
Abstract
Anterior cruciate ligament (ACL) injuries significantly impact athletes’ performance, and a neurocognitive approach, particularly executive functions, may play a relevant role in ACL injury. The aim was to evaluate and compare performance on inhibitory control and visual attention using the Flanker Task and Multiple Object Tracking (MOT) cognitive tests between athletes with and without a history of non-contact ACL injury. 60 athletes of interaction sports (30 athletes with no history of ACL injury and 30 athletes with a history of non-contact ACL injury) participated in this study. During the experimental session participants performed Flanker Task and Multiple Object Tracking to evaluate inhibitory control and visual attention, respectively. Athletes with a history of non-contact ACL injury had longer reaction times than healthy athletes on the Flanker Task cognitive test (p < 0.001). For the MOT, athletes with a history of non-contact ACL injury had worse two-ball follow-through at speeds of 19.9 deg/s (p = 0.034) and 28.8 deg/s (p < 0.001) and three-ball follow-through at speeds of 19.9 deg/s (p = 0.009) and 28.8 deg/s (p < 0.001). Athletes with a history of non-contact ACL injury exhibit poorer cognitive performance than athletes without a history of ACL injury in inhibitory control, particularly interference control and visual attention. Therefore, rehabilitators and exercise professionals should consider the assessment and training of executive functions into the rehabilitation process for ACL injuries.
Introduction
Anterior cruciate ligament (ACL) injury is one of the injuries with the most significant impact on athletes’ motor performance and quality of life. This injury is more common in interaction sports such as basketball, football or lacrosse and tends to affect women more than men. 1 ACL injury hurts the ability of affected athletes to return to competitive activity and regain their previous levels of athletic performance. Therefore, interest in understanding the risk factors for this type of injury has increased considerably.
These factors are complex and varied: biological, mechanical, hormonal and psychosocial, making it difficult to approach the study of the reasons that could lead to it. ACL injury can occur with or without contact in sporting contexts, especially in interaction sports. According to Boden and Sheehan, 2 non-contact injuries occur 70% of the time, with changes of direction and one-legged landings being the most common sporting gestures that trigger it. It is known that the ACL is mainly responsible for stabilising the knee against anterior tibial translation, rotational movements and hyperextension of the knee, 3 so these sporting gestures performed under demanding competitive conditions could contribute to non-contact ACL injury.
Despite the knowledge of the function of the ACL and the sporting gestures where the injury tends to occur, there is controversy in explaining the possible causes. One of the most widely supported factors is axial compressive forces. When these exceed the endurance capacity of the ligament, damage to the structure can occur. 2 However, other potential factors such as knee abduction, the way the heel is supported during landing or poor core stability 4 arouse controversy suggesting further studies to clarify their influence. However, despite advances in sports training and improvements in the incidence of other sports injuries, 5 ACL injury continues to increase worryingly. 6 All this has sparked researchers’ interest in a new perspective of analysing the problem from a hitherto little-considered area: the role of cognition in ACL injury. 7
Athletic performance in interaction sports is linked to the athlete's ability to adjust his or her behaviour quickly and flexibly under high variability conditions. 8 The quality of the athlete's decisions is linked to the ability to selectively direct attention to relevant information and thus readjust their intentions according to the game's requirements. However, current injury prevention strategies are still based on movements that aim to improve physical skills such as strength or flexibility but with little or no demand for cognitive control. 9 This implies that such movements are far from replicating the unpredictable conditions of real competition contexts. 10 The ability to respond to these demands affects athletic performance and has also been linked to the emergence of mechanisms associated with ACL injury risk. 11
Executive functions are cognitive skills that enable individuals to plan, organise, monitor and evaluate their actions to achieve a goal. 12 The development of executive functions has been found to contribute to improved sporting performance. 13 According to Diamond, 12 three basic executive functions can be identified: (1) working memory (WM), the ability to store information temporarily in order to process it efficiently; (2) cognitive flexibility (CF), the ability to change thoughts, behaviours and strategies to adapt to changing situations and (3) cognitive inhibition (CI): the ability to control or inhibit automatic responses or impulses, thus avoiding the performance of inappropriate or maladaptive actions. The latter encompasses interference control, which involves consciously selecting which stimuli are relevant to direct behaviour towards a particular goal while ignoring those that interfere with that goal. 12 This process allows us to focus on a specific task, such as anticipating an opponent's action, based on certain pre-indexes that allow us to foresee their future behaviour while avoiding being distracted by irrelevant elements such as the position of other players or the noise from the stands. 14
Beyond the relevance of executive functions for sports performance, it has been observed that they may play a relevant role in preventing ACL injury. 15 Non-contact ACL injury occurs predominantly in open and unplanned actions. 16 In these situations, the athlete must adjust their motor behaviour quickly and precisely, which may favour the development of mechanisms associated with ACL injury. In the same vein, it has been observed that movement coordination inaccuracies can restrict the muscles’ ability to perform the compensatory contractions required to mitigate impact forces on the joint. 17 Also, the need to process and select a large amount of information quickly may compromise both the motor response and the decision made. 15 In this regard, a systematic review concluded that low-order executive functions may be a potential predictor of musculoskeletal injury risk. 9
Few studies have analysed the bidirectional relationship between executive functions and ACL injury. This study aims to examine the possible association between ACL injury and cognitive function, especially interference control and visual attention. To this end, performance on the Flanker Task and Multiple Object Tracking (MOT) cognitive tests will be compared between athletes with and without a history of non-contact ACL injury.
Materials and methods
Participants
60 participants were recruited. The sample was divided into two groups: 30 athletes with no history of ACL injury (healthy athletes) and 30 athletes with a history of non-contact ACL injury (ACLR athletes). Data regarding age, gender, weight, height and sport modality practised were collected for each. All study participants were interaction sports athletes. The demographic data of the participants are available in Table 1. This study was conducted per the Declaration of Helsinki and was approved by the university's institutional review board (approval no: 3110/ CEIH/2022).
Descriptive statistics of the sample.

Data values are expressed as mean ± standard deviation. N, Sample Size; M, Meters; Kg, Kilograms; BMI, Body mass index
Participants were selected based on the following inclusion criteria: 1) young adults aged 18–35 years, 2) active athletes in interaction sports, with a minimum of 3 years of continuous experience in federated sports and performing at least two training sessions per week in their specific discipline.
Furthermore, participants were not selected based on the following exclusion criteria: 1) history of brain injury or severe head trauma, 2) impaired or uncorrected vision, and 3) diagnosis of psychiatric or neurological disorders, cardiovascular or metabolic diseases. Additional criteria were used to assign participants to each group. For the group of athletes who had suffered a non-contact ACL injury, it was necessary that they were medically cleared or that at least one year had passed since the ACL reconstruction surgery. For the other group, participants had to have no history of ACL injury.
Procedure
Familiarisation session
In the familiarisation session, participants received a detailed presentation of the research and detailed instruction on the procedures and assessments they would carry out in the experimental session. In addition, participants gave their written consent to participate. They were then able to practice all the cognitive tests until they had a full understanding of them. This session lasted approximately 30 min.
Experimental session
The experimental session took place in one of the laboratories of the Faculty of Sports Science of the University of Granada. This was a quiet, noise-free place where the session could occur without interruptions or distractions. Participants were asked to abstain from caffeine, theine or alcohol ingestion during the previous 24 h, sleep at least seven hours the night before, fast during the previous four hours and avoid strenuous exercise during the 48 h prior to the experimental session, to avoid the possible moderating effect of certain variables. The experimental session lasted approximately 45 min.
Participants performed two computer-based cognitive tests in counterbalanced order during the experimental session. Thus, the order of the tests could not explain or alter the results obtained. The cognitive test battery was intended to measure some of the primary executive functions (working memory and cognitive inhibition) as described by Diamond. 12 Specifically, this study aimed to assess interference control, which belongs to the family of functions that comprise the cognitive inhibition types. 18 In addition, visual attention was also assessed.
Flanker task
This assessment aimed to evaluate interference control.
19
Participants were instructed to respond in the direction of a white arrow displayed in the centre of the computer screen. They were required to press the left shift button with their left index finger when the arrow pointed to the left (i.e., “<”) and press the right shift button with their right index finger when the arrow pointed to the right (i.e., “>”). The task encompassed four different flanker conditions:
Congruent: Arrows oriented in the same direction (e.g., “< < < < < < < < <” or “> > > > > > > >”). Incongruent: Arrows oriented in different directions (e.g., “> > > < < > > > >” or “< < < > < < < <”). Neutral: The central arrow is presented alone (e.g., “<” or “>”). Dash: The central arrow without any distractor stimulus (e.g., “–<” or “→”).
The test comprised 172 trials organised into the following sequence within each block: 12 practice trials initially, followed by 40 congruent trials, 40 incongruent trials, 40 neutral trials, and 40 dash trials presented randomly. Each experimental trial was initiated with a 500 ms presentation of a white fixation “cross” symbol in the computer screen's background. Subsequently, a stimulus was displayed for 800 ms, followed by an inter-stimulus interval of 1000 ms. The primary outcome measures included accuracy and mean response times for each type of trial.
Multiple object tracking
The MOT task assess the ability to sustain attention for a prolonged period, distribute attention across multiple items, and select specific objects to actively track. In this cognitive test, eight identical grey balls (radius = 0.4°) were projected onto a 27-inch monitor (ASUS VA27EHE, Taipei City, Taiwan) located 50 cm from the participant at a visual angle of 25°. The MOT task is graphically represented in Figure 1.
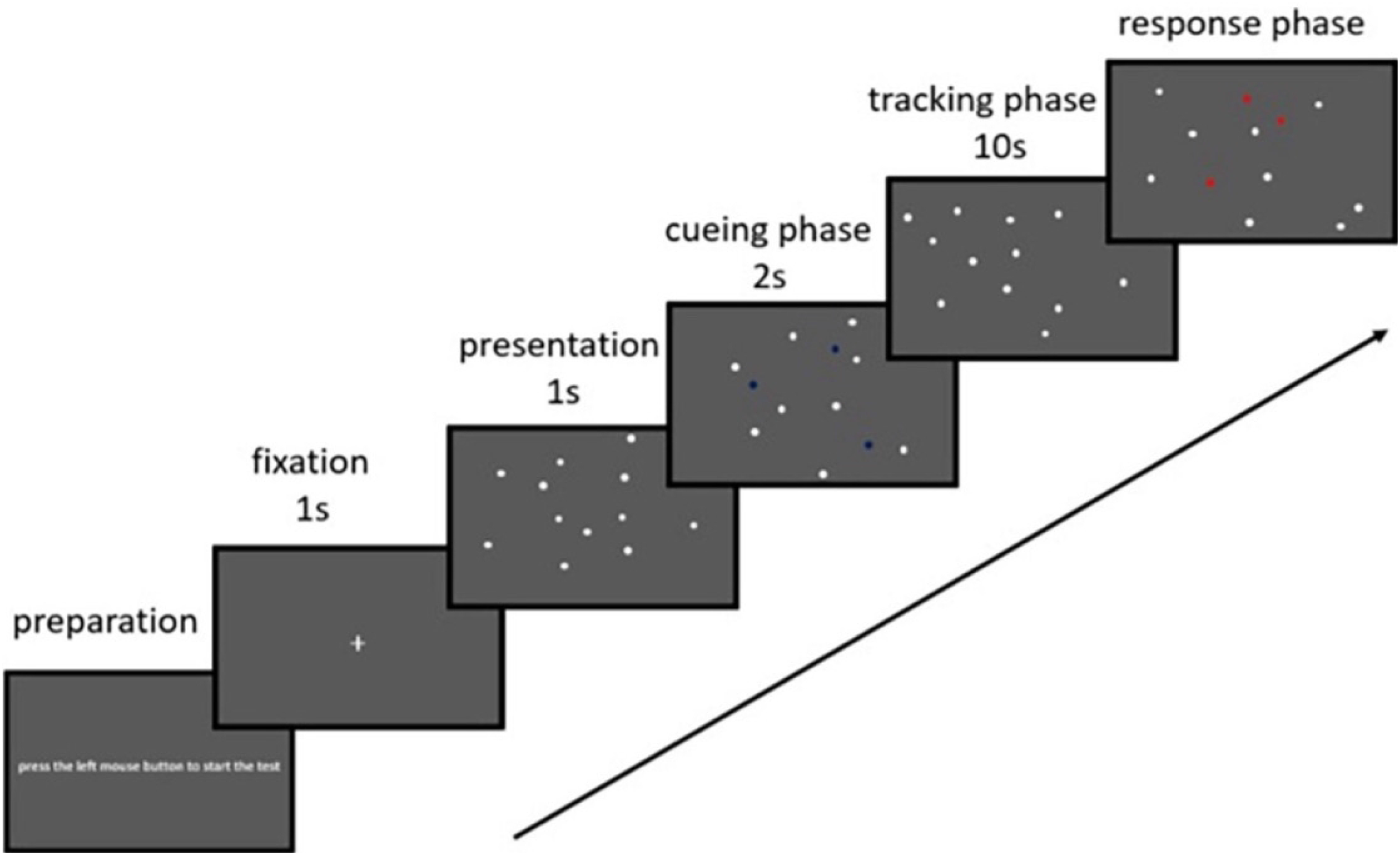
Multiple object tracking (MOT) task. 20
For 2 s, two balls were randomly illuminated in green. After this time, they returned to grey, and all balls started to move randomly in space for 5 s. The participant had to keep track of the balls lit up green. When they stopped, a number from 1 to 8 was randomly assigned to each ball. On each trial, the participant was asked to identify the illuminated balls at the start, specifying the number assigned to each. 21 About the speed of the balls, five speeds were set (6.4 deg/s, 9.3 deg/s, 13.7 deg/s, 19.9 deg/s and 28.8 deg/s). For each speed, five repetitions were performed. The same protocol was then followed by tracking three balls.
The test's performance was established for each speed from the average hit percentage across all repetitions. For example, in the case of three-ball tracking, for speed 28.8 deg/s, the total number of balls hit was summed and divided by 0.15, as 15 was the maximum number of hits that could be achieved.
Statistical analysis
First, all variables of interest were grouped to obtain descriptive statistics. Subsequently, to evaluate whether there are differences between healthy and ACLR individuals in the performance of the Flanker Task and MOT tests, an independent samples analysis was conducted. A t-test was used if the data met the normality assumption, or the Mann-Whitney test if they did not.
The effect size for the t-test was calculated using Cohen's d, interpreted as a small effect when the value is between 0.2 and 0.5, medium when the value is between 0.5 and 0.8, and large when the value exceeds 0.8. For the Mann-Whitney test, effect size was calculated using r, interpreted as a small effect between 0.1 and 0.3, medium between 0.3 and 0.5, and large when it exceeds 0.5. The p-value was set at 0.05, and the statistical analysis was performed using RStudio v.2024.04.2. Both the database and the R code used for this study are available on the following open-access page for community access: https://osf.io/375hy/.
Results
Descriptive results
Table 2 shows the means and standard deviations for each variable of interest. Additionally, the Shapiro-Wilk test indicated that some variables met the normality assumption while others did not. Therefore, parametric and non-parametric statistics were used as appropriate.
Descriptive statistics of the study variables for the entire database and separated by healthy and ACLR athletes’ sample.
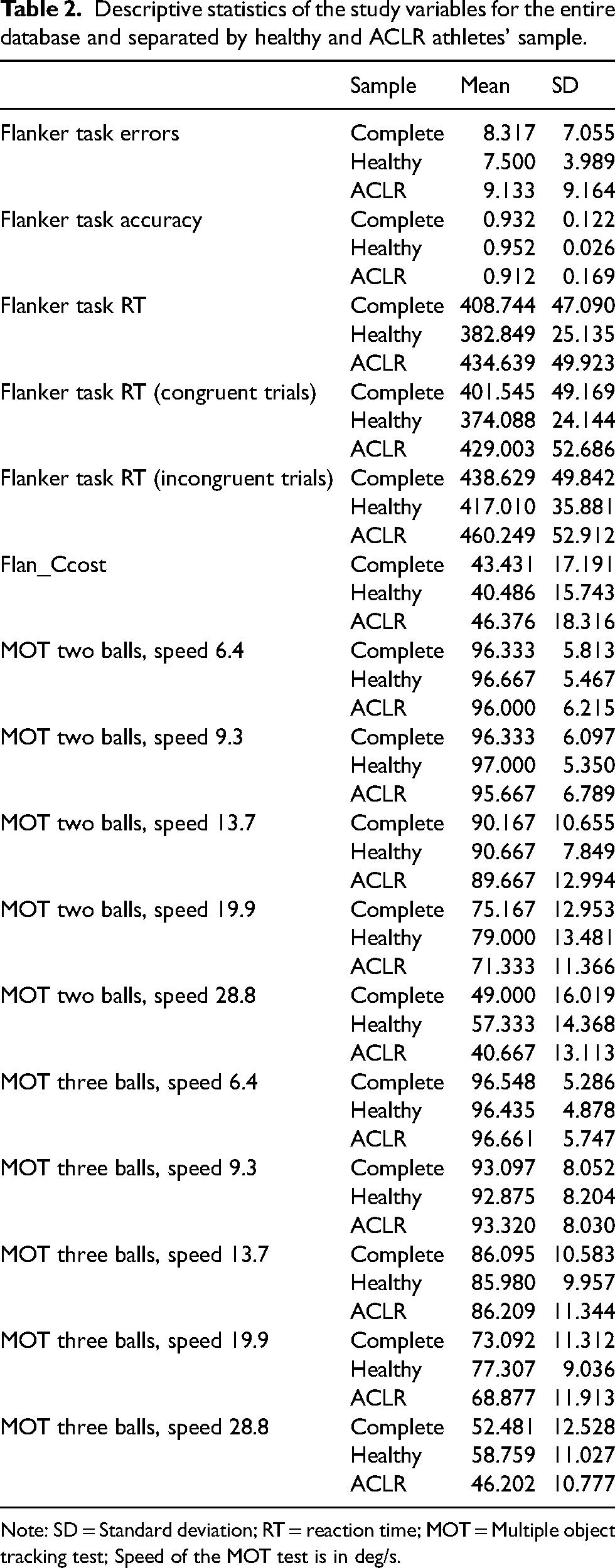
Note: SD = Standard deviation; RT = reaction time; MOT = Multiple object tracking test; Speed of the MOT test is in deg/s.
Flanker task differences between groups
For the Flanker Task, differences between the healthy and ACLR athletes were observed only in reaction time, both overall (t = −5.075; p < 0.001; d = −1.1) and when separated by congruent (t = −5.19; p < 0.001; d = −1.16) and incongruent stimuli (t = −3.705; p < 0.001; d = −0.867). In all cases, the healthy athletes had a lower reaction time. These results are graphically represented in Figure 2. Finally, no significant differences were found in accuracy (W = 404.5; p = 0.504) and error count (W = 497.5; p = 0.485).
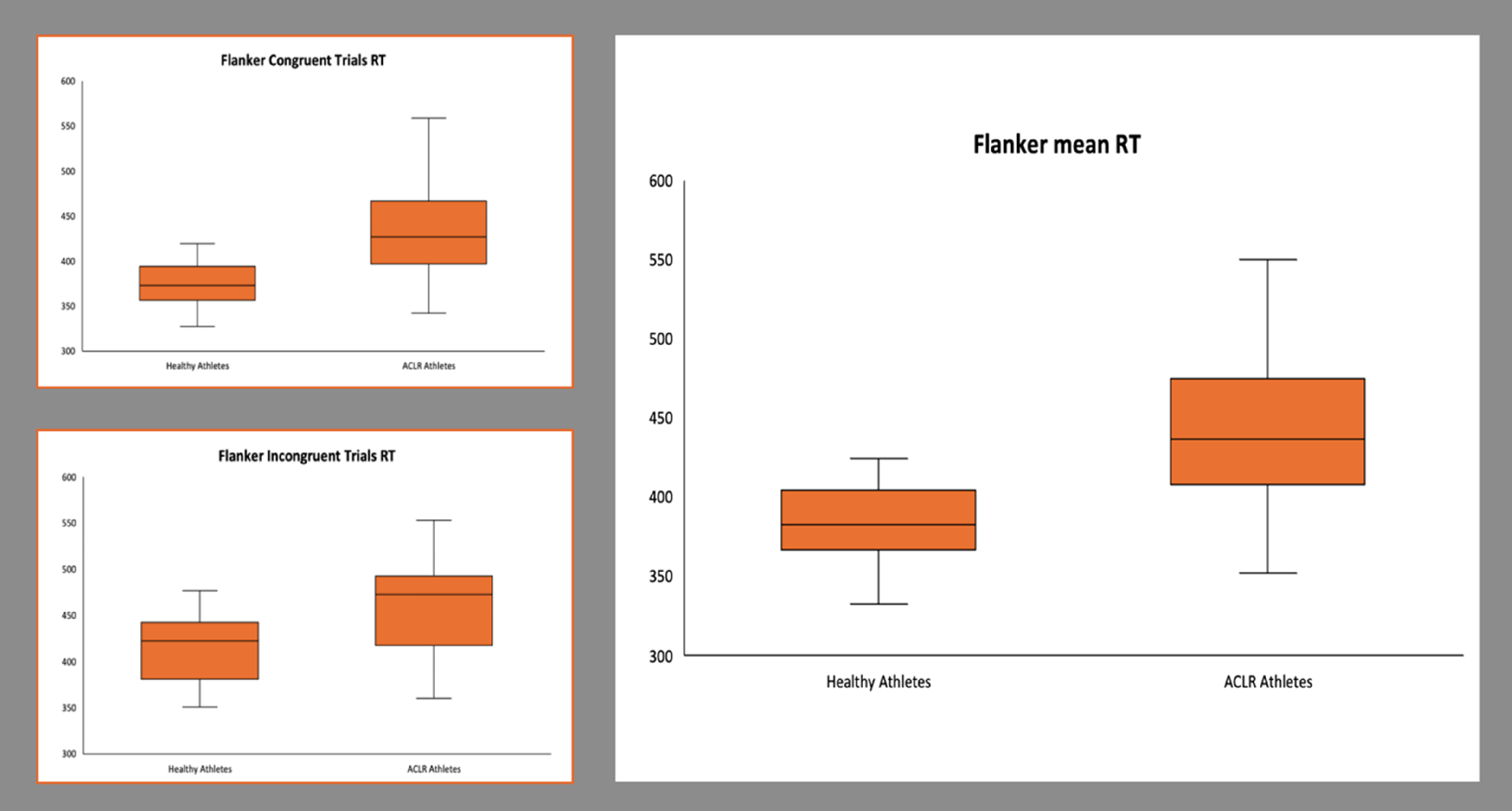
Healthy and ACLR athletes’ differences in Flanker task mean reaction time and congruent and incongruent trials reaction time.
MOT differences between groups
For the MOT, significant differences between healthy and ACLR athletes were observed at speeds of 19.9 and 28.8 deg/s, regardless of the number of balls to find, whether two balls [speed 19.9 (W = 589.5; p = 0.034; r = 0.674); speed 28.8 (W = 717; p < 0.001; r = 1.349)] or three balls [speed 19.9 (W = 624.5; p = 0.009; r = 1.006); speed 28.8 deg/s (W = 722.5; p < 0.001; r = 0.677)]. In all cases, the healthy athletes performed better than the ACLR athletes. These results are visually represented in Figure 3.

Healthy and ACLR athletes’ differences in Multiple Object Tracking.
Therefore, no significant results were observed in the other parts of the test: finding two balls at speed 6.4 deg/s (W = 469; p = 0.736), at speed 9.3 deg/s (W = 487; p = 0.501), or at speed 13.7 deg/s (W = 428; p = 0.734); finding three balls at speed 6.4 deg/s (W = 410.5; p = 0.508), at speed 9.3 deg/s (W = 428.5; p = 0.745), or at speed 13.7 deg/s (W = 394.5; p = 0.412).
Discussion
The main purpose of this study was to evaluate and compare cognitive performance between athletes with and without a history of non-contact ACL injury on the cognitive tests Flanker Task and MOT. ACLR athletes were expected to have worse cognitive performance than their healthy peers. This study found that athletes with a history of non-contact ACL injury had longer reaction times on congruent and incongruent trials (mean reaction time) than healthy athletes on the Flanker Task cognitive test. Likewise, the athletes with a history of non-contact ACL injury had worse two- and three-ball follow-through at speeds of 19.9 and 28.8 deg/s. However, no significant differences existed for 2-ball and 3-ball tracking at any of the other speeds. These results suggest that, despite having completed the rehabilitation process, athletes with a history of non-contact ACL injury have worse cognitive performance than athletes without a history of ACL injury.
The importance of cognitive inhibition, especially interference control, on performance in interaction sports is well known. 22 In this study, athletes with a history of non-contact ACL injury had a longer response time in the flanker task, indicating greater difficulty in processing and resolving visual information conflicts than athletes without a history of ACL injury. This suggests that athletes with a history of non-contact ACL injury may have poorer selective attention and inhibitory control. The ability to perform these processes efficiently is key in changing and uncertain environments such as interaction sports. The anterior cingulate cortex plays a key role in both processes, 23 as it is particularly involved in filtering out distracting elements and focusing on relevant stimuli. This increase in response time could be linked to a dysfunction or less efficient connection between the peripheral nervous system (which captures and transmits sensory information) and the central nervous system (which processes and responds to this information). Proper interaction between these systems is crucial for fast stimulus processing, more effective conflict monitoring and better performance in tasks requiring inhibitory control. 24 Thus, athletes without a history of ACL injury appear to have better interference control, suggesting that they can allocate their attentional resources, better organisation of neural networks and more efficient top-down cognitive control 25 than athletes with a history of non-contact ACL injury.
The ability to sustain visual attention during complex coordination actions is critical to reducing the risk of ACL injury. 7 The MOT task identified differences between athletes with no history of ACL injury and athletes with a history of non-contact ACL injury for some speeds. Interaction sports players performed better on tasks requiring visual attention, probably due to the variability they are exposed to in their training modalities. 26 Because both groups in the present study are amateur players of these types of sports, the MOT task could only differentiate performance between the two groups in visual attention at higher speeds. This may be because the other (lower) speeds did not challenge the participants, given the cognitive resources of both groups of athletes. According to the challenge point framework, the difficulty of a task is linked to a greater extent to its functional difficulty (how challenging the task is considering the skill level of the person performing it) than to its nominal difficulty. 27 Optimally matching the task's difficulty to the participant's abilities could help find differences between the two groups. ACL injury often occurs in environments with high mental workload, i.e., situations that require high cognitive demand from the athlete. 28 In this context, visual attention training, such as through visual perturbation, may play a key role in enhancing proprioception-related sensory neural processing and improving the efficiency of visuomotor processing after ACL injury. 29
Currently, studies that analyse ACL injury from a cognitive perspective are scarce. Most studies that evaluate cognitive performance in ACL-injured individuals focus on basic cognitive skills such as attention, reaction time, or processing speed in tests that do not assess higher-order cognitive skills (executive functions). The systematic review by Wilke and Groneberg 9 concluded that basic cognitive skills predicted injury occurrence. In that study, it was reported that the reaction times of the injured individuals were significantly longer than those of the healthy participants, which aligns with the results obtained in the present study. Furthermore, executive functions are essential for athletic performance, especially in interactive sports, as the environment constantly changes. 30 Athletes need to process the appropriate information to perform the action that adapts to the demands of the environment. 31 Consequently, athletes at a higher competitive level show behavioural and electrophysiological advantages compared to amateur athletes. 32 As uncertainty increases, when game situations become more unpredictable and challenging, athletes are forced to adapt and adjust their motor behaviour. All of this implies a greater consumption of the available mental resources for information processing. 33 This also plays a crucial role in understanding the causes linked to ACL injuries.
On the one hand, cognitive control plays a significant role in information management when the available time is limited and the level of uncertainty is high. In these situations, the athlete must inhibit inappropriate responses (cognitive inhibition) and develop strategies that, at a technical-tactical level, adapt to the demands of the game without being distracted by irrelevant stimuli. 34 When the athlete cannot make these adjustments because of excessive temporal demands, the mechanisms related to the increased risk of suffering an ACL injury are enhanced. 11 On the other hand, a reduction in communication between brain regions and the excitability of cortico-spinal pathways has been observed both before and mainly after ACL injury. 35 In this regard, Diekfuss, Grooms 36 noted that athletes who did not suffer ACL injuries showed a stronger functional connection between one of the cerebellar regions responsible for balance and coordination and a sensorimotor cortical region. Similarly, it has been reported that lower cognitive performance may be associated with a higher risk of injury and poorer motor performance upon returning to competition. 35
It can be hypothesised that cognitive function is linked to the risk of injury and can also be affected after this pathology. The ACL injury could cause neural modifications through the afferent disruption due to the ligament rupture. 37 Disruption involves altering the information that certain mechanoreceptors send to the central nervous system through the dorsal column medial lemniscus pathway. Additionally, it has been observed that ACL injury causes changes in the structure of the corticospinal tract, whose negative effects are exacerbated over time. 38 In the same way, these mechanical alterations and sensory deficits, particularly in proprioception, are primarily caused by swelling of the knee joint capsule and damage to mechanoreceptors within the ACL itself. 39 Such sensory disruptions may contribute to maladaptive neuroplasticity in the somatosensory and motor cortex. 38 Consequently, impairments in sensorimotor integration could influence cognitive-motor interactions, 40 potentially affecting decision-making and motor adjustments in uncertain environments, thus increasing the risk of reinjury. 41 Due to anatomical damage to the sensory pathways, this decrease in afferent information could affect representational movement models. 42 These models are critical for accurately predicting and adjusting movements based on sensory feedback. This phenomenon creates an ‘up-down’ control problem, where the information the brain receives from peripheral levels is insufficient to adjust movements efficiently. 43 When this information is compromised, the nervous system's ability to predict and adjust motor patterns is limited, affecting adaptation to environmental changes and accuracy in motor execution. In this regard, cortical reorganisation following ACL injury may require compensatory strategies 35 that, in uncertain environments, would not be sufficient to achieve good decision-making while making the necessary motor adjustments to avoid the risk of ACL injury. Therefore, in the rehabilitation programmes for ACL injuries, variables such as executive functions should be taken into account since traditional postoperative rehabilitation processes do not succeed in cognitively rehabilitating athletes. The manipulation of cognitive demands in tasks (for example, increasing uncertainty or including the dual-task paradigm) could be an effective tool to prevent future recurrences. 44 Nevertheless, these observations are based on a cross-sectional study, and any rehabilitation recommendations should be validated through longitudinal studies or specific intervention trials.
The hypothesis of the work could be confirmed, which indicates that the design and the selected cognitive tests allowed for the detection of differences between both groups. However, it is necessary to present some considerations for future work. First of all, cognitive tests are not adjusted to the athlete's individual performance. In competitive contexts, athletes’ performance is affected when the difficulty of handling and responding to information exceeds their physical and cognitive abilities. For that same reason, it would be interesting to check performance in cognitive tests where participants are suitably challenged by their difficulty. Secondly, this study could be replicated by analysing the evolution of cognitive performance at different stages of rehabilitation. One possibility would be to take three measurements: in the preoperative period, in the postoperative period, and at the end of the rehabilitation process. Consequently, a more comprehensive understanding of the relationship between cognitive factors and ACL injury could be achieved.
Conclusions
Athletes with a history of non-contact ACL injury show worse cognitive performance than athletes without a history of ACL injury in cognitive inhibition, particularly interference control and visual attention. Despite having completed the rehabilitation process, athletes with a history of non-contact ACL injury do not achieve cognitive performance similar to athletes without a history of ACL injury. Consequently, rehabilitators and exercise professionals should consider the work and evaluation of executive functions during the rehabilitation process of ACL injuries.
Footnotes
Acknowledgements
The authors of this work would like to express their most sincere thanks to Ángel Povedano Arévalo for his invaluable help and for his collaboration in carrying out this study.
Author contributions
FAL and JJM devised the study. JJM, FAL, and DCV developed the methodology and interpreted the data. JJM and AGC carried out the data collection. IMC conducted the data analysis. JJM wrote the initial draft of the manuscript. The manuscript was critically revised by JJM, AGC, IMC, FAL, and DCV. FAL and DCV supervised the study. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Informed consent was obtained from all participants involved in this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This original research was funded by the Spanish Ministry of Science, Innovation and Universities: Grant FPU19/06224 and Spanish Ministry of Universities: Grant FPU20/02022. This study is part of a PhD thesis conducted in the Biomedicine Doctoral Studies program of the University of Granada, Spain. Funding for open access charge: Universidad de Granada/CBUA.