
Abstract
Introduction:
A fatal cardiac arrest in 2022 caused by a local anaesthetic overdose highlighted significant gaps in local anaesthetic safety, including inconsistent documentation, variable dosing practices, and inadequate communication. This quality improvement project aimed to improve local anaesthetic safety through standardised documentation, ideal body weight–based dosing, and structured multidisciplinary communication.
Methods:
A pre–post intervention study was conducted at a district general hospital in South East England. Baseline data were collected using structured questionnaires completed by Operating Department Practitioners during surgical cases. Interventions, informed by national anaesthetic safety guidance, included standardised local anaesthetic documentation, mandatory ideal body weight–based dose calculation, surgeon-led vial checks, and routine discussion of local anaesthetic use during preoperative briefings. Post-intervention data were collected using the same methodology across cases.
Results:
Documentation of local anaesthetic administration in the anaesthetic chart increased from 68% (19/28) pre-intervention to 91% (29/32) post-intervention. The use of ideal body weight–based dosing increased from 29% (8/28) to 94% (30/32). Discussion of local anaesthetic during the preoperative brief improved from 82% (23/28) to 100% (32/32). The number of local anaesthetic overdoses decreased from two cases pre-intervention to one case post-intervention, with no associated patient harm.
Conclusion:
Targeted multidisciplinary interventions, including standardised documentation, structured communication, and ideal body weight–based dosing, resulted in substantial improvements in local anaesthetic safety. These findings support the adoption of simple, scalable safety measures to reduce dosing errors and enhance perioperative patient safety.
Keywords
Introduction
On 12 April 2022, a 47-year-old doctor experienced a cardiac arrest following a hip replacement surgery at Spire Lea Hospital in Cambridge (Heywood 2024). She died 3 months later at Addenbrooke’s Hospital due to a hypoxic-ischaemic brain injury, resulting from a cardiorespiratory arrest triggered by an overdose of local anaesthetic (LA). Motivated by this case in the news, our project aimed to evaluate and improve LA practices at a district general hospital. Specifically, we sought to assess the types, dosages, and routes of administration of LA used in surgical settings. We also aimed to identify the healthcare professionals responsible for verifying and administering LA, as well as the locations where LA administration was documented. Based on these findings, we implemented targeted interventions with the goal of achieving a minimum of 90% compliance across all measured parameters.
Background
The circumstances of the death described above are outlined in the coroner’s inquest: The intention in this case was for a 0.2% solution of Ropivacaine to be diluted 50/50 with normal saline before it was infiltrated. The evidence suggested that this was not done. The result was that excessive Ropivacaine was administered by mistake. (Barlow 2024, ‘Circumstances of the Death’)
Local anaesthetic systemic toxicity (LAST) is a rare yet potentially fatal complication. Although UK specific data regarding the incidence of LAST is limited, data from USA-based registries have provided an incidence of 0.03%, which is equivalent to 0.27 peripheral nerve blocks (Gitman & Barrington 2018). While the most frequent cause is accidental intravascular injection of LA, other risk factors include pre-existing conditions such as liver impairment, cardiovascular disease, and pregnancy, all of which may increase a patient’s susceptibility to overdose (Mahajan & Derian 2022). In this case, however, the cause was an accidental overdose due to incorrect preparation of LA rather than intravascular injection.
LAST can manifest as central nervous system and cardiovascular system dysfunction including seizures, impaired contractility, and life-threatening arrhythmias (El-Boghdadly et al 2018). Prompted by the incident in question alongside the concerns highlighted in the coroner’s report and the suggestion from the Royal College of Anaesthetists and the Association of Anaesthetists, we sought to evaluate the LA practices at this hospital. A fishbone diagram was created to identify the factors contributing to the lack of standardised LA protocols (Figure 1).
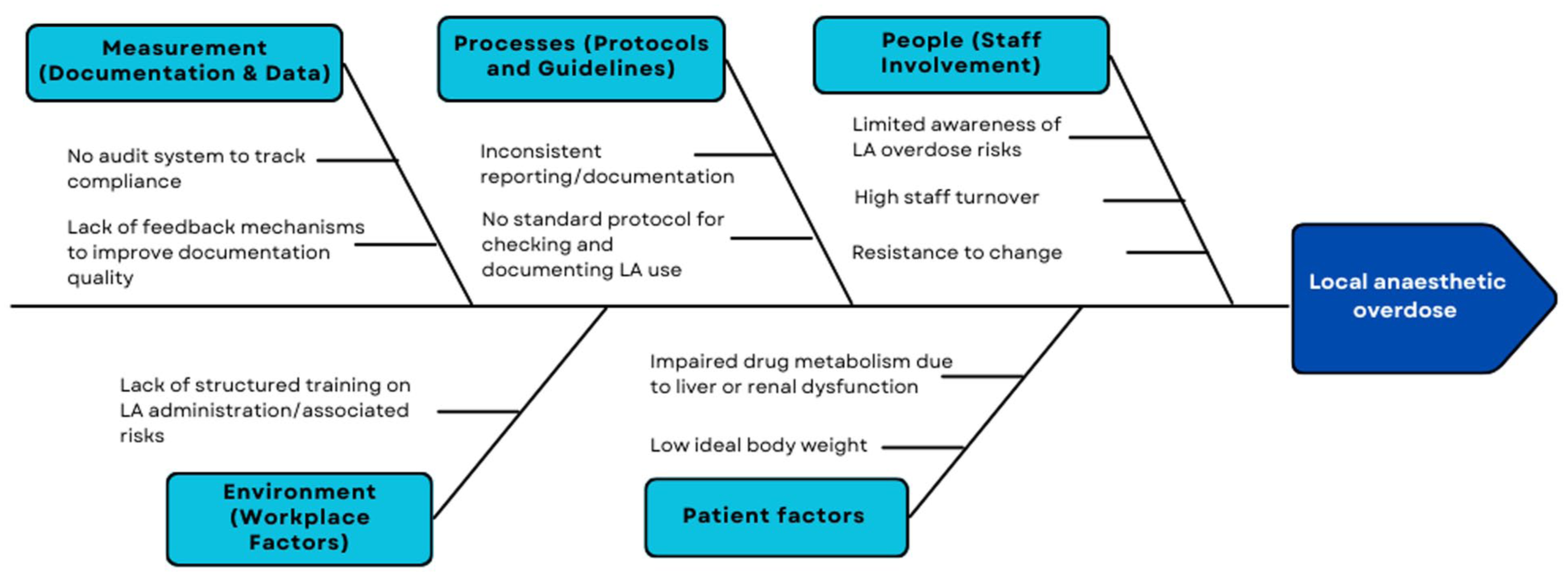
Fishbone analysis identifying factors contributing to the lack of standardised protocols for safe local anaesthetic (LA) administration and documentation
Materials and methods
This fishbone analysis, also known as an Ishikawa diagram, illustrates key contributors to unsafe local anaesthetic practice. Contributing domains include documentation and data processes, existing protocols, staff involvement, workplace factors, and patient factors. These categories were used to guide the development of targeted interventions in the pre-post intervention study.
Measurement
We selected four primary outcome measures to assess both process and outcome changes. These included whether the dose and route of administration were discussed during the pre-surgical brief, whether the LA dose was calculated using the patient’s ideal body weight, whether the administration of LA was documented in the anaesthetic chart, and whether the surgeon verified the LA dose prior to administration. These measures were chosen for their relevance to key safety steps in LA administration and were informed by baseline data collection. These outcomes were selected through discussions between members of the team and the supervising senior anaesthetists.
To achieve our compliance target of at least 90% across all parameters, we focused on evaluating the types, dosages, and routes of LA administration, identifying the healthcare professionals involved in verifying and administering LA, and determining where LA documentation was routinely recorded. Our objectives were to comprehensively assess the dosages and routes of LA used, to clarify which anaesthetic agents were selected, to establish which staff members were responsible for verification and administration, and to locate the points of documentation within the patient care pathway.
Design
To ensure objective data collection, questionnaires produced by the team were distributed to the Operating Department Practitioners (ODPs) and anaesthetic assistants, including nurses, who were asked to complete them anonymously based on intraoperative practices they observed. ODPs and anaesthetic assistants were selected as observers because they are consistently present in operating theatres and share similar responsibilities in theatres. To demonstrate that the outcomes observed were attributable to our interventions, the same questionnaire was distributed to ODPs both before and after the implementation phase. Pre- and post-intervention cycles were completed to assess the efficacy and impact of our interventions.
Pre-intervention study
Our pre-intervention study took place between 22 October 2024 and 28 October 2024. A dedicated member of the team, consisting of three medical students and two anaesthetists, delivered the questionnaires to ODPs before the surgical lists began to maximise the number of responses per day. Our objective was to identify what the common practices were in the theatres, specifically if discussions regarding LA use took place during the pre-surgical brief, whether surgeons were checking the LA dose and route before administration and if there was a standardised method of documenting the LA. We prioritised orthopaedic, obstetrics and gynaecology, and general surgery theatres given their high volume of cases and frequent use of LA and provided questionnaires to each theatre on consecutive days during the aforementioned period. We predicted that the current practice would involve these parameters, ideally resulting in a very low frequency of LA errors and overdoses. Figure 2 illustrates the baseline data collected during this study, highlighting the frequency of compliance with each of the outcome measures.
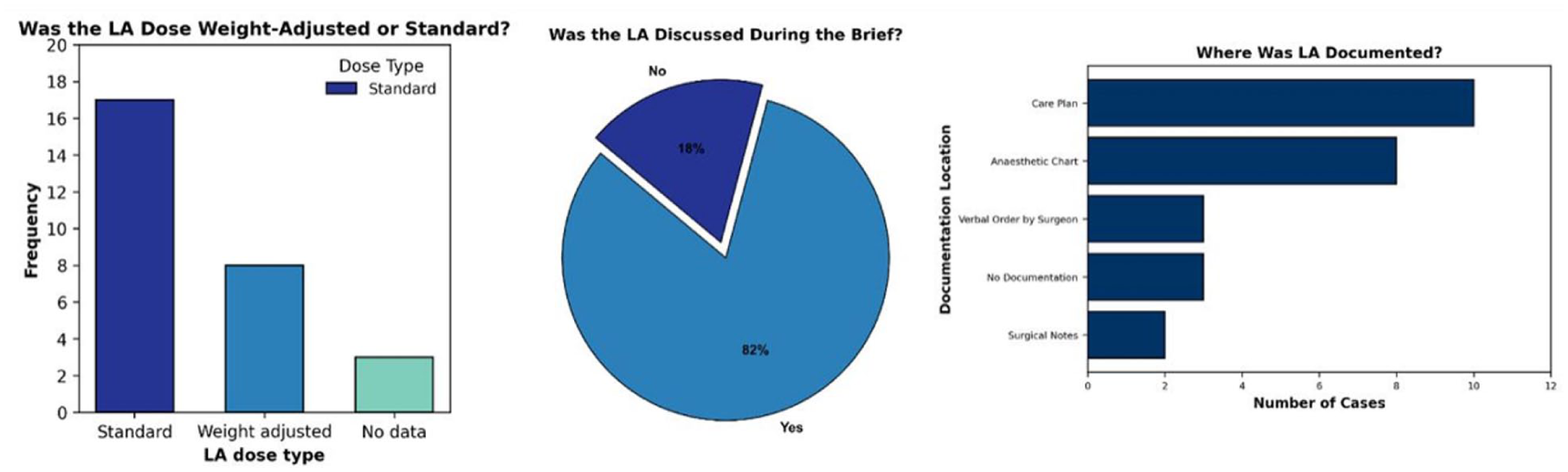
Pre-intervention documentation and dosing of local anaesthetic (LA) in surgical procedures. (a) Bar chart showing the type of LA dose used during the pre-intervention data collection period. Standard doses were used more frequently (n = 17) than weight-adjusted doses (n = 8), with three cases lacking documentation on dose type. (b) Pie chart depicting whether LA was discussed during the surgical brief in the pre-intervention cohort. LA was discussed in 82% (23/28) of cases, while 18% (5/28) had no discussion recorded. (c) Bar chart displaying the locations of LA documentation in the pre-intervention dataset. The most common site of documentation was the care plan (n = 10), followed by the anaesthetic chart (n = 8). Verbal order by surgeon and no documentation were both recorded in three cases, while surgical notes contained documentation in only two cases
After this study, results were presented at the departmental audit meeting. This generated focused discussion on safe and consistent documentation of LA dosing, as well as clarification of roles in verifying doses. A set of practical improvement measures was agreed upon, combining input from the clinical team with recommendations from the Royal College of Anaesthetists (RCoA) (Royal College of Anaesthetists, 2024). These measures included discussing LA dosage during the multidisciplinary team (MDT) brief, recording the LA dose as ‘the volume in ml of a solution containing a specified number of mg/ml of a named local anaesthetic’, documenting LA in the care plan, ensuring that surgeons check vials before use, calculating LA dose using ideal body weight for every patient, and documenting LA infiltration in the anaesthetic chart. These findings were presented and discussed during the theatre safety huddle with operating theatre staff, where the improvement measures were reviewed and reinforced.
Given the variations in documentation and discussion regarding local anaesthetic use, we aimed to standardise practice with the use of posters placed in each of the main theatres in the hospital, with each poster consisting of reminders and prompts regarding the discussion, documentation, and confirmation of dose and routes of local anaesthetic administration (Supplemental Appendix A). The prompts incorporated in these posters were formulated through discussions between the team and the rest of the anaesthetic department during the audit meeting, ensuring all members of staff agreed with the implementations and their respective predicted efficacies. Moreover, the reminders mentioned in the posters were in line with the recommendations put forward by the coroner’s report and the Royal College of Anaesthetists. To raise awareness of this initiative, emails were sent out to departmental leads, and the initiative was discussed in departmental huddles prior to starting the surgical lists (Ellis et al 2023).
The impact of this intervention was assessed with a second series of questionnaires for the ODPs to complete, focusing on where the LA was documented, if weight-adjusted doses were utilised and if the LA dosage and route was discussed in the pre-surgical brief. Responses were collected after 1 week, followed by data analysis by the team. We anticipated that we may receive a small number of responses due to some ODPs not having enough time during the day to fill these questionnaires out or perhaps not filling them correctly, which we aimed to mitigate through ongoing discussion within the team regarding updates of responses, how we could increase responses and which theatres would be best to target.
Post-intervention study
We produced two educational posters to be distributed in the main theatres; one focused on raising awareness of the fatal case of LAST, as well as the most pertinent findings from our pre-intervention cycle. The second poster consisted of a series of steps that should be followed to ensure there is safe practice around documentation, discussion, and administration of LA. These posters were accompanied by emails sent to the departmental leads and discussion during team huddles. A second, revised questionnaire was formulated, as per the anaesthetic team recommendations, to assess the impact of our interventions. The posters were placed in the theatres on 20 December 2024, and the questionnaires were handed out between 21 January 2025 and 28 January 2025, followed by analysis by the project team.
Results
The results from the post-intervention study showed improvement in all areas. All 32 cases had local anaesthetic (LA) use discussed in the pre-surgical brief (100%). Ninety-four percent (30/32) of the cases had LA administered using ideal body weight, and the surgeon checked the dose 91% (29/32) of the time pre-administration. In addition, 91% (29/32) of prescriptions were recorded in the anaesthetic chart and 91% (29/32) in the care plan, demonstrating improvement in standardisation. Across both cycles, we obtained data from 60 surgeries (cycle 1 n = 28, cycle 2 n = 32), as illustrated in Figure 3.
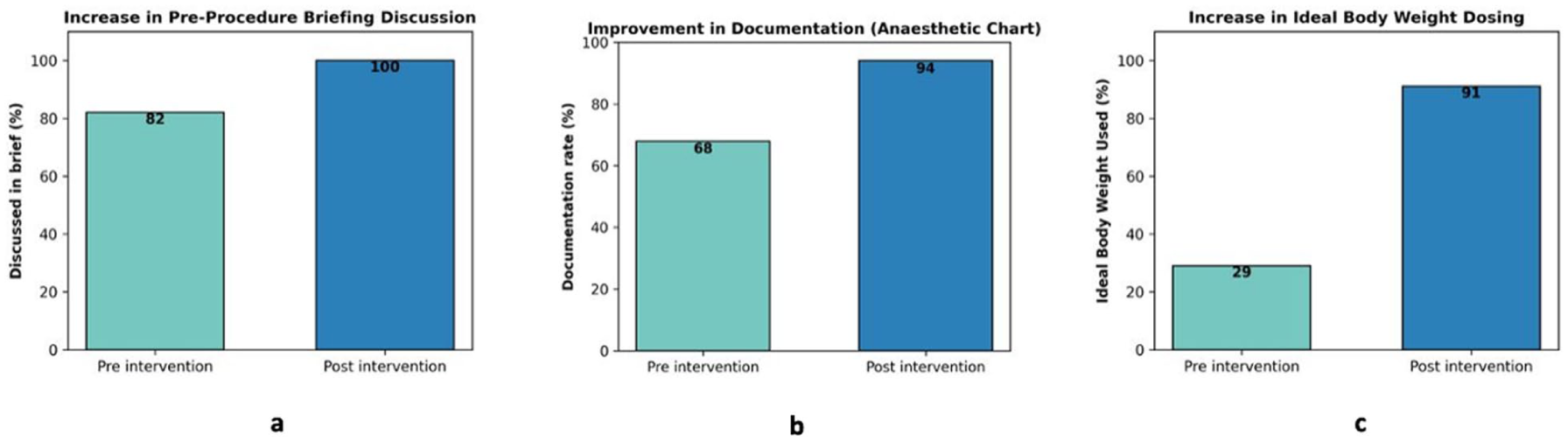
Improvements in local anaesthetic (LA) safety following intervention: pre–post comparison. (a) bar chart showing the increase in use of ideal body weight–adjusted dosing, rising from 29% (8/28) pre-intervention to 94% (30/32) post-intervention. (b) Bar chart depicting the frequency of pre-procedure briefing discussions about LA, which increased from 82% (23/28) before the intervention to 100% (32/32) after the intervention. (c) Bar chart showing improvement in documentation of LA administration in the anaesthetic chart, increasing from 68% (19/28) pre-intervention to 91% (29/32) post-intervention
The proportion of cases using ideal body weight rather than a standardised dose increased substantially from 29% (8/28) in cycle 1 to 94% (30/32) in cycle 2 (Figure 3(a)). The frequency of pre-procedure briefing discussions increased from 82% (23/28) to 100% (32/32) between the two cycles (Figure 3(b)), demonstrating meaningful improvement in local anaesthetic discussions prior to surgery. Documentation compliance increased from 68% (19/28) in cycle 1 to 91% (29/32) in cycle 2 following our interventions (Figure 3(c)). One overdose of 2.04 mg/kg of levobupivacaine (maximum dose 2.00 mg/kg) was identified in the post-intervention cycle compared to two overdoses in the pre-intervention cycle (Table S1). Both cases of overdose were identified by an anaesthetist retrospectively. No clinical symptoms of overdose were observed, and the incident was reported through Datix so that it could be addressed appropriately.
Discussion
We believe our project has been successful in providing a concise, coherent, and effective method of documenting and enhancing safety around the use of LA. Our aims to achieve 90% compliance in key parameters of LA practice have been met. However, in our second cycle, we identified two cases (6%) where LA was not documented. Further investigation is required to identify any potential barriers stakeholders faced in following the checklist.
Our results align with previous initiatives involving implementation of checklists in anaesthesia. The use of an anaesthesia preinduction checklist (APIC) increased the knowledge of critical information (100% vs 90%), information exchange (100% vs 33%), perception of safety (91% vs 84%), and perception of teamwork (90% vs 86%) when compared to a control group (Tscholl et al 2015). The results from this study, alongside our own, demonstrate that targeted interventions can help mitigate known risk factors. Development of a standardised checklist proved beneficial in enhancing the safety of LA documentation in this hospital. Our project reinforces principles established by existing literature, emphasising that safe systems in anaesthesia should include a simple, linear, and standardised design, involving double checking ampoules and equipment (Kothari et al 2010).
A major strength of this project is its practical and scalable interventions, which can be easily adapted across different NHS trusts to improve local anaesthetic safety. Further distribution of questionnaires could help to improve patient safety and embed these practices as part of departmental culture. Multidisciplinary engagement contributed to the project’s sustainability, aligning with the Sustainable Quality Improvement (SusQI) framework (Mortimer et al 2018).
A limitation of this project is that we are trying to change culture and practices using an educational intervention. While we have shown an improvement in all our measured parameters by discussing our results and planned interventions with theatre staff, it is unclear how long this effect may last. Posters are displayed in all anaesthetic rooms; however, there is a risk that these may be overlooked. Future interventions may look at a system-wide change, such as a modification to the World Health Organization Surgical Sign In. The proposed changes encountered some resistance initially, especially from team members who felt they had been working effectively with no harm to patients. However, discussing the coroner’s report highlighted the implications of poor practice on patient safety. In addition, our short data collection period and small sample size in this single-centre study limits the assessment of temporal variation and reduces generalisability. Furthermore, data collection relied on ODPs who were aware of our study and what our aims were, which may have introduced response bias. Despite these limitations, we did obtain enough data to identify an immediate process and safety issue. Additional data collection and further interventional cycles may yield greater insights into long-term trends and further areas of improvement.
Conclusion
Overall, we were able to reach and exceed our predefined targets of attaining a minimum of 90% across the parameters studied. The success of these interventions demonstrates how targeted education for healthcare professionals about the risks of local anaesthetics and the importance of standardised documentation can result in meaningful improvements in clinical practice. We aim to ensure that there is continued retention and improvement of these parameters through the implementation of further post-intervention studies and consideration of wider system changes so that standards of local anaesthetic practice remain consistently high after the project has concluded. Ultimately, sustaining these improvements will contribute to a safer perioperative environment and reduce the risk of patient harm.
Supplemental Material
sj-docx-1-ppj-10.1177_17504589261454167 – Supplemental material for Safer local anaesthetic practices through multidisciplinary engagement: A pre–post intervention study
Supplemental material, sj-docx-1-ppj-10.1177_17504589261454167 for Safer local anaesthetic practices through multidisciplinary engagement: A pre–post intervention study by Cansu Ozdemir, Aksh Tailor, Chimba Mubanga, George Clews and Priya Krishnan in Journal of Perioperative Practice
Footnotes
Author contributions
CO and AT conceived the study and are co-first authors. All authors contributed to study design, data collection, analysis, manuscript drafting, and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
This study was conducted as a quality improvement project aimed at evaluating and improving local anaesthetic safety practices within routine clinical care. Formal ethical approval was not required, in accordance with the UK Health Research Authority (HRA) guidance, as the project did not involve randomisation, deviation from standard care, or the collection of identifiable patient data. The project was reviewed and approved locally by the relevant departmental governance and audit leads at Medway Maritime Hospital NHS Trust as a service evaluation/quality improvement initiative.
Consent to participate
Individual patient consent was not required, as no identifiable patient data were collected, and all data were recorded in an anonymised and aggregated format as part of routine quality improvement activity.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.