
Abstract
At-Risk Units (ARUs) are dedicated facilities established in New Zealand prisons to assist those considered to be ‘at risk’ of self-harm or suicide. Their remit is ostensibly care-based and rights-conscious, with authorities noting that ARUs preserve the ‘right to life’. Drawing upon research within two correctional sites, alongside analysis of recent documents from oversight bodies and courts, this article considers ARU operations. It is argued that, all too often, ARUs have undermined humane practices towards suicidal or ‘at-risk’ prisoners. Four problems are apparent: (1) ARUs are misused and overused in such a way that secure punishment, rather than care, is prioritized; (2) within a context of ‘lesser eligibility’, ARUs operationalize degrading conditions and treatments towards prisoners; (3) humane treatments are further diminished by a correctional approach to prioritize legal or bureaucratic compliance; and (4) authorities avoid institutional sanction for prisoner harms or deaths, particularly through an emphasis on personal responsibilization or blame. The end-result is that ARUs are regularly operationalized in ways that exacerbate risks and diminish rights for prisoners. A question remains about their fundamental use as an appropriate response to those who suffer mental health distress within penal environments.
Introduction
At-Risk Units (ARUs) are dedicated, purpose-built facilities established in New Zealand prisons to provide safe spaces for individuals considered to be ‘at risk’ of self-harm or suicide. In many jurisdictions, prisons have introduced ARUs, or similar ‘safe-cell’ regimes, as a way to uphold human rights obligations, including preserving a prisoner’s ‘right to life’. Their remit is ostensibly care-based and rights-conscious, with authorities noting that many prisoners have been stopped from self-harming and suicide, whether attempted or actual, as a result of interventions (Burrows et al., 2003; Corcos and Lewin, 2001; WHO, 2007). However, in practice, these units often operate almost identically to punitive or behaviour management regimes and can result in vulnerable prisoners being subject to periods of solitary confinement, sometimes for lengthy periods of time (Shalev, 2017).
This article considers the establishment and operations of ARUs, with a particular focus on New Zealand. Drawing upon recent research across two correctional sites, we argue that ARUs, while wrapped in a language of rights, have served to diminish and undermine humane practices towards suicidal or ‘at-risk’ prisoners. The article examines four principal problems. First, penal institutions misuse ‘at-risk’ cells and prisoners subsequently experience ARUs as a form of harmful punishment. Second, social discourses of ‘lesser eligibility’ and offender dangerousness contribute to degrading conditions and treatments within ARUs. Third, correctional bureaucracies have prioritized compliance with legally driven rights, in a way that undermines the humane or care-oriented treatment of prisoners. And, fourth, authorities place the ultimate responsibility for self-harm and suicide onto individual prisoners, thus avoiding institutional blame for the conditions and practices inherent in the correctional environment that contribute to prisoner harms or deaths in the first place. In short, the practice of responding to those ‘at risk’ in New Zealand prisons has often served to enhance rather than reduce risky treatment and conditions.
In many ways, these harmful realities for ARU prisoners are consistent with the broader heightened emphases on risk management in modern penal environments (Feeley and Simon, 1992). Anglophone punishment systems have seen a shift to more punitive and risk-averse approaches, and risk has become ‘a much more expansive category’ (Pratt and Anderson, 2016: 529–530, emphasis in original). The remit of controlling ‘disordered’ or ‘dangerous’ individuals has heralded a range of ‘public protection’ measures including expansive surveillance measures, indefinite imprisonment, civil detentions, the increased use of remand, tightening of parole and restrictions on movements (Pratt and Anderson, 2016). Politicians and government agencies insist that any displacement of human rights is entirely reasonable, and indeed necessary, given the amorphous nature of offender risks that must be contained. In turn, alongside a shift to managerialism (invoking financial efficiencies and performance indicators), prisons are dominated by security concerns (Drake, 2012).
Against this background, ARUs are prison sites in which the notion of risk is particularly fluid. Prisoners can be ‘at risk’ of suicide or from the harms posed by the mainstream prison, however they are also cast as being particularly ‘risky’, creating risks to themselves and to the institution. Thus, ARUs prioritize risk prevention over other logics such as prisoner rehabilitation, care or human rights. Units control ‘disorderly’ ARU prisoners by restricting movement, removing access to others, preventing activities, denying privacy, using restraints for prolonged periods and consolidating surveillance, among other practices. The end-result is a ‘risky’ environment for prisoners. Yet, for prison authorities, these risks and the human rights violations that underpin them are legitimate responses to the maintenance of secure order and prison performance.
Data collection
The primary research for this article took place within ARUs in two male prisons in New Zealand (Harris, 2015). Its principal elements involved: (1) 19 semi-structured interviews with correctional, nursing, psychology and psychiatry staff working in the ARUs; and (2) a case file analysis of 187 prisoners held in the ARUs during a three-month period in 2014, with data gathered from the Department of Correction’s Integrated Offender Management System. The primary research was carefully established to align with the Department’s research priorities and, after some negotiation on access (a process that took almost six months), the Department gave approval. In retrieving data, the project received valuable assistance from a Correctional Health Centre Manager. On completion, and according to usual contract, the Department’s ‘Research and Evaluation Governance Committee’ reviewed the research. They requested the redaction of certain data before any publication. This article subsequently cites the research (Harris, 2015), where appropriate, rather than directly quoting from primary data. To supplement the interview and case file research, the authors analysed other documentary sources, such as statistics relating to suicide and self-harm, official policies relating to ‘at-risk’ procedures and reports from official bodies such as the Coroner’s Court, the Ombudsman’s Office and the Human Rights Commission.
Prisoners’ Rights and the Development of At-Risk Units
At-Risk Units have emerged in line with the global development of human rights, which emphasizes the fair treatment, dignity and protection of prisoners and other detained persons (Cliquennois and Champetier, 2012). Over the last half-century, the United Nations (UN) has developed a network of laws, rules and principles to which signatory states must adhere, combined with monitoring and oversight mechanisms to provide increased scrutiny of practices behind closed walls. 1 These international levers and conventions have been ratified by various governments through the introduction of domestic legislation, which are also supported by a state’s ‘duty of care’ obligations for those held in the custody of the state (IPCA, 2015).
In relation to health, the UN requires states to provide equitable services to prisoners, and to ensure that prison conditions and treatments do not impact negatively on prisoners’ health and well-being. The International Covenant on Economic, Social and Cultural Rights confirms that everyone should enjoy the ‘highest attainable standard of physical and mental health’ (UN, 1966: art. 12). The Basic Principles for the Treatment of Prisoners determines that ‘[p]risoners shall have access to the health services available in the country without discrimination’ (UN, 1990: Principle 9). And, the UN’s recently revised Standard Minimum Rules (the ‘Nelson Mandela Rules’) establish clear guidelines for the medical treatment of prisoners. Among other instructions, physicians (or their equivalent) must see prisoners regularly, and identify and treat any health care needs, including those mental health needs that are ‘brought on by the fact of imprisonment’ (UN, 2015: Rule 30(c)). 2
Similarly, the World Health Organization (WHO) works to establish situations where ‘all prison health services […] reach standards equivalent to those in the wider community’ (WHO, n.d.). This global organization has outlined that prisoners struggling with suicidal or self-harm ideation must be placed within ‘suicide-safe environments’. These harm-preventive spaces should have minimized hanging points 3 and will restrict prisoners from accessing other ‘lethal materials’ (WHO, 2007: 16). Prison authorities are encouraged to provide conditions that ensure prisoners (and staff) are well, in body and mind.
Alongside health-based rights obligations, the Nelson Mandela Rules also explicitly prohibit the placement of prisoners with physical or mental disabilities in solitary confinement (see Rule 45(2)). As outlined by Shalev (2017), despite ARUs providing a ‘suicide-proof’ environment for prisoners, it could be argued that – by their very nature – they operate in breach of international standards. This is particularly worth considering in light of the fact that suicide and self-harm, which are over-represented in prison, are higher still in the context of solitary confinement (Kaba et al., 2014). Similarly, it is widely understood that individuals with existing mental health issues are likely to have any conditions worsened as a result of isolation (Reid, 2000).
Despite these considerations, in many Anglophone states, an endorsement of ‘rights-based’ approaches has been translated into the introduction of ARUs, or similar regimes. For example, Australian states, such as Victoria and New South Wales, have adopted practices to manage ‘at-risk’ prisoners through the use of ‘Safe Cells’ or ‘Safe Observation’ cells which minimize ligature points and furniture (Corrections Victoria, n.d.; Corrective Services NSW, n.d.). Similarly, ‘safer cells’ were introduced in prisons across England and Wales in 2000, in efforts to prevent suicide and self-harm (Strickland and Grimwood, 2016). While the Ministry of Justice there notes that safer cells can reduce self-harm and suicide via minimized ligature points, officials note that they are not effective in dealing with underlying mental health or behavioural issues (Ministry of Justice, 2012). In a bid to prevent suicides, many authorities have also adopted other restrictions, such as the use of anti-suicide gowns or the curtailment of prisoner access to razor blades (Burrows et al., 2003; Corrections Victoria, n.d.; Department of Corrections, 2013).
New Zealand has incorporated the above approaches, to minimize harms through changes in architecture, clothing and resource provision. Yet, as detailed further below, the Department of Corrections also relies upon technologies – such as ‘tie down beds’ – that are prohibited elsewhere, including in England and Wales. There is a growing consensus that such restraints lead to prisoner violation, particularly given that prisons are generally not well equipped to deal with challenging mental health or suicidal behaviours (Shalev, 2017). Other jurisdictions have begun to explore alternative responses to ‘at-risk’ individuals, including the diversion of those with mental health issues towards a more rights-based treatment and recovery pathway. For instance, in the USA, there are now over 300 adult mental health courts, established to divert mentally unwell individuals away from the prison system and into community treatment plans, with recent indications being that this treatment can substantially reduce recidivism rates (Costopoulos and Wellman, 2017).
At-Risk Units in New Zealand
There are 14 ARUs in New Zealand, present in all but four of the country’s 18 public prisons (Office of the Ombudsman, 2017). Units are made up of a number of segregated cells, where prisoners are transferred once they are assessed as being ‘at risk’. Prisoners may be assessed as being ‘at risk’ on arrival by officers, or after self-reporting thoughts of self-harm or suicide. Once in the prison system, a prisoner may also be categorized as ‘at risk’. Again, this can result from self-identification or if an officer is concerned about a prisoner’s behaviour or changed mood. The Prison Operations Manual (POM) describes the purpose of an at-risk assessment is to identify the level of self-harm risk that each prisoner presents and to minimize any risks to that individual as quickly and as safely as possible (Office of the Ombudsman, 2017).
Officially, prisoners are moved to ARUs to ensure that they are managed safely through accurate recording of information, frequent observation and careful consideration of transfer (Department of Corrections, n.d.). Prisoners deemed to be ‘at risk’ must have a separate ‘at-risk’ file established and a tailored management plan in place, which outlines any ongoing assessment, treatment or monitoring deemed necessary. This may include ongoing secondary mental health care, continuous observations or specific management interventions that will assist the prisoner to remain in, or return to, mainstream residential units (Department of Corrections, n.d.).
Notwithstanding the benefits that ARUs are depicted to have within correctional policy and literature, it is increasingly clear that they are operationalized in ways that diminish care and erode human rights for prisoners. Department of Corrections officials have noted that ARUs are not equipped to treat or address underlying causes of self-harming or suicidal behaviour and recognize that people exhibiting similar behaviours, including those with significant mental health needs, would generally be managed differently in the community (Frame-Reid and Thurston, 2016). This departmental stance is supported by a recently announced review of ‘at-risk’ prisoners, titled ‘Transforming the management of at-risk prisoners’, as well as the announcement of a new strategic plan to provide a greater level of mental health, alcohol and drug support to prisoners (Shalev, 2017). Despite these positive developments, issues of institutional cultures and pressures, lesser eligibility, a focus on compliance combined with a corresponding tolerance for impunity are currently coalescing to make ARUs ‘risky’ environments in themselves. While discussed separately below, these elements intersect to produce harmful conditions and treatments for those held in New Zealand’s penal institutions.
The Misuse of At-Risk Units
In New Zealand, official policy states that ARUs should only be used to ‘manage and observe’ prisoners with self-harming or suicidal ideation (Department of Corrections, n.d.). Yet, in reality, ARUs manage a much wider range of prisoners. Staff often make discretionary decisions about placement to achieve other institutional priorities, and this results in a steady throughput of prisoners. Between 2014 and 2017, over 7000 prisoners spent time in these Units (Beales, 2017). Given the significant over-representation of Māori in New Zealand’s prisons, it seems reasonable to determine that Māori account for a majority of those held in ARUs. 4
More recently, case file analysis of two New Zealand prisons found that 187 male prisoners (ethnicity unidentified) had progressed through ARUs over the three-month period of 1 June to 31 August 2014 (Harris, 2015). Staff decisions for holding 19 of the prisoners within ARUs went unrecorded or were unclear. However, the remaining 168 prisoners had varied backgrounds (see Table 1), and just over a quarter had experienced self-harming or suicidal behaviours.
ARU placement decisions in two New Zealand prisons.
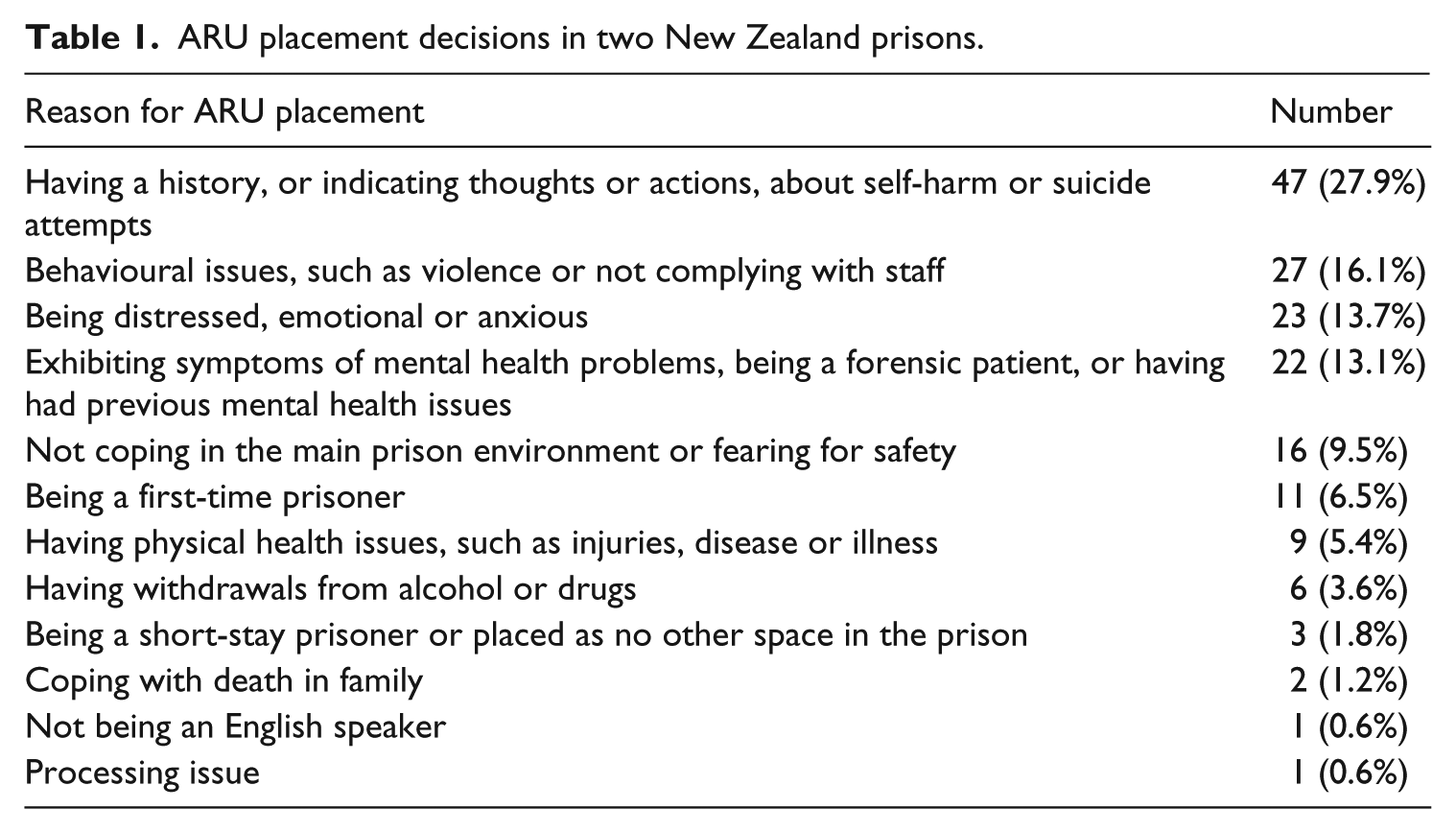
The two prisons used ARUs to manage a host of prisoner circumstances and difficulties that went far beyond their remit. For instance, ARUs were regularly used for ‘behaviour management’ purposes, for prisoners who had been violent or non-compliant in other Units. In 2012, the New Zealand Ombudsman similarly noted that it is particularly common for volatile prisoners who show signs of ‘highly disruptive and disturbed behaviour’ to be physically contained and managed in ARUs (Wakem and McGee, 2012; also see National Health Committee, 2010). As one ARU nurse put it: ‘[t]his is a dumping ground for when you can’t find a place for somebody’ (Harris, 2015: 50).
Prisoners who felt distressed, anxious or were not coping in the mainstream prison also accounted for well over a quarter of those held. These individuals, that included new arrivals to the prison, could express fears relating to their personal safety after, for example, being stood over for medication or food in the mainstream. These rational bursts of emotion meant that prisoners were informally diagnosed as ‘at risk’. The individual, rather than the dangerous nature of prisons, was identified as the concern (see National Health Committee, 2010).
A steady stream of prisoners presented with mental health difficulties, with one ARU nurse commenting how the ARU acted as ‘the prison mental health unit holding unit […] because we don’t have anywhere else. We don’t have anywhere else that is safe, that is monitored […] so [the ARU is] our default position’ (Harris, 2015: 52). This included those with personality disorders, or those experiencing manic episodes or hallucinations. Some had acute mental health problems.
The UN’s Nelson Mandela Rules stipulate that those diagnosed with severe mental disabilities should not be detained in prisons at all (UN, 2015: Rule 109). Official New Zealand guidelines dictate that these prisoners should be quickly transferred to an external Regional Forensic Psychiatry Service for treatment (Department of Corrections, n.d.; Wakem and McGee, 2012: 93). Strong pressures on external services have, however, meant that ARUs are used as a default waiting room (Office of the Auditor-General, 2008). While segregation has a negative impact on mentally unwell individuals (see Morgan et al., 2007), workers regularly felt ‘that there is nowhere else in the prison’ to go (Harris, 2015: 90).
Alongside these diverse populations, ARU staff dealt with prisoners who had physical health problems, such as those with heart conditions, infectious diseases or bone breakages. They increasingly encountered elderly prisoners who had specialist health requirements, leading some staff to note how their Unit sometimes ran ‘like a geriatric ward’ (Harris, 2015: 51). In addition, staff dealt with those detoxing from drugs or alcohol, including those who had concealed drugs internally.
To add to the mix, the Units were also used to separate gang members, to detain ‘vulnerable’ youth prisoners and to hold those dealing with the grief of bereavement. Non-English-speaking prisoners could also find themselves in an ARU, as their level of risk could not be easily ascertained by staff. Finally, ARU cells filled when the mainstream prison was experiencing a ‘blowout’, meaning that there were simply no other beds elsewhere. ARU staff members described ARUs as ‘the ambulance at the bottom of the cliff’ and ‘the end of the line’ for prisoners who have no other placement options available to them within the wider prison (Harris, 2015: 50).
These findings are supported by a recent report, which noted the relative ease involved in admitting a prisoner to an ARU compared to the process required to segregate a prisoner for behavioural or management purposes, which is regulated by legislation. Inspectors raised concerns that not all prisoners held in ARUs are at risk of self-harm or suicide and should instead be segregated in other areas of the prison. It was noted that practice of this nature undermines the purpose and function of the ARU (Office of the Ombudsman, 2017).
While ARU policy establishes that Units should only be used as a matter of last resort to protect a prisoner’s safety, they served a much broader range of institutional functions. Some ARU prisoners cited suicide or self-harm-related concerns, or enacted visible emotional distress, however many others strongly and repeatedly denied thoughts (and posed no risk) of suicide or self-harm. The elastic term, of being ‘at risk’, could be invoked on the basis of ‘subjective judgements’ and wider institutional demands for security management and control (Hannah-Moffat, 1999: 81). This net-widening – led by institutional pressures or prison staff perceptions of who should receive ARU treatment – demonstrates how risk assessments can be subverted to punish, rather than protect, prisoners. The Units are, then, misused and overused in a way to manage prisoners perceived as both ‘at risk’ and ‘risky’. The end-result is that Unit conditions are worsened, and any opportunities for ARU staff to work constructively with ‘at-risk’ prisoners are seriously undermined.
Lesser Eligibility
In New Zealand, prisoners are entitled to a ‘standard of health care that is reasonably equivalent to the standard of health care available to the public’ (Corrections Act, 2004: s. 75). In practice, this is commonly interpreted as meaning that prisoners should not receive treatment of a standard higher than that found in the community, despite prisoners having significantly higher and more complex health needs (WHO, 2007). This is particularly pertinent in relation to mental health, as the Department of Corrections has previously stated that it does not feel obliged to supply counselling or other treatment options for prisoners with less severe or acute issues, given the lack of these types of services available in the community (Office of the Auditor-General, 2008). A report commissioned by the Office of the Auditor-General (2008: 27) asserted that substandard community services in no way absolves the Department of Corrections’ responsibility to cater to prisoners’ mental health needs.
The institutional acceptance of poor conditions within Units is linked to notions that prisoners are less ‘deserving’ of care or humane treatment. Within Anglophone countries, in particular, the label of ‘prisoner’ has become shorthand for those who must be ‘expelled’ or outcast (Drake and Henley, 2014: 154). Within cultures of popular punitiveness, prisoners’ rights are regularly represented as a societal affront (Stanley, 2011) and common representations invoke that prisoners, who are generally viewed as implicitly to blame for their situation, are ‘less eligible’ for health care or other services (Sim, 1990). Indeed, a recent New Zealand Minister for Corrections, Anne Tolley, supported this view, stating that prisoners ‘shouldn’t get a better health service being in a prison than hard working law-abiding citizens’ (Radio New Zealand, 2013). Such perceptions run counter to international human rights law that establishes that prisoners should receive equivalent standards of care to the general population. The notion of ‘lesser eligibility’ underpins poor conditions within ARUs and the ‘inhumane’ treatment of prisoners.
Conditions
On entry to ARU, prisoners are stripped, searched and given an ‘anti-suicide gown’ before being placed in a cell. They are then kept under 24-hour observation by staff, with minimal light or fresh air. Most ARU cells are monitored via CCTV, which can be viewed by any staff working within the immediate office. Surveillance includes watching prisoners using the toilet and at various stages of undress, with no policy in place preventing staff of opposing genders viewing such activities (Office of the Ombudsman, 2017).
The New Zealand Ombudsman’s Office has recently criticized conditions for ‘at-risk’ prisoners. A now-replaced Unit at Invercargill prison, that detained 25 prisoners in April 2016, did ‘not promote wellness for either staff or prisoners’ (Office of the Ombudsman, 2016b: 18). Beyond their cell, prisoners had access to a small yard that was ‘run-down and bleak with no direct sunlight or seating and mould on the plastic corrugated roof’ (Office of the Ombudsman, 2016b: 18). At Manawatu, ‘at-risk’ prisoners were held in safe cells, in an ‘extremely busy’ and noisy remand unit. With limited natural light or ventilation, the ‘grim’ conditions provided ‘a detrimental environment for individuals already struggling with significant mental health issues’ (Office of the Ombudsman, 2016a: 14).
The Ombudsman further reported daily routines of long lock-downs in ‘barren’ or ‘sparsely furnished’ cells (Office of the Ombudsman, 2016a, 20016c). The daily conditions for an Invercargill ARU prisoner were outlined:
there was no evidence of any current or scheduled specialist input […] His daily routine consisted of being locked in a barren cell (up to 23 hours a day), or in the small run-down external yard. The prisoner was clothed in an anti-rip gown (no shoes). The lack of any positive stimulus for prisoners considered to be at risk is a significant concern. (Office of the Ombudsman, 2016b: 19)
These environments of deprivation combine with conditions in which prisoners enjoy no, or little, external contact or stimulation. There is limited access to the outside world – no television, books, radio and limited access to visitors, despite Corrections policy stating that ‘at-risk prisoners have the same opportunities for involvement in prison activities as other prisoners’ (Department of Corrections, n.d.). Such solitary confinement is prohibited under the UN’s Standard Minimum Rules. 5 Further, it is widely condemned for reinforcing prisoners’ feelings of isolation, hopelessness, anxiety, fear, despair, depression and disempowerment (Bell, 1999; Camilleri et al., 1999; National Health Committee, 2010; Scraton and Moore, 2005; Wakem and McGee, 2012). These ARU conditions can stop prisoners from disclosing their thoughts of self-harm or suicide, as they want to avoid an ARU stint. And, if transferred, the ARU environment can actively contribute to a deterioration in a prisoner’s mental state, particularly for those with pre-existing conditions (Anasseril, 2006). For those ‘at risk’, the ARU can be especially ‘risky’.
Treatment
The notion of ‘less eligibility’ that makes solitary conditions officially acceptable also frames how ARU prisoners are treated by staff. Recent reports have outlined that at-risk prisoners have received ‘no meaningful therapeutic intervention’ to address their self-harming intentions (Office of the Ombudsman, 2016a, 2016b, 2016c: 8). Care has been described as ‘perfunctory’ (Office of the Ombudsman, 2016a: 17). As one ARU officer put it:
Corrections would rather have someone unwell and in a situation where they’re not able to self-harm than put them in an environment that would perhaps give them the opportunity to self-harm but would be more beneficial for them to get better. (Harris, 2015: 58)
Limited therapeutic interventions can also result from staff adherence to rule-following rather than responding to individual prisoner needs during periods of significant distress. In order to manage risk within one ARU, for example, rules were applied inflexibly, even when such an approach resulted in negative outcomes for prisoners. One staff member highlighted this somewhat paradoxical tension:
It’s very, very rigid here […] It’s black and white for Corrections. For example, we had a guy who was having seizures who was being controlled and restrained. So he kept having epileptic seizures and they were controlling and restraining him because he had assaulted someone […] So they put him in the round room, this guy, and I said ‘don’t put him in the round room’ […] they then tried to strip this guy – that made him get angry and have another seizure […] he had another fit and I sent him out by ambulance in the end. We could have contained him here if they’d left him in his ordinary clothing in the ARU. But they had this blanket thing that if you’re in the ARU you have to have the stripped gown. (Harris, 2015: 62)
Risk management practices are regularly framed in a correctional culture of prisoner degradation and mistrust. As Joe Sim (2002: 307) has argued in the UK context, a dominant officer culture exists in which prisoners are viewed as constantly attempting to ‘blag’ the system. Within New Zealand, many ARU staff described prisoners as ‘manipulators’ or ‘malingerers’, trying to get an easier sentence. Reflecting others, one officer described ARU prisoners as ‘hangers-on, the ’fraidy cats who want to come here because it’s the easy option’ (Harris, 2015: 53).
The mistrust of prisoners was especially pronounced for prisoners who were not seen to comply with prison rules and authority. In these situations, workers might engage punitive attitudes that shape risk management practices with devastating effects. This has been particularly clear in the death of 30-year-old Jai Davis in an at-risk cell at the Otago Corrections Facility in 2011.
On arrival to Otago, Jai Davis was regarded as a security risk. Corrections staff had received information that he had internally concealed drugs. Staff classified him as being ‘at risk’ and illegitimately moved him to an at-risk cell, complete with anti-suicide gown, so that they could actively observe him, ‘catch him’ when the drugs emerged and charge him with smuggling contraband (McKay, 2014). In the at-risk cell, Jai began to vomit blood before he passed out for some time. Over two days, he was not seen by a doctor or taken to hospital and subsequently died in the cell (New Zealand Coroners Court, 2015).
During his inquest, a duty nurse considered that the prison’s at-risk facilities were an ‘accident waiting to happen, and [that] people were going to die due to nurse neglect’ (McKay, 2014). She recounted how a nurse that managed Jai Davis frequently referred to other ARU prisoners as ‘guilty little fuckers’ (McKay, 2014). She depicted a punitive, security-oriented response that took precedence over providing care for urgent and obvious health needs. That punitive response was masked by the use of an at-risk cell, which perhaps suggested a more therapeutic approach than was actually employed. At the conclusion of the inquest hearing, the Coroner noted that the initial police inquiry into the death was ‘cursory and flawed’ and not conducted in a timely manner, ultimately compromising the outcome of the coronial inquiry (Dougan, 2015; McNeilly, 2015). The Coroner later noted it would be in the public interest for the Independent Police Conduct Authority (IPCA) to scrutinize the role of police in their investigation into the circumstances of Davis’ death. A subsequent police investigation concluded that there was insufficient evidence to prosecute any correctional staff working at the time (McNeilly, 2015). The case of Davis not only highlights the inherent limitations of ARUs in their ability to protect the life, but also the indifferent attitudes among staff towards ‘lesser eligible’ prisoners who are legitimately at risk of harm and who require responsive care and treatment. 6
Legal Compliance over Humane Treatment
A further issue relates to how risk management is intimately tied to the state’s need to comply with international human rights obligations. Under a risk-averse strategy, prison managers view human rights claims as ‘organizational risks’ that they wish to avoid – publicity about the bad treatment of detainees can undermine an institution’s reputation but it can also lead to significant costs in legal battles or fines
7
(Whitty, 2011: 124). As outlined by one ARU nurse:
[The staff] are worried about the risk that they take if they don’t put [prisoners] at-risk and they hang themselves. It’s high-risk, you make a mistake like this and it goes to the paper and as much as you don’t want to, you do end up taking the can for it. So the officers, because of the culture of the department, the risk averse culture, they don’t want to be the ones to say that he’s not at-risk and then he hangs himself. (Harris, 2015: 59)
In a period in which the poor treatment of prisoners can bring (short-term) reputational and financial costs, human rights obligations have regularly been distorted. For example, ARUs have been established to protect ‘the right to life’. Yet, in a bid to prevent prisoner deaths, ARUs regularly prioritize interventions that are not rights-regarding. Bare cells, anti-ligature gowns, solitary conditions or 24–7 monitoring may prevent suicide but they are questionable as humane responses (Scraton, 2007). In New Zealand, cameras watch prisoners sleep, sit, walk about their tiny space and even go to the toilet. The Ombudsman has recently queried the need for surveillance over the lavatory, viewing it as a degrading violation of privacy. They saw no ‘evidential basis’ that ‘at the particular time that prisoners use the lavatory there is in fact the ability to self harm’ (Office of the Ombudsman, 2016c: 14–15). In response, the Department has argued that ‘privacy […] must be secondary to the risk posed to a prisoner’s life’ (Department of Corrections, 2016). The result is that the person does not die, or they may be less likely to die. But, along the way, any semblance of humanity or dignity for individuals suffering in extreme circumstances is removed (Moore and Scraton, 2013).
Many institutional responses to prevent prisoner suicide may gain a certain degree of legitimacy. ARUs rely on medical discourses to explain the risks of self-harm and suicide (Scraton, 2007). There is also a ‘quietness’ to surveillance, architectural modifications or clothing that can hide the depths of prisoner despair (Crewe, 2011; Scraton, 2007). However, some initiatives towards ARU prisoners are more obviously challenging to onlookers. For example, in some jurisdictions, physically intrusive control and restraint mechanisms, such as the use of tie-down beds, are also endorsed when the risk of suicide is high (EHRC, 2012; Victorian Ombudsman, 2014; WHO, 2007). In the United States, reports have described prisoners chained to beds and forced to wear ‘leg irons’ to prevent self-harming behaviour (Livingstone, 2000). The UN (2015: Rules 47–48) confirms that restraint instruments that ‘are inherently degrading or painful shall be prohibited’. They must only be used to prevent self-harm when all ‘other methods of control fail’. In such circumstances, physicians and higher administrative authorities must be alerted and restraints should be the ‘least intrusive method’ possible. All restraints should be removed ‘as soon as possible after the risks posed by unrestricted movement are no longer present’.
In New Zealand, restraints have been used on the claims of maintaining the right to life. In 2016, the Ombudsman undertook an unannounced visit to Otago prison. They found an ARU prisoner who: ‘was being managed in a waist restraint with his hands cuffed behind his back (for approximately 10 weeks) due to his self-harming’ (Office of the Ombudsman, 2016c: 17, emphasis added). For two-and-a-half months, the man had spent at least 21 hours a day in the restraint:
He was un-cuffed every two hours during the day and every four hours at night in order to stretch his muscles, take a shower or eat his meals (average three hours unlock a day). He was able to watch some TV in his cell from late afternoon. (Office of the Ombudsman, 2016c: 18)
The monitoring body highlighted that this prolonged restraint was ‘disproportionate and unreasonable’. Being ‘in prolonged restraints’ placed a ‘huge strain on the person’, causing ‘significant physical and mental distress’ – it was ‘a torturous experience’ (Office of the Ombudsman, 2016c: 18). While restrained in this way, there was ‘no evidence of therapeutic intervention of psychological support […] having taken place’ for this prisoner or any other in the ARU (Office of the Ombudsman, 2016c: 18). It is certainly difficult to see how this restraint use could adhere to the ‘least intrusive’ or minimum duration rules established by the United Nations.
Within ARUs, the managerial prevention of death (sometimes encompassing violent containment for legal human rights compliance) takes precedence over any nurturing of life. While health care professionals do work in ARUs, it is also apparent that their ‘care’ input can be subverted by institutional cultures and operations that emphasize control and punishment within an intensely narrow context of legal compliance and bureaucratic risk management. The end-result is that ARU practices can give the illusion of health care and progressive interventions towards those made most vulnerable by their life or incarceration experiences while, on the floor, they increase risks for prisoners in many, varied ways.
Avoiding Sanction
Internationally, legal and administrative mechanisms for human rights protections offer relatively limited opportunities for change. Monitoring bodies and courts tend to be ‘avowedly state-centric’ as they work within state-defined processes and structures (Weber and Pickering, 2011: 213). They rarely raise challenges to the broader institutional or social conditions that make prisoners susceptible to self-harm or suicide, or contest the problems of prison facilities, neglectful conditions or inhumane treatments (Scott, 2013). In the New Zealand context, prisoners’ rights are regularly ‘read down’ within court cases, and arguments that security, compliance or safety should be prioritized over rights can dominate the legal landscape (Stanley, 2011; see also Drake, 2012). There are no regional human rights courts – like the European Court for Human Rights – which means that prisoners have few options once their case has progressed through the New Zealand system. Monitoring bodies for prisons are also relatively weak. There is no independent prison inspectorate, and monitoring organizations like the Ombudsman or the Human Rights Commission are under-funded given their scope of work (Stanley, 2016). Nonetheless, as the sections above demonstrate, these bodies have sought to expose the maltreatment of those held in ARUs in recent years.
In the wake of pressures from monitoring bodies, there has been a limited shaming of the Department in relation to the poor treatment of ‘at-risk’ prisoners. However, one recent case – that of Nicholas Harris, who died in an At-Risk Unit in 2011 – demonstrates the way in which further sanctions for ARU prisoner deaths or ill-treatment can be avoided. Nicholas Harris had engaged in serious self-harm within the ARU at Waikeria prison. After being observed, he subsequently died while being restrained by a number of prison staff, with his cause of death being formally attributed to a combination of asphyxia and morbid obesity. In the Inquest to establish the cause of his death, the Coroner blamed Nicholas Harris for his risk-creating behaviours, stating:
The major contributing factors in the death of Mr Harris were his attitude and behaviour towards [staff] which necessitated a robust spontaneous control and restraint process […] if Mr Harris had not created a high degree of risk around himself, and if he had been compliant rather than resistant, it is likely the officers […] would have been able to assess his medical condition. (New Zealand Coroners Court, 2012: 73)
The Coroner referred to Harris’ mental state as a ‘luxury’ that staff did not have the capacity to consider (New Zealand Coroners Court, 2012: 77). The implication, here, was that mental health or ‘right to life’ considerations should be an optional or secondary concern in volatile situations where institutional or staff safety was compromised. Nicholas Harris had not harmed anyone other than himself. Yet, his ‘risks’ changed from being a mental health issue into an issue of management, control and safety.
Harris’ case highlights how ‘institutional discourses of risk make individuals responsible for their own safety management […] [and] encourage the attribution of blame by attaching risk to individuals who are marginalised or in need of specialist care’ (Mythen, 2014: 37). In Nicholas Harris’ case, the responsibility of Corrections to uphold a ‘duty of care’ was abdicated. Ultimately, given the way discourses of risk and compliance are currently operationalized, at-risk prisoners are made ultimately responsible for themselves. This diverts attention away from the human rights obligations placed on state institutions to provide safe, dignified or respectful conditions for those they detain.
Conclusion: Risk and Human Rights
Scholars have long noted that law and order policy has moved away from ‘justice’ as a central ideological commitment, with a shift towards ‘risk’. Risk management has become ‘a key organising principle of contemporary correctional practice and offender management’ (Feeley and Simon, 1992; Maurutto and Hannah-Moffat, 2006: 438). As a means of ensuring efficiency, cost-effectiveness, good order and the ‘avoidance of failure’, prisoners have become increasingly classified by levels of assessed dangerousness, via the use of risk assessment tools and other actuarial techniques (Whitty, 2011: 126). In doing so, ‘individualised diagnosis and response is displaced by aggregate classification systems for purposes of surveillance, confinement and control’ (Feeley and Simon, 1992: 452). Risk and justice are presented as paradoxical, in the sense that ‘risky’ individuals are no longer viewed as legitimate recipients of human rights or procedural justice.
This would seem to be the case in terms of the introduction and implementation of At-Risk Units. While ARUs appear to represent a new human rights conscious means by which prison authorities can ensure safety for those at risk of harm or suicide, they are regularly operationalized in ways that enhance risks and diminish rights for prisoners. Further, they increasingly legitimize notions of containment, security and force on the grounds of prisoner ‘well-being’.
For vulnerable prisoners, ARUs and other harmful containment mechanisms, such as tie-down beds, can – deliberately or inadvertently – be used to punish or degrade those requiring tailored, care-oriented treatment. Distressing conditions, combined with negative treatments by some staff who view prisoners as ‘less eligible’, create increasingly ‘risky’ environments for those sent to At-Risk Units. Such risks are enhanced by a correctional culture that can prioritize legal or institutional rule-compliance – a baseline ‘death-avoidance’ approach – over the need to respond to prisoners with dignity or respectful care (Cliquennois and Champetier, 2012: 397; Livingstone, 2000).
As long as institutional or policy requirements are upheld, the individual needs of a diverse range of prisoners are left unaccounted for. Moreover, normative levers, conventions and tools that are intended to protect prisoners against ill-treatment can be lost or subverted when pitted against the day-to-day institutional realities and requirements of a correctional environment. In conclusion, ARUs have frequently exacerbated rather than reduced risk, and have diminished the status of prisoners as legitimate recipients of health services or humane, just treatment. A question remains about their fundamental use as an appropriate response to those who suffer mental health distress within penal environments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/ or publication of this article: This writing of this article was supported by a Rutherford Discovery Fellowship, administered by the Royal Society of New Zealand, and funded by the New Zealand government.