
Abstract
In a context in which research evidence indicates high rates of alleged sexual victimization among adults with psychosocial disabilities, this article draws upon rape allegation data collected by the Metropolitan Police Service in April and May 2012, to explore some of the challenges that are posed to the criminal justice system by these types of complainants. Although the insights that can be generated from these data in relation to complainants with psychosocial disabilities are limited, in the context of this article it provides a valuable snapshot into contemporary patterns of rape victimization and attrition in England and Wales. It also serves as a useful stepping off point from which to highlight the need for more sustained critical research and reflection on the treatment of complainants, and the adequacy of police and prosecutor training and practice in this area.
Introduction
It is widely acknowledged that recent decades have been marked by a shift (in theory, if not always in practice) towards a more ‘victim-centred’ approach to criminal justice in England and Wales (Home Office, 2002, 2012, 2013; Jackson, 2003). Initiatives have been designed, for example, to assist vulnerable witnesses in the process of giving their testimony in the adversarial environment of the courtroom, to give added weight in sentencing decisions to statements from victims of crime regarding its impact and to improve the infrastructures of support that are routinely provided to victims with special needs. Despite this, however, concerns have continued to be expressed – and, indeed, with growing momentum – regarding the handling of allegations of victimization which are made by complainants with a history of and/or a current diagnosis of mental illness or, more broadly, psychosocial disability (hereafter PSD) (Mind, 2007; Pettitt et al., 2013). In this article, we explore some of the challenges that are posed to the criminal justice system by these types of complainants, focusing particularly on the context of rape allegations, where a number of the barriers in relation to disclosure and credibility that critics suggest are faced by those with mental health concerns may be compounded further by tenacious cultures of scepticism and victim-blaming (Horvath and Brown, 2009; Kelly et al., 2005; Temkin and Krahe, 2008). We highlight the surprising extent to which, despite the ways in which the treatment of complainants with mental health problems can be seen to be a litmus test for the success of ‘victim-centred’ criminal justice, remarkably little is known about the scale of sexual victimization experienced by this constituency, the effectiveness of police and prosecutors in responding to such complaints appropriately and the influence of mental health diagnoses (in all their diversity) on assessments of the allegation’s credibility and the prognosis for successful prosecution. To do so, we draw upon a variety of sources, including data recently collected by the Metropolitan Police Service in relation to a sample of rape allegations made in April and May 2012. Although, as we discuss below, the insights that can be generated from these data in relation to complainants with PSD are limited (for fuller discussion of what can be gleaned in relation to rape prosecution more generally, see Hohl and Stanko, in preparation), it provides a valuable snapshot into contemporary patterns of rape victimization and attrition in England and Wales. As such, it offers a starting point for future research that can begin to explore in a more targeted fashion the scale of reporting, factors influencing attrition and experiences of criminal justice professionals, as well as complainants, in handling this genre of rape allegation.
The following discussion falls into four main parts. In the first section, we explore the current evidence base in relation to the scale of alleged sexual assault and rape victimization among persons with mental distress or PSD. In so doing, we also reflect upon the obstacles to formal disclosure of such assaults. Following the prosecution process through from the point of disclosure, in the next section, we reflect on what we currently know about patterns of attrition in these cases, as well as the difficulties faced by agents of the criminal justice system in correctly identifying complainants with mental health issues and dealing with initial disclosures in an appropriate manner. We will situate our discussion within a broader context in which the overall scale of attrition in rape cases continues to be a source of considerable concern, but will also pay specific attention to the ways in which a lack of victim support, barriers in relation to producing a ‘credible’ account and concerns regarding the complainant’s ability to cope with the rigours of the trial process (particularly cross-examination) can have a particularly pronounced impact in relation to allegations from those with mental health concerns (or a history thereof). Having sketched over these sections the current state of knowledge in relation to the operation of criminal justice in these cases, in the third section, we provide an outline of key findings in relation to the handling of rape allegations from persons with mental health issues by the Metropolitan Police Service. Though limited in its scale, and not designed specifically to ‘drill down’ on issues relating to PSD complainants, we suggest that these rarely available data are valuable in both supporting several of the trends identified in previous research and providing a snapshot of contemporary criminal justice responses in England and Wales – including the potential shortcomings that they may exhibit. In a context in which there is much concern, but also much conjecture, regarding the handling of rape complainants by persons with PSD, we will use the Metropolitan Police data as a starting point from which, in the final section of this article, to highlight the need for more sustained critical research and reflection on the treatment of complainants, and the adequacy of police and prosecutor training and practice in this area. It will also briefly explore how insights from such research would be invaluable in contributing to the strategic working partnership of a number of statutory and non statutory bodies, involved in public mental health and victimization such as the Department of Health, Crown Prosecution Service and the Royal College of Psychiatrists.
Before embarking on this discussion, however, it is appropriate and important to make a brief point regarding terminology. In the above discussion, we have at times utilized the general language of ‘mental health difficulties’/‘mental distress’/‘mental health issues’. While this is the preferred terminology of some organizations working in this area (see, for example, Mind, 2007), in what follows, we tend to adopt the term ‘psychosocial disabilities’ (PSD), utilized, for example, by the World Network of Users and Survivors of Psychiatry. We believe that this terminology offers two important advantages: first, it has the potential both to cover a broader spectrum of conditions, including those best thought of within a social rather than a medical model of the conditions and experiences labelled as ‘mental illness’, and to recognize that internal and external factors in a person’s life situation can affect her need for support or accommodation beyond the ‘ordinary’ (Oliver and Barnes, 2012); second, it brings the conditions and experiences of this constituency of persons firmly within the terrain, and potential protection, of disabilities legislation, which – as we will reflect upon further in the final stages of this article – may be particularly significant in a context in which non-discrimination imperatives impose positive obligations upon public agencies, including those of the criminal justice system, in relation to their equal treatment of complaints. When discussing others’ research, we continue, however, to rely on the terminology of the original study – be this mental health difficulties, mental illness or mental distress – and endeavour where possible to articulate clearly what is included therein. While this is important in terms of not misrepresenting the remit or findings of these previous studies, it should be borne in mind both that not all previous researchers have been explicit regarding the intended meaning and parameters of these terms, and that divergence in terminology or definition across studies inevitably limits the scope for cross-comparison. Finally, it is necessary to note that we use the term psychosocial disability in this article to refer to those who have experience of mental health issues and/or who identify as mental health service users, drawing a distinction between psychosocial disability and intellectual disability. It is, nevertheless, important to acknowledge that these are not mutually exclusive categories – many people with intellectual or cognitive disabilities also identify or are identified as having psychosocial disabilities (Cooper et al., 2007).
The Scale of Victimization: A Known Unknown?
In what follows, we restrict our focus to adult rape complainants – this is by no means to suggest that PSD children do not also experience victimization and attendant challenges in accessing criminal justice against perpetrators, and nor is to deny the complex ways in which experiences of childhood abuse can create additional vulnerabilities as well as more acute reactions to repeat abuse in adulthood. Given the specific procedural and contextual issues that arise in relation to minors, however, we believe this is an issue that merits its own, dedicated analysis.
While there are no routine reporting or recording processes designed to identify the number of crime victims and witnesses who suffer from psychosocial disability in England and Wales, there is growing international evidence that adults with PSD are disproportionately at risk of victimization when compared to the general population (Hiroeh et al., 2001; McCracken et al., 2009; Maniglio, 2009; Sin et al., 2009; Teplin et al., 2005). Many of the studies that have been conducted to date have focused on violent crime, suggesting that persons with severe mental illnesses are particularly vulnerable (Brekke et al., 2001; Hiday et al., 1999; Walsh et al., 2003), with men being more often victims of physical assault while women are at heightened risk of sexual assault and rape (Khalifeh and Dean, 2010; Khalifeh et al., 2013). Mind’s (2007) survey of over 300 people living with ‘mental distress’ in England and Wales found, for example, that 10 per cent had been sexually assaulted, often by someone known personally to them. Following on from this, in a more recent London-based survey of 361 people with ‘severe mental illness’ (a term used here to refer to people with any mental health diagnosis who had been under the care of community mental health teams for one year or longer), a Victim Support/Mind study revealed high levels of victimization, with 45 per cent of respondents having been victims of a crime in the previous year (compared to 16 per cent of London residents in general) (Pettitt et al., 2013). Looking specifically at women, some 42 per cent reported being the victim of rape or attempted rape since the age of 16 and approximately 10 per cent reported being the victim of sexual assault in the past year. In a number of cases, the abuse was determined to be ongoing (see, further, Kelly and McKenna, 1997; Pedlar et al., 2000; Read and Baker, 1996), and there was evidence of a high risk of repeat victimization among persons with PSD, with 43 per cent having experienced more than one type of crime in the past year.
Research from other jurisdictions has reported similarly high rates of alleged sexual victimization among adults with PSD. In the USA, for example, Goodman et al.’s (2001) survey of 782 men and women with ‘serious mental illness’ across four US states discovered that 20.3 per cent of women and 7.6 per cent of men had been the victim of sexual assault in the last year (for other recent US studies, see Coverdale and Turbott, 2000; Eckert et al., 2002; McFarlane et al., 2006; Sells et al., 2003; White et al., 2006). Similarly, a study in France, discovered that 22 per cent of the 64 women with schizophrenia who were interviewed, and 15 per cent of the 26 women with bipolar disorder, claimed to have been raped as adults, with more than half of the former having been raped multiple times (Darvez-Bornoz et al., 1995; see also Chapple et al., 2004).
Of course, it is not simply the mere fact of a diagnosis of mental illness that generates this heightened risk – a range of related contextual factors in the lives of individuals with PSD can increase their vulnerability to abuse, ranging, for example, from low income, a lack of secure housing (Goodman et al., 1995), a history of childhood abuse and a history/current problem with substance misuse. Indeed, as Crossmaker (1991: 204) observes, for many people, living with the label ‘mental illness’ means ‘economic deprivation; little credibility; powerlessness … others making decisions in their “best interest”; lack of access to resources and information more readily available to the general public’, all of which are factors that can potentially increase the risk of (sexual) victimization. Equally, however, research by Hart et al. (2011), using data from the National Child Development Study in the UK found that ‘mental disorder’ among a cohort of participants at age 46 was significantly associated with criminal and violent victimization, even after adjusting for potentially confounding mediators, such as socio-economic status, family income, financial strain, education, housing ownership, heavy drinking and gender. Similarly, in Pettitt et al’s recent study, having taken into account demographics, social deprivation and area characteristics, it remained the case that people with ‘severe mental illness’ were found to be five times more likely to be the victim of an assault than the general population (with women at increased risk being 10 times more likely than general population women).
In part, perhaps, as a result of these pre-existing additional vulnerabilities, there is also evidence which suggests that the impact of victimization on individuals with PSD can be substantial. Indeed, a recent study in England and Wales has identified the impact of domestic and sexual violence as being particularly serious, with 40 per cent of women and a quarter of the men who had experienced these forms of victimization having attempted suicide as a result (Pettitt et al., 2013). Respondents explained how being a victim of crime had impacted on many aspects of their lives, including their financial and material situation, their personal relationships and behaviour, their physical health, housing situation, emotional well-being and mental health. Negative impacts on emotional and mental well-being were particularly marked, with some individuals having to be re-admitted to hospital for treatment for their mental illnesses as a result. For too many complainants, moreover, previous experiences of victimization may be compounded further by subsequent abuse when detained in such mental health wards. In the UK, Mind’s Ward Watch Report, in 2004 found that 18 per cent of inpatients in mental health wards had been sexually harassed and that one in 20 had been sexually assaulted. Meanwhile, the National Patient Safety Agency (2006), in a report which only covered incidents reported to it by health trusts in England and Wales, found disturbingly high rates of sexual harassment and assault, including 19 allegations of rape.
Taken together, then, while there is a paucity of official data on criminal victimization among this constituency, the bespoke research that has been conducted to date in the UK in order to provide a prevalence snapshot paints a stark picture of the potential vulnerability of adults with PSD to sexual assault. The number of such cases that are subsequently reported to the police or to third parties remains a ‘dark figure’, however. Indeed, it is accepted in a wider context that the vast majority of rape victims choose not to report to the police – for a range of reasons, including embarrassment, fear of blame and/or disbelief, distrust of the police, self-blame, shame, fear of reprisals, actual intimidation, fear of the court process and not characterizing an assault as rape (Kelly et al., 2005; Myhill and Allen, 2002). Added to this, recent studies – while not addressing rape victimization specifically – have pointed to the existence of additional and substantial barriers to reporting by victims with PSD. For example, many victims with PSD who responded to Mind’s aforementioned 2007 survey expressed a reluctance to report offences to the police, citing prior negative experiences of reporting and/or detention by the police under ‘place of safety powers’, poor levels of mental health awareness among officers and a consequent lack of confidence that they would be taken seriously and treated with due sensitively and respect. Some victims described an unwelcoming and dismissive police response following disclosure of their diagnosis, while over a third of respondents felt that they had been treated less favourably by the police because of their mental health (Mind, 2007; see also Pettitt et al., 2013). Elsewhere, victims with PSD have expressed fears about being discredited on the basis of their mental health history, the prospect of an intrusive cross-examination based on psychiatric records and the potential detrimental impact that involvement in the criminal process could consequently have on their mental health (Pedlar et al., 2000; Pettitt et al., 2013). In addition, it is clear that some victims elect to remain silent, telling no-one – not even close friends and family or medical professionals – about the offence(s) perpetrated against them for fear that an allegation may be misinterpreted by the police or others as a sign of relapse, possibly leading to hospitalization and/or other serious repercussions such as the loss of access to children; while others fear being blamed for an incident and the negative ramifications that this may hold for the care or services that they receive in the community (Mind, 2007; Pedlar et al., 2000; Pettitt et al., 2013).
Of course, the decision to make an official report to the police is just the first step within the legal system and, as Hanly et al. (2009: 47) point out, one of the only steps – barring a decision to withdraw co-operation down the line – that the complainant takes herself. As the following sections explore, once a rape is reported, the complainant’s role is reduced to that of witness and it is the police and Crown Prosecution Service who take responsibility for the progression – or non-progression – of the case within the criminal justice system. This can generate difficulties for all rape complainants, particularly where they are inadequately supported as vulnerable witnesses, left out of communications in relation to the progression of their case or ‘dropped’ from the system as a result of others’ decision making. For complainants with PSD, however, this process may prove especially challenging, whether because of an apparently increased risk of seeing one’s case fail to progress or a failure to provide/lack of appreciation of the need for additional support and assistance.
The Attrition Problem
Attrition refers to the process by which rape cases ‘drop out’ of the criminal justice system and thus do not result in a conviction. There are various so-called exit points located chronologically at the police investigative, prosecution and trial stages. Once an allegation is made, the first step or hurdle is whether the police record the allegation as a crime, dismiss it or record it as intelligence. If recorded, the police may then refer a case to the Crown Prosecution Service (CPS) or decide to take no further action (NFA) on the basis of insufficient evidence. CPS decisions are, in turn, taken on the basis of the Code for Crown Prosecutors which contains a two-level test: an evidential sufficiency test by which prosecutors must be satisfied that there is a realistic prospect of conviction and a public interest test which requires prosecutors to consider whether a prosecution is needed on this ground, if necessary, balancing factors such as seriousness of the offence, the circumstances of and the harm caused to the alleged victim, the age of the suspect and his or her level of culpability. Finally, if a case reaches court, jurors are tasked with deciding whether the prosecution has discharged its burden and proved beyond reasonable doubt the substantive elements of the offence which under English and Welsh law centre on the absence of consent to sexual intercourse and the absence of reasonable belief in consent (Sexual Offences Act, 2003).
While all crimes have some attrition, sustained high levels of attrition in rape cases have been a source of concern and a focus of policy consideration and much research over the last three decades (Grace et al., 1992; Harris and Grace, 1999; HMCPSI/HMIC, 2002, 2007; Kelly et al., 2005; Lea et al., 2003; Stern, 2010). In this section, we explore what this body of research reveals – and just as importantly fails to reveal – about attrition patterns and pathways in cases involving complainants with PSD. Before doing so, however, it is essential to point out that any analysis of attrition in respect to such cases will necessarily be based on cases identified by the police, or possibly later down the line by prosecutors, as involving a complainant with PSD. As such, one would expect victims with PSD to be underrepresented in relevant studies. While the Code of Practice for Victims of Crime (Home Office, 2013) places an obligation on the police to identify ‘vulnerable or intimidated victims’ – a term defined in section 16 of the Youth Justice and Criminal Evidence Act, 1999 as embracing, among others, victims ‘whose quality of evidence is likely to be diminished because they are suffering from a mental disorder as defined by the Mental Health Act, 1983’ – and to provide them with an enhanced service, research suggests that police have difficulty identifying vulnerable and intimidated witnesses in practice, and that this is particularly true for those with mental disorders (Burton et al., 2007). While critics point to the lack of a consistent approach to training to help officers recognize and work with mental health conditions (McLeod et al., 2010), research suggests that victims may be reluctant to disclose a PSD themselves out of embarrassment or aforementioned concern that it may have an adverse impact on their case by lessening their credibility as a witness. This further compounds the problems of police identification (Mind, 2007; Pettitt et al., 2013), but there is evidence which suggests individual complainants may be more likely to disclose their condition if they are asked about it directly, and particularly if it is explained that the information is needed in order to meet their support needs (McLeod et al., 2010).
Charting attrition in cases involving complainants with PSD
One of the earliest UK-based attrition studies to make reference to rape complainants with PSD investigated 483 rape cases reported in one year and followed their progress through the criminal justice system (Harris and Grace, 1999). With respect to overall attrition, approximately a quarter of cases were no-crimed, a third were NFA-ed and only 6 per cent of cases originally recorded by the police as rape resulted in convictions for rape. The rate of attrition for cases involving complainants with PSD was not specifically examined, however, the authors record that 40 cases discontinued by the police involved complainants ‘who had learning disabilities or were mentally disordered’ (1999: 23). Of these cases, a number were dismissed as false cries for help while others were discontinued out of concern about the possible stress that participation in a trial might have on a complainants’ mental health (1999: 23). Similar reasons for discontinuance were cited in a subsequent study by Lea et al. (2003: 594) who – while not providing figures – reported a ‘very high’ rate of attrition in cases where the alleged rape ‘involved a victim with learning disabilities, psychiatric problems or physical disabilities’. Following on from this, Kelly et al. (2005) observed patterns of attrition in more than 2500 reported rape cases and found that the vast majority (80 per cent) did not proceed beyond the investigative stage. Significantly, the authors of this study highlighted that complaints from women with a disability were almost twice as likely to be designated false compared to reports from non-disabled complainants. Twenty-four cases fell into this former category and in 19 cases complainants were recorded as having ‘mental health problems and/or learning disabilities’ (Kelly et al., 2005: 48). The authors did not address whether the likelihood of conviction was associated with a complainant’s mental health history but did record that convictions were obtained in just 4 per cent of reported cases involving women with ‘disabilities’, whereas 8 per cent of reported cases overall resulted in a conviction (2005: 72).
Two further studies have since given more explicit and detailed attention to cases involving complainants with a background of mental ill-health. Stanko and Williams (2009) provide an analysis of 677 rape allegations recorded by the Metropolitan Police Service Crime Report Information Service (CRIS) during April–May 2005. Of these allegations, one in three was recorded as ‘no-crime’ (of which 30 per cent were designated false allegations), 75 per cent did not proceed beyond the police investigation stage and approximately 6 per cent resulted in a conviction. Drawing attention to the context of allegations, Stanko and Williams report that 87 per cent of complainants had at least one of four so-called ‘vulnerabilities’ – defined in terms of exposure to rape plus disadvantage in relation to what the authors term social believability; namely, they were under 18 years old, under the influence of drugs/alcohol at time of rape, were recorded as having ‘mental health issues’ or were former partners of their assailants. Of these social believability vulnerabilities, mental ill-health, alcohol-related sexual contact and being a young adult reporting peer sexual assault were found by the researchers to have an adverse impact on case outcome. Significantly, victims with mental health issues in this sample were three times less likely to have their allegations classified as a crime of rape and had reduced odds of reaching a conviction (Stanko and Williams, 2009: 215).
More recently, in a relatively small-scale study, Hester (2013) examined attrition in a sample of 87 rape cases reported across three police force areas in the north-east of England. Nearly one in five victims had a mental health problem according to the police record and in the majority of cases these were historical cases with rapes and sexual abuse taking place when the victims were children. Mental health issues were found to be a significant feature in cases that did not result in conviction. Only about a third of cases where the victim had mental health problems resulted in arrest, compared to half of the cases where no such problems were recorded. In accounting for this high drop-out rate, Hester (2013) notes that police officers indicated that some victims with mental health problems were difficult to understand, confused or, in their assessment, delusional. In such instances, the police typically regarded their stories as inconsistent and took the decision not to proceed further with the complaint.
Outside of England and Wales, relevant research is harder to come by but broadly echoes these study findings. For example, in an extensive study of police responses to rape in New Zealand, Jordan (2004) reports high levels of scepticism when confronted with allegations made by victims with a psychiatric illness. Jordan examined 166 cases of which 10 per cent involved complainants with learning disabilities or ‘psychiatric disturbance’. Only three of these cases (13 per cent) were regarded as genuine by the police. Similarly, in an Australian study, researchers found that few allegations of rape made by complainants with PSD resulted in a prosecution and that the single highest predictor of whether a rape complaint was believed by police was whether the complainant had a ‘psychiatric history’ (Heenan and Ross, 1995; see also Lievore, 2004). Meanwhile, in an Irish context, a survey of rape case files received by the Director of Public Prosecutions (DPP) between 2000 and 2004 revealed that approximately 13 per cent involved a complainant with a history of mental illness. Of these 78 cases, only two were prosecuted and both resulted in not guilty verdicts at trial (Hanly et al., 2009: 240).
In summary, then, the picture that emerges from these previous studies is one of heightened attrition rates in cases involving reports from complainants with PSD. It is, however, a picture that contains substantial gaps. Some attrition studies have neglected victims with PSD entirely, while others provide a fairly rudimentary assessment of the passage of complaints by victims with PSD through the criminal justice system. There has, for example, been little attempt to examine the context of these reports, the circumstances within which these alleged rapes occurred, the life circumstances of complainants and any association between such factors and rape attrition. Without such contextualization, it is difficult to know what conclusions to reach. After all, while police and prosecutors are duty-bound to make progression decisions based on the credibility of a complaint, as well as the complainant’s ability to withstand evidence-giving, these assessments may well be complicated by the existence of a history or current PSD diagnosis, even in some cases where it remains undisclosed. Indeed, in a context in which researchers have documented the existence of a substantial overestimation of the scale of false rape reporting among police officers (Kelly et al., 2005: xii; see also McMillan, 2010), it may be hypothesized that (mis)understandings of mental illness will provide an additional justification for scepticism. Certainly, some victims with PSD have a perception of prejudicial attitudes existing within the police service and have voiced concerns about not being believed or taken seriously because of their mental health background (Mind, 2007; Pettitt et al., 2013). Outside of the CJS context, moreover, there is a substantial body of literature which documents the woeful stigma and discrimination faced by people with PSD in a variety of areas of social life (Corrigan, 2005; Crisp, 2004; Hinshaw, 2007; Thornicroft, 2006). This evidences – as acknowledged, for example, in recent debates around public mental health (Royal College of Psychiatrists, 2010) – the existence of poor levels of understanding about mental illness within the general population and common ‘myths’ about the capabilities of those diagnosed with a psychiatric condition.
Given that the police receive limited mental health awareness training (McLeod et al., 2010; Mind, 2007), it would be surprising if these same attitudes were not also present to some extent within the police service and, consequently, exerting some influence over police handling of rape allegations by complainants with PSD. Even if individual officers and prosecutors do not subscribe to such stereotypes, moreover, they may impute this type of thinking to others (i.e. future jurors) and calculate that there is thus no realistic prospect of conviction, notwithstanding the intrinsic evidential merits of a case. Certainly, while researchers have yet to investigate the influence, if any, of specific PSD diagnoses on decisions made in the jury room, findings of rape trial simulations suggest that certain case characteristics, including the complainant’s consumption of intoxicants and evidence of inconsistencies or incomplete recall in her account can damage credibility in the eyes of (mock) jurors (Ellison and Munro, 2009; Finch and Munro, 2006, 2007; see also Munro and Kelly, 2009). In addition, concerns have been raised about the potential misuse of psychiatric evidence in court to discredit complainants unfairly by tapping into common prejudices about mental illness and the link between mental ill-health and witness credibility in ways that may undermine prospects for fair and just outcomes (Ellison, 2009; Mind, 2007; Pettitt et al., 2013).
Further, dedicated research is clearly required, then, in order to disentangle the ways in which assessments of the credibility of complaints and the reliability of victim-witnesses are made in cases involving rape complainants with PSD and, in particular, to explore the extent to which they are premised on prejudice or misunderstanding and might be improved by additional training. Moreover, in a context in which victim withdrawal remains a significant contributor to rape attrition in general, the ways in which improved victim support (tailored as appropriate to the peculiar needs of a complainant) and better engagement between criminal justice system (CJS) personnel and complainants throughout the investigation and trial process might assist in securing greater access to justice in cases involving PSD complainants also merit further exploration (Kelly et al., 2005). In this regard, while subject to a number of limitations, data gathered by the Metropolitan Police Service, discussed in the next section, provide important initial insights into the profile of rape allegations made by victims with PSD and some of the factors that potentially come to influence decision making at the early stages of the criminal process. As such, it provides a useful starting point from which to develop an agenda for a fuller and more contextualized evaluative study of contemporary CJS responses.
The Study
As discussed in the previous section, such research as currently exists in England and Wales indicates that the odds of attrition are higher for cases involving victims with PSD than for non-PSD rape allegations (Harris and Grace, 1999; Hohl and Stanko, in preparation; Kelly et al., 2005; Lea et al., 2003; Stanko and Williams, 2009). However, these studies do not provide any systematic analysis of the role of complainant PSD in the attrition process. The London Metropolitan Police Service (MPS) produced a comprehensive dataset of all allegations of rape received in April and May 2012 (N = 679). The dataset is representative of all complaints of rape made to the Metropolitan Police. This is confirmed by official records for the same year published by HMIC. Key sample characteristics such as the overall number of rape complaints and number of ‘no-crimed’ cases in the two months sampled for this study are in line with the annual MPS figures as reported by HMIC (2014). The HMIC (2014) report further indicates that the MPS data might provide a good representation of the nation-wide picture. Compared to other police forces in England and Wales the MPS has average levels of no-criming and sanction detections. ‘No-criming’ refers to the practice of re-classifying a case initially reported and recorded as a crime as ‘no crime’. According to the Home Office Counting Rules, a case should be no-crimed if there is verifiable information that no crime was committed or for administrative reasons (e.g. duplicate record or if the case falls outside the jurisdiction), however, there is evidence that, in practice, police forces have also no-crimed cases on the basis of perceived insufficient evidence, the suspicion that the complaint might be a false allegation or when the complainant withdrew from the process (HMCPSI/HMIC, 2007; Stern, 2010).
Under the guidance of Professor Elisabeth A. Stanko researchers at the MPS Strategy and Research Unit read, analysed and coded the full police records of each rape complaint in the sample. The resulting dataset includes complainant mental health as an analytical category, thus giving us a valuable opportunity to carry out statistical analyses focusing specifically on how complainant PSD may relate to other case characteristics and affect the case outcome. The authors have been granted permission to re-analyse the dataset via an Information Sharing Agreement under the MPS Freedom of Information Act Publication Scheme.
The key variable of interest for the present study is the police records noting ‘victim has mental health issue’, coded as 0 = no and 1 = yes. The variable is an indicator of either the complainant having disclosed to the police what the police consider to be a PSD, the police obtaining evidence of a victim PSD or the police recording the impression that the complainant has a mental health issue. Thus, the variable may be both under-inclusive in that not all complainants with a PSD will disclose or display symptoms to the police and over-inclusive in that it may include complainants without a PSD whom the police nonetheless perceive to have a ‘mental health problem’. These discrepancies need to be kept in mind when interpreting the findings and, to the extent that having a PSD may not impact on the attrition process in the same way as being recorded as having a PSD, the analysis requires an additional measure of caution. Since the data collection did not focus specifically on PSD, the dataset made available to the authors does not provide detail on the nature and severity of the PSD, and does not specify whether the PSD is past or ongoing. Our findings thus aggregate over these potentially relevant differences within the broad range of PSD contexts, but allow broader-brush conclusions.
In analysing the dataset, the authors have used significance tests to identify differences between cases involving complainants with and without recorded PSD. All analyses exclude cases involving a male complainant (42 cases) and 50 cases in which the sex of the complainant is not recorded.
Case outcomes
Table 1 shows case outcomes for complainants with and without recorded PSD. The results indicate that complainants with recorded PSD are significantly more likely to have their case no-crimed than complainants without recorded PSD (11 per cent and 5 per cent, respectively) and significantly more likely to have their case dropped through a police NFA decision (45 per cent vs 38 per cent). Key intermediate milestones in the police investigation such as suspect identification, arrest and charge are also significantly less likely to be reached in cases noting a complainant PSD. Cases of complainants with recorded PSD are then significantly less likely to have their case referred to the CPS for a decision (13 per cent vs 21 per cent) and the CPS is, in turn, significantly less likely to charge in cases involving complainants with PSD (4 per cent vs 10 per cent). In short, therefore, the picture that emerges from these data appear to be consistent with that depicted in pre-existing literature; suggesting that rape allegations involving complainants with recorded PSD are significantly and substantially more likely to suffer from attrition.
Comparison of case outcomes and milestones between victims with and without PSD.
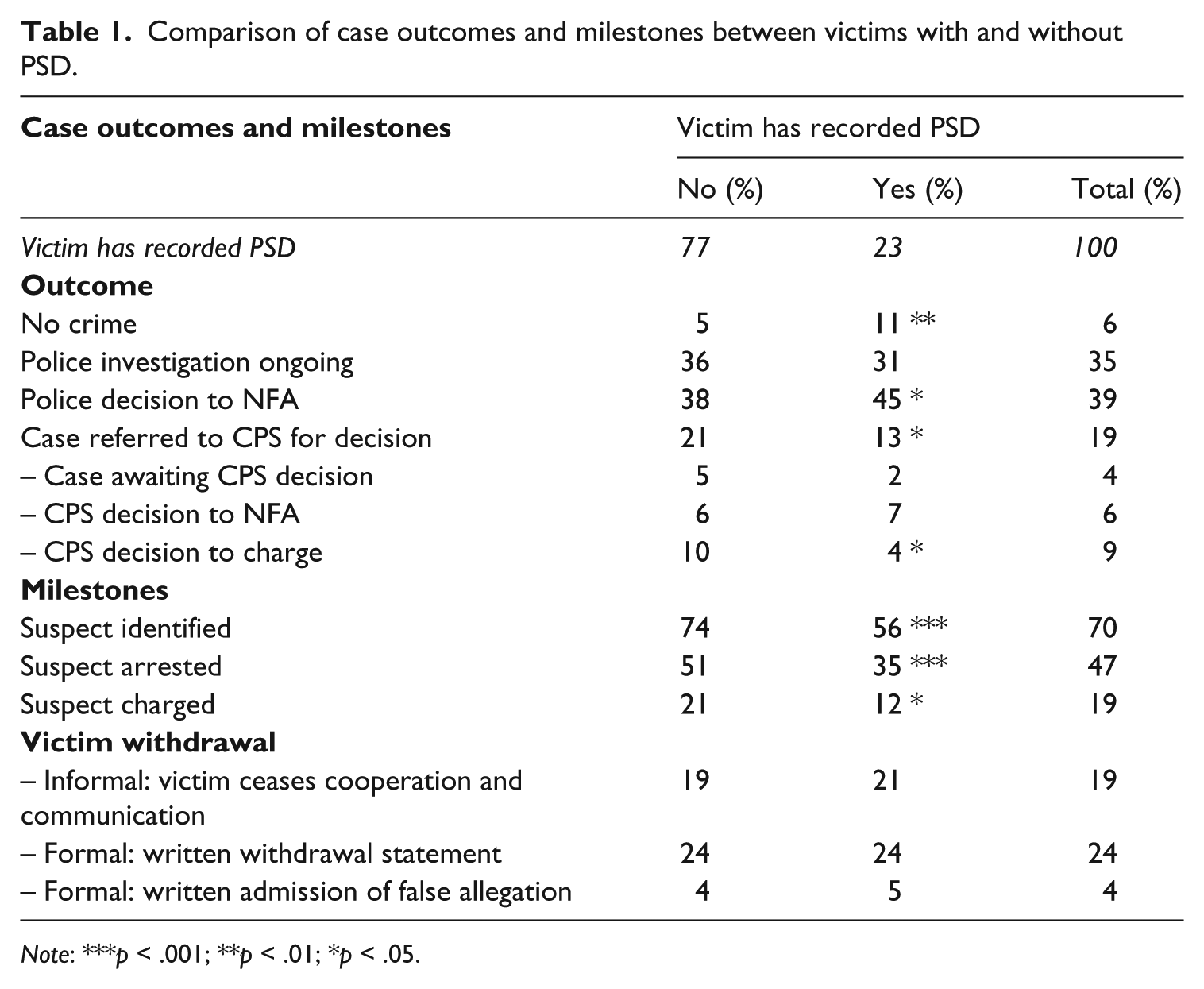
Note: ***p < .001; **p < .01; *p < .05.
Importantly, and in contrast to the findings of Hanly et al.’s (2009) research in Ireland, which found a ‘disproportionately high rate of withdrawal’ (2009: 241) among complainants with a history of mental illness, the significantly higher rate of attrition at all stages in the MPS data was not attributable to complainants with recorded PSD withdrawing from the process any more frequently than other complainants. It follows, therefore, that the higher attrition must be due to a police or CPS decision to drop the case, a finding that – as discussed above – underlines the importance of conducting further research in order to explore in more detail the contexts within, and justifications upon, which such progression decisions are taken.
Case characteristics
Table 2 provides a comparison of complainants with and without recorded PSD along incident, reporting, police investigation and complainant characteristics. Statistically significant differences are displayed in the table and pertinent non-significant results summarized in the text.
Comparison between victims with and without PSD.
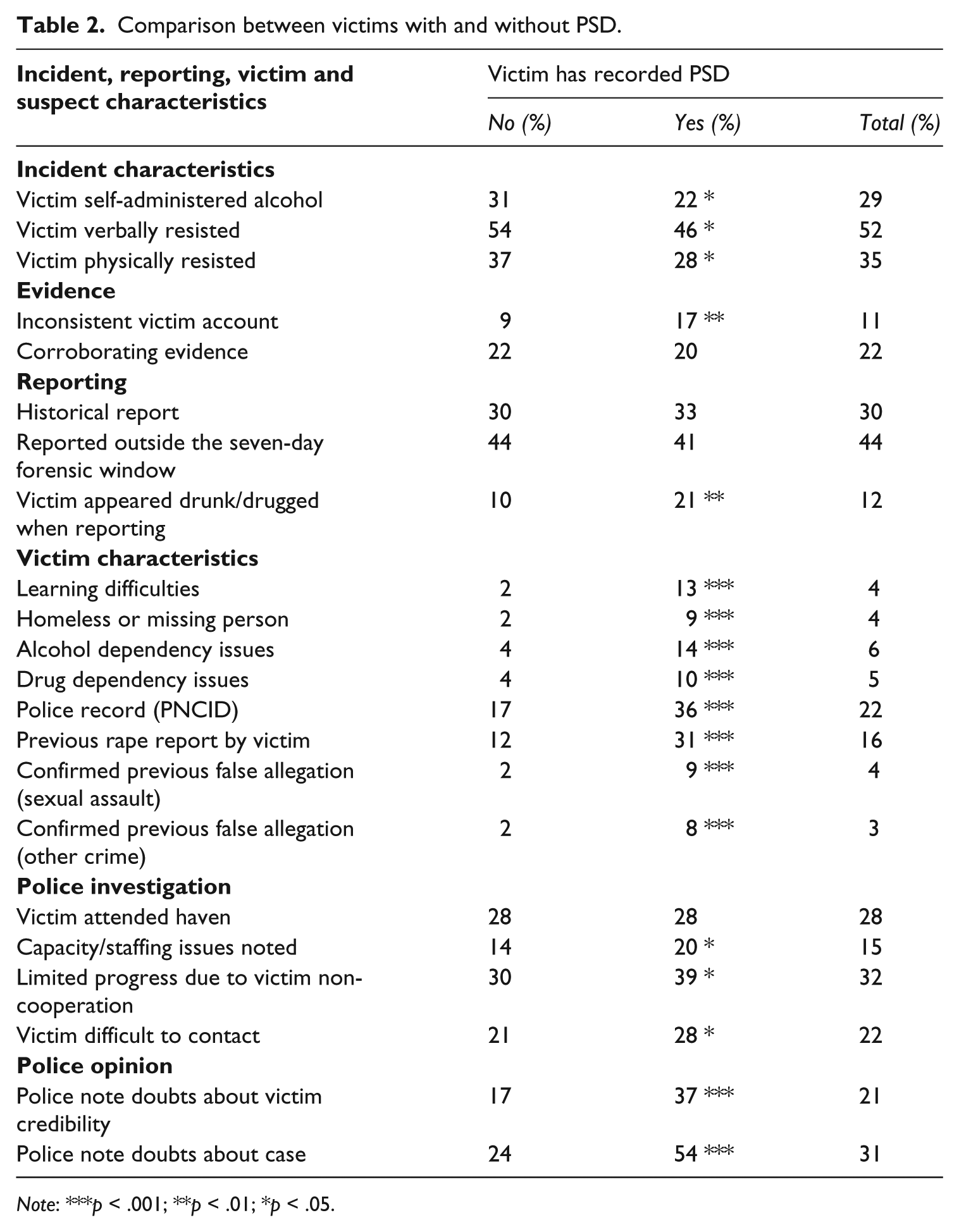
Note: ***p < .001; **p < .01; *p < .05.
Cases involving complainants with recorded PSD were more likely to display a range of characteristics that the research literature suggests may contradict common notions of ‘real rape’ and lessen the credibility of the complainants: more specifically, complainants with recoded PSD were significantly less likely than complainants without recorded PSD to resist the attack physically (28 per cent and 37 per cent, respectively) or verbally (46 per cent vs 54 per cent), they were significantly more likely to provide an inconsistent account of the incident when recounting it to the police (17 per cent vs 9 per cent) and significantly more likely to appear under the influence of drugs or drink when reporting the allegation to the police (21 per cent vs 10 per cent), even though they are in fact less likely to have been drinking when attacked (22 per cent vs 31 per cent).
Complainants with recorded PSD in the present study were also significantly more likely than complainants without recorded PSD to display a range of other characteristics which the literature suggests heightens victim vulnerability and damages complainant credibility. Complainants with recorded PSD were, for example, significantly more likely than complainants without recorded PSD to have learning difficulties (13 per cent vs 2 per cent), be homeless or reported as missing persons (9 per cent vs 2 per cent), have an alcohol or drug dependency (14 per cent vs 4 per cent and 10 per cent vs 4 per cent, respectively) and to have previously reported a rape to the police (31 per cent and 12 per cent). Furthermore, complainants with recorded PSD were more likely to arouse police scepticism because they were twice as likely to be known to police (36 per cent and 17 per cent) and four times more likely to be recorded as having made a previous false allegation, either of sexual assault or some other crime (9 per cent and 8 per cent respectively, vs 2 per cent).
The notion that PSD, and the associated vulnerabilities, may damage complainant credibility is seemingly confirmed, moreover, by the finding that police officers in the present study explicitly recorded general doubts about the case in over half of those involving a complainant with recorded PSD (54 per cent) but in only 24 per cent of cases involving a complainant without recorded PSD. Furthermore, the police explicitly noted doubts about the credibility of the victim in particular in 37 per cent of cases involving a complainant with a recorded PSD compared to only 17 per cent of cases in which the complainant had no recorded PSD. Data from the present study also suggest that the police investigation itself may be more likely to be hampered by problems if the case involves a complainant with a recorded PSD. Indeed, in such cases, police officers were significantly more likely to note slow progress in the investigation due to capacity/staffing issues (20 per cent vs 14 per cent), difficulties in contacting the victim (28 per cent vs 21 per cent) and poor cooperation on the part of the victim (39 per cent vs 30 per cent).
On the other hand, our results suggest that complainants with recorded PSD are no different from those without recorded PSD when it comes to a range of other factors which previous research has identified to be relevant for a successful investigation and prosecution of a rape complaint. In particular, complainants with recorded PSD were no more likely to report outside the seven-day window for forensic evidence, no more likely to delay reporting an experience of rape for long periods, as in the case of historic rapes, just as likely to attend a Rape Crisis ‘haven’ to receive support and no less likely to have sustained visible injuries during the rape. In addition, the data indicate that there were no significant differences between these types of complaints in terms of the availability of independent, corroborating evidence (e.g. witnesses, CCTV footage, mobile phone records).
In summary, then, and bearing in mind the possibility of under-recording of PSD by the police, our analysis of this snapshot of Metropolitan Police rape reporting suggests that complainants with recorded PSD are significantly more likely than those without recorded PSD to experience additional, circumstantial vulnerabilities, that their credibility is explicitly doubted by police officers in the majority of cases and that police officers are significantly more likely to judge such complainants to be uncooperative and difficult to contact. In this context, it is perhaps unsurprising that complainants with a recorded PSD in the present study were nearly three times (2.92) more likely to have their case no-crimed than victims without recorded PSD. Multivariate logistic regression analysis reveals that this cannot be explained by the range of other differences in incident and complainants characteristics between complainants with and without recorded PSD, including the likelihood to provide an inconsistent victim account or to have made previous false allegations (the effect on the odds only reduces to just under 2.5). This suggests that there is a need for greater critical scrutiny in relation to the factors that provoke and justify these non-progression decisions. To the extent that this may suggest that police and prosecutors are being inappropriately influenced by stereotypes and prejudices about mental illness, and misconceptions regarding the impact of PSD on victim perception, credibility and reliability, or being pushed towards dropping cases out of a concern about complainant welfare that could be obviated by better provision of victim support, this is clearly a significant concern in terms of access to justice and non-discrimination. Though the MPS data discussed here provide glimpses that allow us to begin to interrogate the current handling of these complainants and their allegations, it is clear that far more research is needed in order to begin to evaluate critically, understand and if necessary improve responses.
Future Directions
Understanding attrition in rape cases involving complainants with PSD is no straightforward task, not least because PSD covers such a diverse range of mental health conditions – from anxiety and depression to psychotic conditions like schizophrenia. Each rape case is thus likely to present its own unique challenges not only in terms of issues relating to a complainant’s PSD and other associated needs but also – as indicated in previous sections – in terms of the other contextual factors associated to the complaint and the complainant. Nonetheless, in a context in which existing research points consistently to a disturbingly high dropout rate for this category of rape allegations, we submit that there are potentially valuable insights to be gained from further targeted study that – in contrast to previous studies – sets out to disaggregate types of PSD, to look closely at the wider context of allegations, and to engage police and prosecutors in qualitative discussions about the challenges these cases pose for individual officers/prosecutors, their institutions and the wider criminal justice system. Such discussions could specifically help to elucidate, among other things: (1) the extent to which criminal justice personnel regard themselves as equipped to identify complainants with PSD and then to deal with cases appropriately in a context of reputedly limited mental health awareness training; (2) the ways in which PSD (and associated vulnerabilities, e.g. drug dependency, learning difficulties, repeat victimization) are seen to be damaging to the reliability or credibility of rape allegations and the consequent impact on decision making; (3) the information sources that criminal justice personnel rely upon in making credibility/reliability assessments (e.g. medical records, family members, other professionals); (4) how far decisions to proceed or discontinue are influenced by trial-related concerns (e.g. defence use of psychiatric records, ability of a complainant to withstand the stress of testifying, the influence of PSD diagnoses on juror decision making); (5) the perceived sufficiency of support /protection afforded to PSD rape complainants at different stages of the criminal process.
Without this contextualized information and data there can be no meaningful evaluation of the current criminal justice response to sexual victimization involving adults with a PSD. As a consequence, it is impossible to say whether this population of complainants are receiving fair, just and appropriate treatment at the hands of criminal justice agencies or whether – as critics fear – a combined lack of support, poor levels of understanding of mental illness and/or attitudinal barriers are, at present, operating to deny complainants with a PSD an equal chance to secure justice. While this may be considered problematic in itself – given that the fair treatment of all victims is fundamental to the proper administration of justice – the need for a more robust evidence base is, we would argue, further compounded, in this context, by statutory obligations imposed on all public authorities, including the police, CPS and the courts, to promote actively equality of opportunity for those with disabilities and to eliminate unlawful discrimination (Equality Act, 2010). People with long-term mental health conditions come under the protection of this legislative framework, and criminal justice agencies are accordingly required to have an understanding of the impact of their activities on this constituency, and in particular the potential barriers to equality of opportunity and access that may arise in their day to day handling of such cases. Similar evidence gathering and monitoring obligations also flow, we suggest, from international obligations to ensure ‘effective access to justice’ for persons with disabilities on an equal basis with others contained in the United Nations Convention on the Rights of Persons with Disabilities (Article 13) adopted in 2006. The Convention adopts a definition of disability which includes persons with ‘long term mental impairments’ – a formulation which embraces people with PSD (Article 1). Moreover, it specifically requires governments to ‘collect appropriate information, including statistical and research data, to enable them to formulate and implement policies’ to give effect to convention rights (Article 31).
As a final reflection, it is important to acknowledge that the victimization of people with PSD poses significant challenges not only for the criminal justice system but for other services including health, social care and voluntary sector organizations with which criminal justice agencies must necessarily work in partnership. While the concept of partnership working in rape cases is now well established (HMCPSI/HMIC, 2007), the extent to which these different agencies are able to surmount the challenges associated with joint working and co-ordinate at a strategic and operational level is something about which we know very little at present and is thus, we suggest, another key area on which future research could usefully shine a light. In its mental health strategy for England and Wales, No Health without Mental Health (Department of Health, 2011), the government has made an explicit commitment to providing parity of esteem to mental health services and ensuring that those suffering with mental health problems receive a high quality of service from all government agencies. Furthermore, the policy acknowledges that women suffering with mental health problems are more likely to be victims of sexual violence. This makes the victimization of women with psychosocial disability not only a criminal justice concern but also an important public health issue as emphasized by the Royal College of Psychiatrists (2010) in its own policy statement No Health without Public Mental Health. Further detailed research looking not only at the legal progression of such cases but also the impact on victims and mental health support offered would provide invaluable and much needed information to inform future models of interagency working. It is as yet unknown to what extent victims with psychosocial disabilities receive appropriate care and support throughout the criminal justice process, any variations in the levels of support offered and the impact of the process on such victims. Research would allow the current provision of support to be ascertained and allow possible recommendations to ensure such victims receive appropriate support and care from all agencies working in concert so that they are not re-traumatized or re-victimized by the very agencies trying to extend help.
Footnotes
Acknowledgements
The authors would like to thank Professor Betsy Stanko and Corporate Development Strategy and Research Unit at the Metropolitan Police Service for their kind assistance in facilitating data access.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.