The unsafe attitude of players to specific scenarios regarding concussion could lead to premature return-to-play and subsequent concussion with persisting symptoms. Regarding concussion risk-taking, coaches and referees had significantly higher (safer) scores compared to players, which could indicate the value of BokSmart. Coaches and referees are required to attend a compulsory BokSmart workshop bi-annually. As mentioned before, the aim of the workshop is to provide the knowledge and technical skills to ensure safety and best practices. The administrative staff demonstrated the second lowest CKI scores, which warrants concern because they could play a vital role in player welfare. The CKI was higher for senior amateur players than previously reported by Viljoen et al. 10 and similar to research performed by Kraak et al. 23
Concussion Knowledge Index
On average the players scored 67% in the CKI, which was the lowest compared to the other stakeholders. This was deemed insufficient because only scores above 75% have previously been considered sufficient10,25 for concussion knowledge. The players scored lower compared to previous research done by Kraak et al. 25 and Olutende et al. 30 who investigated university hostel rugby and sub-elite rugby players, respectively. The results were, however, higher compared to a similar population of South African amateur players investigated by Viljoen et al. 10 In the study by Viljoen et al. senior players scored 60% which was thought to lead to unsafe behaviour regarding concussion. Coaches (74%) were found to score significantly higher than players (p < 0.01) for concussion knowledge. The divided response by various stakeholders in Question 5 could be due to colloquial terminology used for concussion and thus under-emphasize seriousness. Although still insufficient, the relative higher score obtained by coaches could be because of the compulsory bi-annual BokSmart education workshops.
Referees presented sufficient knowledge scores of 78% similar to medical staff (79%), while coaches were ranked third highest by scoring 74%. In community rugby, coaches are often left with the responsibility of concussion detection and the removal of concussed players because medical support might be lacking. 10 Chinn and Porter 31 also highlighted the coaches’ role in community college rugby in that coaches played an important role in implementing the concussion management protocol. According to Griffin et al. 14 85% of the referees in their study stated they had the final say regarding to whether a player should leave the field. In the current study, the referees yielding the highest concussion knowledge scores, indicated a positive sign. Recently, World Rugby introduced a Blue Card, by which referees or medical staff can order a player with suspected concussion to leave the playing field. This recent change will establish the role referees play alongside medical staff in concussion management during match-play. 32 Misconceptions were still identified within the roles of respective stakeholders, which should be considered for future research initiatives (supplementary Addendum A).
Scoring poorly in Question 13 from Section 1 was a concern because administrative staff previously considered themselves to play a vital role in injury prevention. 12 However, only half of the administrative staff identified that there was long-term health and well-being risks from multiple concussions. Administrative staff can, thus, enforce the prescribed rest period, as well as implement regular screening, 9 thereby preventing subsequent concussions.
Concussion Attitudes Index
The stakeholders in the community club rugby reported a CAI of 76%, which is higher than that reported previously by Kraak et al. 24 and Viljoen et al. 10 It was found that more than a third or players would continue playing the sport even if they had persisting symptoms such as headaches resulting from concussion. Difference within the abovementioned question was found between both players and medical staff (p < 0.01) as well as players and referees (p = 0.02). The results of the fifth question found that there are stakeholders that believe concussion to be less important than other injuries, which warrants serious concern. Specifically, differences in response were found between referees and player (p < 0.01), coaches (p = 0.04) as well as administrative staff (p = 0.01). Question 6 also evoked that there is a lingering pressure to return to play regardless of the symptoms following a concussion. Difference was most commonly found between the players and other stakeholders, with players reporting a less safe response to questions.
Concussion attitudes: Self versus others
Scenario 1 from Section 4 relate to the perceptions of others, when coaches withhold a concussed player from playing a game. Medical staff scored the lowest regarding the opinion of others, compared to referees (p < 0.01) and administrative staff (p < 0.01). The low perceived safety reported by referees regarding the opinion of others could likely be because of prior experiences on club rugby level; however, no research was conducted on referees at this level. Regarding Scenario 2, significant differences were found for the self-score in which players had the highest score, demonstrating the most unsafe behaviour towards match importance determining the RTP. Players, therefore, scored significantly higher than both coaches (p < 0.01) and referees (p < 0.01), which should warrant concern. Similar responses have previously been found among soccer players, indicating that 96% would allow match importance to influence reporting of concussion and RTP. 25
Concussion symptom checklist
The only symptoms identified by more than 80% of all the players were headaches (93%) and dizziness (86%). This is consistent with previous research in which the recognized symptoms were also only two out of eight. 23 The other symptoms, which were often selected, were dizziness (86%), difficulty remembering (72%) and drowsiness (70%). Significant differences were found between the stakeholders for the following symptoms: difficulty speaking (p < 0.01), sensitivity to light (p = 0.01), difficulty remembering (p < 0.01), drowsiness (p < 0.01), feeling in a fog (p = .0.02), difficulty concentrating (p = 0.01) and dizziness (p = 0.01). Administrative staff reported the lowest score for five out of the eight above-mentioned symptoms. Clacy et al. 33 report that there is a great reliance on medical staff to identify symptoms, although at community level, medical staff may not be present at training sessions and/or matches. Cussimano et al. 8 stated that recognition of symptoms leads to decision making regarding diagnosis, treatment, as well as prevention. As these symptoms could be challenging to test, the need for concussion protocols at community level is highlighted.
Conclusion
In conclusion, the results of the study indicated that half of the stakeholders at club level in WPRU had sufficient knowledge regarding concussion with players and administrative staff demonstrating the lowest levels of concussion knowledge. Understanding the knowledge and attitudes towards concussion at community club rugby level might assist in identifying which areas are to be further targeted by the South African Rugby Union. 32 Comparing the CKI of players to that of English football 25 and Canadian hockey 29 players, it is evident that WPRU club rugby yielded noticeably lower scores. CAI indicated an overall score of 76% for all stakeholders; however, within specific questions, a proportion of players demonstrated unsafe attitude towards concussion. Limitations of the study could include that the questionnaire was originally designed for student-athletes and not coaches, medical personnel, administrative staff or referees and thus comparison of other stakeholders should not be generalized. Limitations also include the sample size of the medical staff, as well as the variance in the type of medical staff, which should be specified in future studies. The low response rate by club stakeholders inhibits the generalization of results as to the entire union’s club rugby population. The low response rate could indicate a non-response bias, and trademarks of respondents and non-respondents could differ. There are also numerous limitations associated with incorporating (ad hoc) measurements that have not been trailed for validity and reliability. For future studies, the focus should be placed on all levels of competition, as concussion occurs at all levels of participation.
Supplemental Material
SPO913175 Supplemental material - Supplemental material for Concussion knowledge and attitudes amongst community club rugby stakeholders
Supplemental material, SPO913175 Supplemental material for Concussion knowledge and attitudes amongst community club rugby stakeholders by Hanno van Vuuren, Karen Welman and Wilbur Kraak in International Journal of Sports Science & Coaching
Footnotes
Acknowledgements
The authors would like to thank the different stakeholders who participated in the study, as well as Professor Martin Kidd of the Centre for Statistical Consultation, Stellenbosch University, for assisting with the statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.