
Abstract
Background:
Long-term psychological complications of ECMO have been reported and current national guidelines state that there should be access to psychologists for patients in intensive care; however, this is not available in all ICUs. This project was based in a cardiothoracic critical care unit (CTCCU) of a hospital in the north-west of England that does not currently have a psychologist. Therefore, the aim of this project was to identify the psychological needs of ECMO patients. A subsidiary aim was to develop and trial an ECMO-specific group intervention.
Methods:
The prevalence of mental health difficulties in ECMO patients was investigated using data from outcome measures completed 6 weeks post-discharge. Patients were interviewed about their experiences of ECMO, and themes were identified using a thematic analysis. Based on these themes, a pilot 6-week group was developed, and quantitative and qualitative outcomes were collected.
Results:
Analysis of post-discharge HADS found 50% of patients scored within the clinically significant range for anxiety and 37% for depression. Patient themes included feeling powerless, alone and fears around ‘what is normal?’. The ECMO group was well-received by patients, with feedback that they felt ‘seen and heard’. Despite the small sample size, the group demonstrated positive outcome data, with a 66% decrease in anxiety symptoms and a 78% decrease in depression symptoms.
Conclusions:
This project highlighted significant mental health distress for ECMO patients. Positive psychological outcomes were gained from the ECMO group and recommendations were made that embedding psychologists within CTCCU could promote post-traumatic growth for patients.
Introduction
Extra corporeal membrane oxygenation (ECMO) is a form of mechanical circulatory support, used in the management of life threatening pulmonary and/or cardiac failure. It is typically used as temporary support for critically ill patients when other treatment forms are unlikely to be successful. 1 It can be used to allow time for organs to heal or as a bridge to heart or lung transplantation. 2
Common complications associated with ECMO include renal failure, bacterial pneumonia and bleeding. 3 Long term complications also included increased risk of depression, anxiety and post-traumatic stress 4 , with a recent systematic review reporting a depression prevalence of 31% and an anxiety prevalence of 36% in patients at least 6 months post discharge from ECMO. 5 The need for a mental health follow-up and psychological support post discharge has also been identified,6,7 with high levels of emotional distress associated with ECMO-related physical disability 8 and delusional experiences post ECMO. 9
The Guidelines for the Provision of Intensive Care Services highlight the role of Psychologists within critical care teams to provide psychological assessment and support for all alert patients in intensive care, family members and staff. 10 The National Institute of Clinical Excellence (NICE) guidelines similarly recommend both psychological assessment and intervention for patients in rehabilitation after a critical illness. 11 As a result, the need for a minimum of one full time psychologist for every 10 beds on the ICU is recommended and the psychologists in Intensive Care UK Group (PINC UK) recommend a psychological review at an outpatient critical care follow-up clinic approximately 3 months post discharge. 10
There is currently no psychology provision for patients on the cardiothoracic critical care unit (CTCCU) at this large hospital in the North-West of England and this unit is currently on the risk register due to this. Therefore, the aim of this project is to explore the psychological experiences of ECMO patients discharged from the CTCCU at this hospital, to help identify psychological needs and to make recommendations on how these needs can be addressed. A further aim is to develop an ECMO specific group intervention, based upon the identified themes.
Methodology
Participants
Patients who received their 6-week ECMO follow up MDT in the last 2 years were identified and data from the outcome measures completed at the time were collated, including the Hospital Anxiety and Depression Scale (HAD Scale 12 ). Twenty patients were identified, with 16 of these having completed the outcome measures at follow up. All patients were contacted via email or letter to invite them to participate in the project and eight agreed to be interviewed.
All 20 patients were invited to attend the ECMO group and five agreed to attend. Four of the attendees also completed the patient interviews.
Design
A qualitative design was used to explore participant experiences of ECMO through semi-structured interviews conducted over the telephone by a Trainee Clinical Psychologist. Participants were informed that the interview data would be collated and anonymised to maintain confidentiality.
The interview focussed on patient experiences both during and after their admission to CTCCU, in addition to an exploration of the psychological support they received from the team. The interview topic guide was developed using themes highlighted in the existing literature and the clinical experience of a Consultant Intensivist, Specialist Nurse working in CTCCU and Consultant Clinical Psychologist. Patients were also asked what they felt would have been helpful to support their emotional wellbeing and any recommendations they had for the team.
A pilot ECMO group was developed based upon themes identified in the existing literature and themes from the patient interviews. Patients provided post-group feedback on their experience of attending the group and completed pre/post-treatment outcome measures.
Analysis
The themes from the interviews were identified by a Trainee Clinical Psychologist using thematic analysis to help identify patterns across ECMO patients and then discussed with the supervising Clinical Psychologist. Braun and Clarke’s 13 six-step framework was used to perform the thematic analysis including: (i) familiarisation of the data through transcribing and reading through the interviews, (ii) highlighting important information through the generation of initial codes, (iii) creating broader themes from these codes, (iv) reviewing the themes, (v) refining and naming each theme and (vi) writing up the narrative.
Results
Part 1: Prevalence in follow up data
16 out of 20 patients discharged in the last 2 years completed outcome measures at the MDT follow up (see Figure 1). 50% of patients scored within the clinically significant range for anxiety on the HADS (within the moderate or severe range), with 31% of these in the ‘severe range’. In addition to this, 37% of patients scored within the clinically significant range for depression with 25% of these within the ‘severe range’. For 50% of patients, a referral was made or had already been made to local mental health services at follow up.
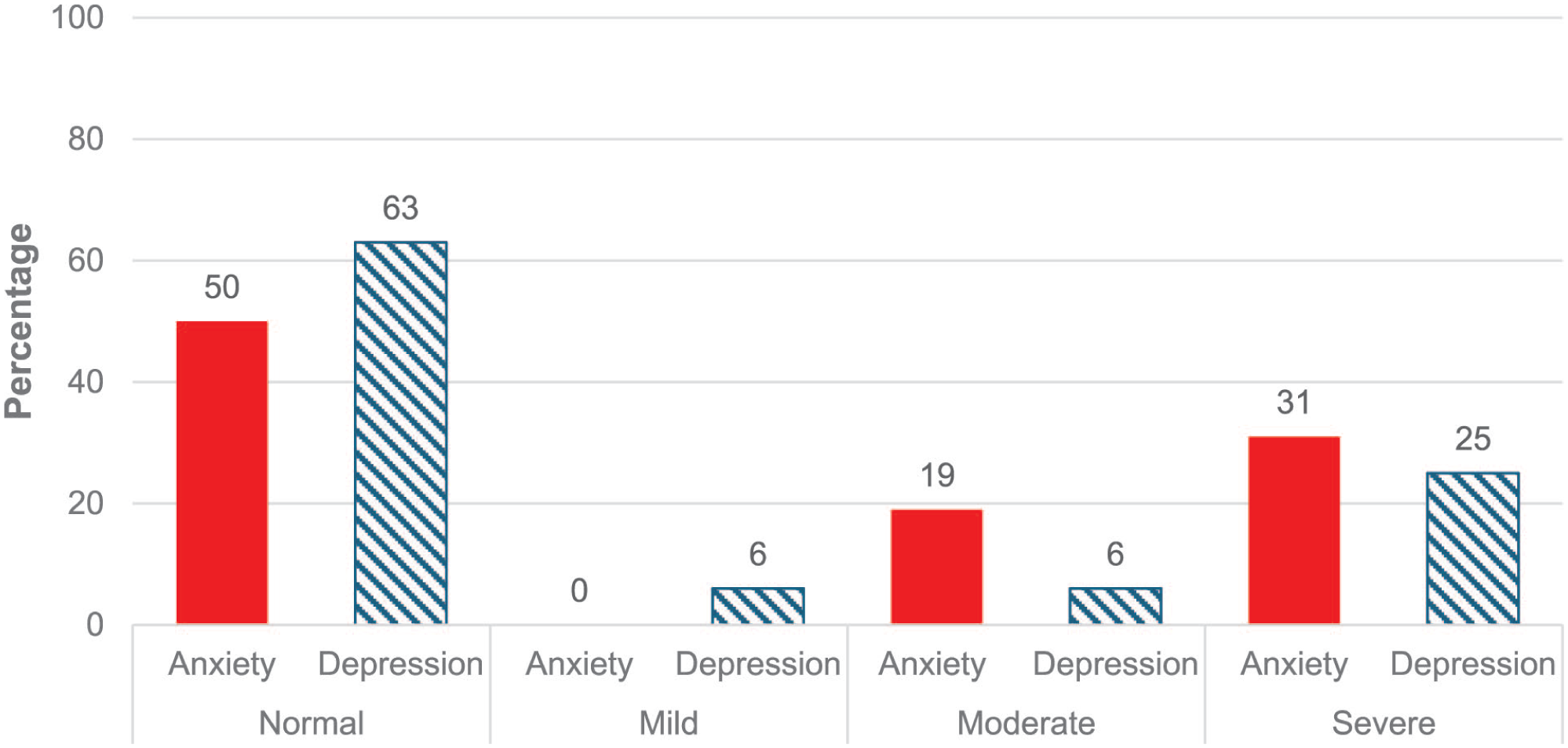
HADS scores at 6 week follow up.
At the time of the interview, seven out of eight patients were currently attending or on the waiting list for mental health support, with only one patient describing the psychological support that they had received locally as ‘helpful’.
Part 2: Thematic analysis of patient experience
As a result of analysis of the data from the patient interviews, three themes were identified: (i) Understanding of experience (ii) Difficult emotions (iii) Coping. Within these themes, nine subthemes were also identified (see Figure 2).
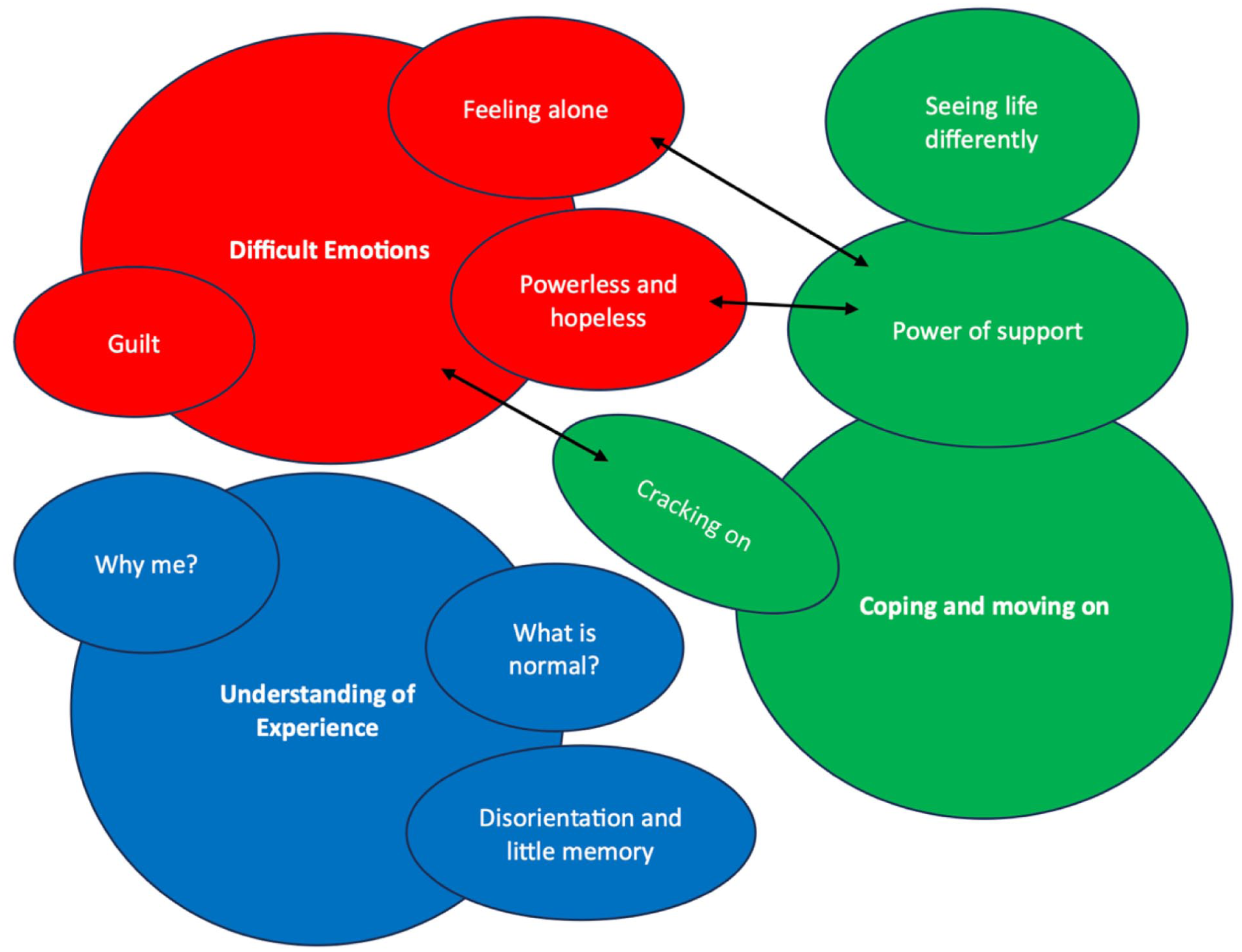
Diagrammatic map of themes and subthemes.
Understanding of experience
This theme described patients’ memories and thoughts about their ECMO experiences and the unanswered questions about this time. Three subthemes were identified.
Disorientation and little memory
All patients who participated in the interview described feelings of confusion and disorientation upon waking after ECMO. Patients had very little memory of the events leading up to ECMO, which contributed to feelings of fear and anxiety for many. Conversely, others found their little memory to be a protective factor.
The biggie is not knowing, because I wasn’t there consciously. . .and that’s the strange thing. I know it happened, but I wasn’t there. I don’t remember much about my admission at all. The team were just superb
Patients also described experiencing dreams whilst sedated on ECMO which added to the confusion about what was real and what was not. This was particularly difficult for those experiencing extremely vivid or distressing dreams.
Some patients were able to recall being woken after ECMO, with one patient describing dreams that his organs were being harvested and recalls resisting reintubation as a result of this.
Waking up with pipes and your throat open. It is the worst. Waking up to find my wife. . .it’s the best memory in the world. . .she woke me up and it was all sunny.
Patients described confusion and distress once awake, including some experiences of ICU delirium and distress related to the amount of time that they were sedated.
The realisation that I missed Christmas and New Years. I just threw up everywhere. I can still remember it so vividly. I just lost 4 weeks of my life.
Why me?
Three patients reported thoughts around why they had to be put on ECMO. Almost all patients had no significant history of medical or substance misuse problems and this contributed to feelings of frustration and comparisons to others.
I didn’t feel lucky to be alive, all I felt was why did this happen to me
Patients found it difficult to accept that there was no specific identifiable reason for why their bodies responded in that way to problems that others may have recovered from quite easily for example, infections. Patients commonly used language such as ‘unlucky’ and ‘by chance’ to describe their ECMO journey and the long-term impact that this had on them.
The only thing that does make me angry is that it was pure chance that I was there. The ‘why me’ hits me quite hard sometimes
What is normal?
Four patients described uncertainty about what a ‘normal’ recovery looks like once discharged from the hospital, both physically and psychologically. They recalled feelings of anxiety and panic at home, particularly due to the sudden loss of professional care.
There was no one checking on me. I thought I was losing the plot, I was crying every single day, and I couldn’t control my emotions. I was filled with fear every day for a year and a half Every day I thought I was dying
Worries about ‘going mad’ or being ‘abnormal’ often stopped patients from talking about how they were feeling emotionally.
You just saying that having those dreams is normal, that is so reassuring, those little things to know you’re not mad
As a result of this, patients highlighted the value of talking to people and the positive impact that reassurance can have.
I had no one to reassure me that what I was feeling was normal. When I did finally speak to someone, even though I don’t think it was to the extent that I needed it, it opened my eyes that a lot of these feelings are normal
Difficult emotions
This theme described the difficult emotions described by the patients, both during and after their admission. Three subthemes were identified.
Feeling powerless
Whilst admitted to the ICU, four patients reported feelings of powerlessness, largely in relation to a lack of control over their body. Many described vivid memories of being awake and not being able to move or speak, which was found to be one of the most difficult times post-ECMO.
It was so traumatising because I couldn’t move or say anything I was all over the place, I couldn’t control a thing about me. I couldn’t move my body, and I couldn’t control my brain
Patients described occasions where the medical team were discussing plans between themselves, without involving the patient. Patients reflected that even though they were unable to communicate verbally, it would have been helpful if they were still updated on their care.
The doctors would speak as if I wasn’t even there because they didn’t know that I was It was like I wasn’t being treated as a person, I was being treated as something they were trying to keep alive. I felt like a project rather than a person
Feeling alone
All patients recognised their ECMO journey to be extremely rare and unique, with most describing this to be a key contributing factor to their experiences of isolation. This continued at home where the limits to their physical health prevented them from re-engaging with their social network The whole nature of ECMO is that it is isolating isn’t it. . .and then I went home, and I was isolated
Patients also reflected on how their experience of ECMO felt vastly different to that of their family members. This contributed to feelings of emotional disconnect and beliefs that others did not understand what they went through.
Whenever we discuss it, we are talking about someone else’s experience not mine I feel alienated from my family, because they went through it together and I was isolated
Guilt
All patients described feelings of guilt for the psychological impact on family members and friends whilst they were on ECMO. They described worries about how their family coped during that time in addition to the long-term effects.
I still see that she is haunted by it when she looks at me All I could think of was that I did that to her
Many patients made comparisons with their own ECMO experience and highlighted how different this was for the family members, with many expressing beliefs that it was harder for their family than it was for them. Many expressed guilt and helplessness about not being able to help them.
I survived it, they went through it I feel almost that I was on the better end as opposed to them obviously, I would hate to imagine going through what they did.
Coping
This theme described the different ways that patients coped with the psychological impact of ECMO, both whilst trying to overcome current challenges and those they may encounter in the future. Three subthemes were identified.
Cracking on
During their recovery, patients described difficulties focussing on the psychological impact of ECMO and instead three patients found themselves prioritising their physical health, mostly because this was seen as the main barrier to discharge. This included consciously avoiding thoughts about their mental health as it was felt to be too painful at the time.
I was just so focused on getting back to work and trying to earn some money, so I just can’t deal with it [psychological therapy] . . . I just couldn’t face it I was so focused on getting physically better and my mobility, I didn’t really have the time to allow myself to deal with it emotionally at that time.
For most, ‘cracking on’ was seen as a helpful strategy to cope with the vast number of changes that they were experiencing at the time, as it allowed them to regain a level of control that they had not felt for some time.
Can you change it? No? Crack on then. What definitely got me through those first few months was you haven’t got time for this, what’s my other option
Others set themselves goals to focus on to help them to keep progressing with their physical recovery.
My priority was being mobile enough and walking so that I can be home to be able to welcome my daughter when she was home.
Seeing life differently
Six patients reflected on the psychological changes that they noticed post-ECMO, particularly in relation to how they cope with everyday life and how they view the world. Patients also described some negative feelings and behaviours about themselves that they wish they could change.
I do find it harder to be optimistic about things Now I’ve become the person that used to annoy me, someone who will sit and worry about something
Patients also described feelings of anxiety and uncertainty about the future and what this may look like, particularly regarding their health.
I’ve never had a health condition before, I’ve always been fit and healthy, so it hit me like a tonne of bricks that if it can happen to me, it can happen to anyone
In contrast, some patients were able to reflect on some positive changes post-ECMO. For example, they gained a new appreciation for life and increased motivation to enjoy their ‘second chance’.
My life 2.0. . .we are really trying hard to make it a life worth living
The power of support
The increased need for support post-ECMO was also identified during these interviews. Patients described varying levels of support that was offered from the team and highlighted the significant impact that not having this had on them. This included limited information about what had happened to them, and normalisation about what they were experiencing.
I had no one to talk things through with, and I think if I did, my mental health wouldn’t have been as bad as it was at that time
Those who did feel supported by the staff team, reflected on how beneficial this was. Support was offered by different team members and patients expressed a strong appreciation for this.
This nurse stayed by me. . .it was like having a little guardian there If it weren’t for her, I don’t know what would have happened to be honest [physio]
Family members were indicated to be the most valuable form of support for patients, providing reassurance and explanations about what was happening. Patients expressed feelings of sadness for those who did not have family with them and one patient described her gratitude for the reassurance she received from a family member of another patient whilst she was sedated on ECMO. She described being able to recall the women’s voice and found it reassuring to have someone looking out for her.
My heart breaks for people who don’t have a single person with them to speak to or explain things because without my mum I didn’t know This woman. . .her voice, her manner, it was just so reassuring. She was just telling me it was okay
Part 3: Pilot ECMO group
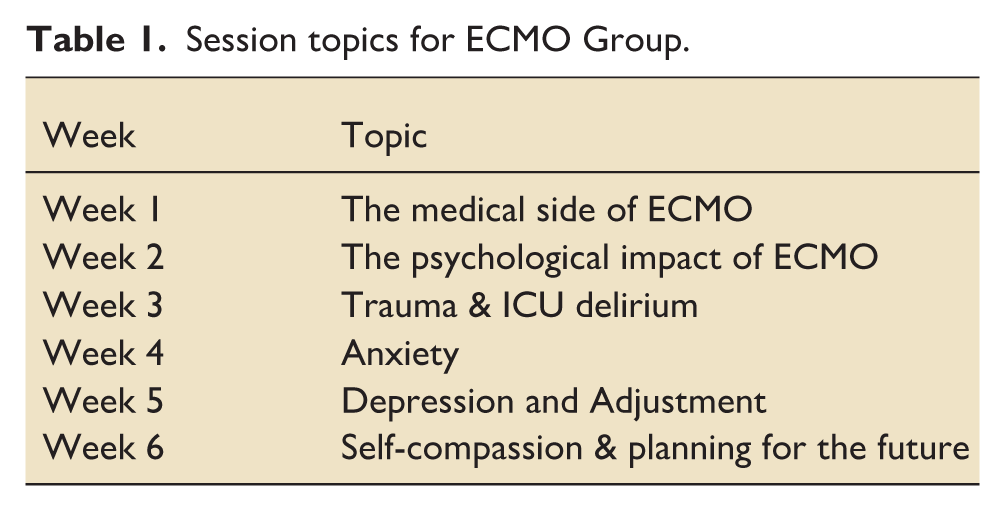
A pilot ECMO group was developed (see Table 1) in response to the themes identified in the existing literature and themes from patient interviews. The aim of this group was to explore whether an ECMO-specific psychological intervention would meet the needs of ECMO patients post-discharge. This was a 6-week online group that was offered to all 20 patients who had their ECMO follow up MDT in the last 2 years. The focus of this group was to create a space for patients to share their experiences and to normalise their feelings, which was highlighted as a key theme throughout the interviews.
Session topics for ECMO Group.
Qualitative feedback – Benefits of attending the ECMO group
Patients described the group to be a place where they could relate to others, in contrast to the ‘barriers’ that were felt when talking to family members. The value of hearing the experiences of others were highlighted, in addition to the power of peer reassurance that they were ‘on the right track’ in their recovery.
The qualitative feedback suggested that the group was effective in addressing most of the problem themes they had described in their initial interviews:
Patients described having a better understanding of their experience and reported feeling hopeful now and validated by talking in the group.
I’m not the only one, I can get through it and take my time, there is no rush
Patients also reported feeling more connected with other ECMO survivors.
I feel seen and heard You have kinship like the way only brothers look at each other
Patients reported no longer just ‘cracking on’, as they were allowing themselves time to process and understand their ECMO experience: It’s given me the structure to think about things that I don’t usually, so I put time aside for it
Patients reported seeing life differently, experiencing post-traumatic growth as an ECMO survivor: It’s made me re-evaluate everything. I am grateful and I look at myself with more compassion: Helped me to cut out people who were never there for me. . . at least you know who would be there at your funeral More grace towards myself, made me stronger, I pushed through when my life was in jeopardy
However, patients reported still feeling angry and wanting better recognition and funding for ECMO.
ECMO is unseen, a hidden realm- like a hidden disability People who have it either die or hide their scars under their t-shirt; cancer is a lot more celebrated than hidden
Patient recommendations
Patients suggested a range of improvements to ECMO services to help them to understand and cope better with their experience
(1) Better information to help with understanding experience
A summary of care by the lead consultant before you leave to help you process what has happened
(2) Importance of psychological support after ECMO
I hope that other people could get this support like I have (ECMO group), it has been amazing
(3) Trauma-informed care on ICU
Support with communication- give patients a voice as soon as possible to reduce frustration e.g. (yes/no) Explain things to us, even if you think we can’t hear you Please close the curtains when asked as when delirious it looks so strange
(4) Better funding for ECMO
ECMO has such a low profile but is a vitally extreme treatment, hope there is the ability to give more money to ECMO, raise the profile of what it gives people like us e.g support group like Macmillan give cancer patients,
Outcome measures
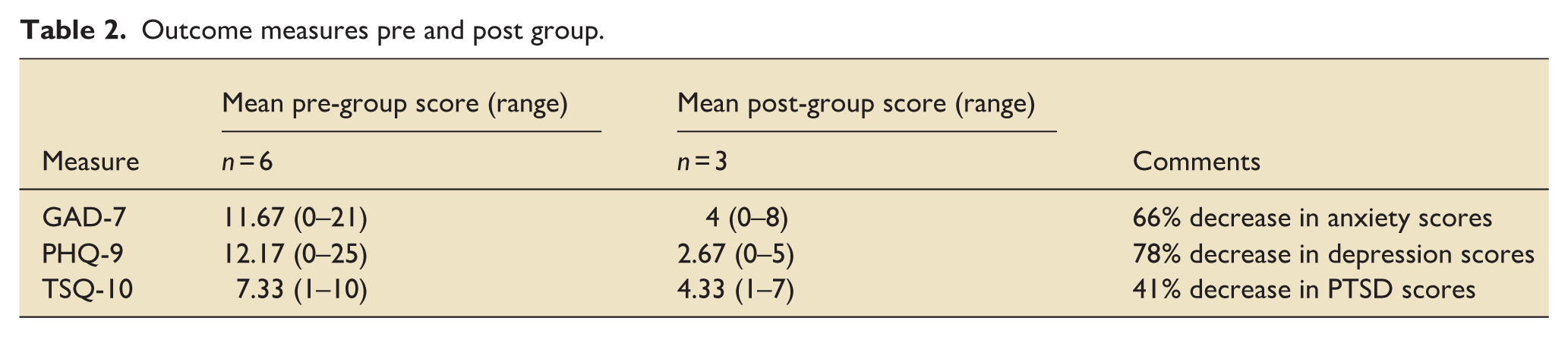
Outcome measures were completed before and after completion of the group. These measures included the Generalised Anxiety Scale (GAD-7 14 ), the Patient Health Questionnaire (PHQ-9 15 ), and the Trauma screening Questionnaire (TSQ-10 16 ).
The outcome measures showed an overall decrease in mean anxiety, depression and PTSD scores after completion of the group (see Table 2). For both anxiety and depression, no patients scored within the ‘moderate’ or ‘severe’ range post-group. Patients indicated to be at risk of PTSD on the TSQ-10 also reduced by 41%.
Outcome measures pre and post group.
Discussion
This project found a high prevalence of anxiety and depression in ECMO patients, similar to the levels found in other critical care populations. 5 This was explored in further detail in the patient described themes, with some findings consistent with previous qualitative studies, for example, struggling to understanding ICU delirium and fragmented memories. 9 However, several new themes emerged, with patients struggling to understand ‘what is normal’ in reaction to their critical care experience. Previously unidentified themes around experiences of powerlessness and isolation were also highlighted. The patient-described problem themes formed the basis of the ECMO 6-week group, and the post-group feedback highlighted that this psychological intervention successfully met those needs. For example, feeling kinship replaced feelings of isolation and loneliness and understanding the context of ECMO replaced their earlier struggles to understand their experiences.
Trauma appears to be an overarching theme for this project, and patients identified factors that could either exacerbate or protect them against risk for post-traumatic stress, depending upon the level of psychological support available.
Post-Traumatic Stress can develop when rumination on a critical care experience leads to negative interpretation and predictions about the future. In this project, patients reported worrying about their health and feeling they had no control over when it might happen again. However, post-group feedback suggested that patients also experienced positive change associated with having coped with their ECMO experience, in relation to how they see themselves, the profound impact on their relationships and a new perspective on life.
A recent conceptual review offers advice on facilitating post-traumatic growth after critical illness, 17 explaining that continuously ruminating on the trauma is an attempt to understand and incorporate this into their worldview. Supporting patients to revisit and process the trauma in a planned way can help them find new meaning and positive reappraisal of their personal strengths. This project provides evidence of post-traumatic growth in ECMO survivors when offered appropriate psychological support to understand and process their trauma.
Patients offered recommendations for psychologically informed improvement to ECMO services, but they were aware of limited funding being available. There was a strong sense of perceived injustice that ECMO services were not as well funded as cancer services. Indeed, patients expressed a sense of shame at being an ECMO survivor ‘we die or hide our scars under a t-shirt’ but cancer patients are well supported to be proud of their survival. Providing better funding for ECMO services would include greater psychological support to reduce that burden of shame.
Strengths and limitations
This mixed-methods service development project had significant limitations. It was a single centre project with a small sample size and therefore, the findings may not be generalisable to other settings or patient groups. Future research could increase the sample sizes across multiple centres. Furthermore, the piloted intervention within this study was a brief 6-week group intervention with a small number of patients, and therefore future research could also explore the impact of psychological support for a larger sample of patients to further evidence the benefits.
Conclusion
This project found evidence of the unmet psychological needs of ECMO patients, and the benefits reported from the pilot ECMO group suggests that appropriate psychological intervention could support post-traumatic growth. Such trauma-informed pathways would include dedicated psychologists for direct and indirect intervention in critical care and supporting others to work in psychologically informed ways. Thus, implementing Intensive Care Society/ Faculty for Intensive Care Medicine 10 minimum standards could minimise the psychological burden of ECMO and support post-traumatic growth for patients, families and potentially also for critical care staff.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.