
Abstract
A 30-year-old woman presented at 19 weeks of gestation with symptoms of sore throat, rhinorrhea and haemoptysis that progressed to massive haemoptysis. Her medical history included asthma and a history of smoking prior to pregnancy. Investigations revealed no obvious cause of bleeding. Right lower lobe lobectomy was performed, given the suspicion of a lesion within the intermediate bronchus. The patient developed adult respiratory distress syndrome around 36 h postoperatively. Polymerase chain reaction testing on bronchoalveolar lavage samples was positive for influenza A. Therapy with oseltamivir was initiated. She was discharged two weeks later. This is a rare case of a severe complication from seasonal interpandemic influenza during pregnancy, which underscores the importance of immunization for pregnant women.
Introduction
Pregnancy has been linked to worse prognoses during influenza pandemics. Literature from the 2009 H1N1 influenza pandemic reported few cases of haemoptysis as a presenting symptom. 1,2 We present a rare case of severe haemoptysis in a pregnant woman, possibly due to influenza.
Case presentation
A 30-year-old woman with a 10 pack-years smoking history and asthma consulted at 14-weeks’ gestation for haemoptysis. She had no personal or familial history of arteriovenous malformation or bleeding diathesis. She had no fever, chills, myalgia, chest pain or epistaxis. She had been using her bronchodilator daily since the beginning of the pregnancy due to increased dyspnoea. Her vital signs remained stable except for mild tachycardia, with no recurrence of haemoptysis. Blood work yielded normal coagulation, renal and hepatic function. Initial haemoglobin level was 111 g/L. Chest X-rays showed a small infiltrate in the right middle lobe, which had almost disappeared on repeat films the next day. A ventilation-perfusion scan was negative. Foetal echocardiography was normal. No definite source of bleeding was found, and she was discharged on inhaled fluticasone and standard follow-up with her obstetrician.
She consulted again at 19-weeks’ gestation for recurrence of haemoptysis. Despite initial improvement after discharge, five days before this admission she developed a sore throat, rhinorrhoea, and coloured sputum. She had no fever, chills, myalgia, or headache. She had coughed around 100 mL of blood. History was negative for symptoms of thromboembolic disease, gastrointestinal symptoms, tuberculosis risk factors, and symptoms of connective tissue disease. Influenza vaccination status was not noted.
On physical examination, O2 saturation of 80% was noted which normalized with supplemental oxygen. Crackles were heard in the right inferior lung. Haemoglobin level was 101 g/L. Her blood work-up was normal. Chest X-rays showed an alveolar infiltrate in the right lower lobe. An echocardiogram showed normal cardiac function.
A bronchoscopy showed an organized lesion within the intermediate bronchus that obstructed 80% of the lumen. Coagulated blood and oozing could be seen behind the lesion. She was immediately transferred to a tertiary centre for possible endobronchial intervention and/or angioembolization.
Upon arrival at the tertiary centre the patient had stable vital signs, with O2 saturation of 96% on room air. Her haemoglobin concentration had dropped to 85 g/L. She underwent another bronchoscopy during which blood was continuously aspirated and no lesion could be detected. Her O2 saturation dropped during the procedure and endotracheal intubation became necessary. She was sent for urgent rigid bronchoscopy which revealed bleeding from the right lower lobe, but no endobronchial lesion was seen.
A CT pulmonary angiogram was ordered (Figure 1) which showed no arteriovenous malformation and no pulmonary emboli. Even though the right bronchial artery was deemed adequate for embolization, a decision was made to perform right lower lobectomy because the initial bronchoscopy suggested the possibility of bleeding from an endobronchial lesion.
CT scan showing right lower lobe consolidation probably due to bleeding.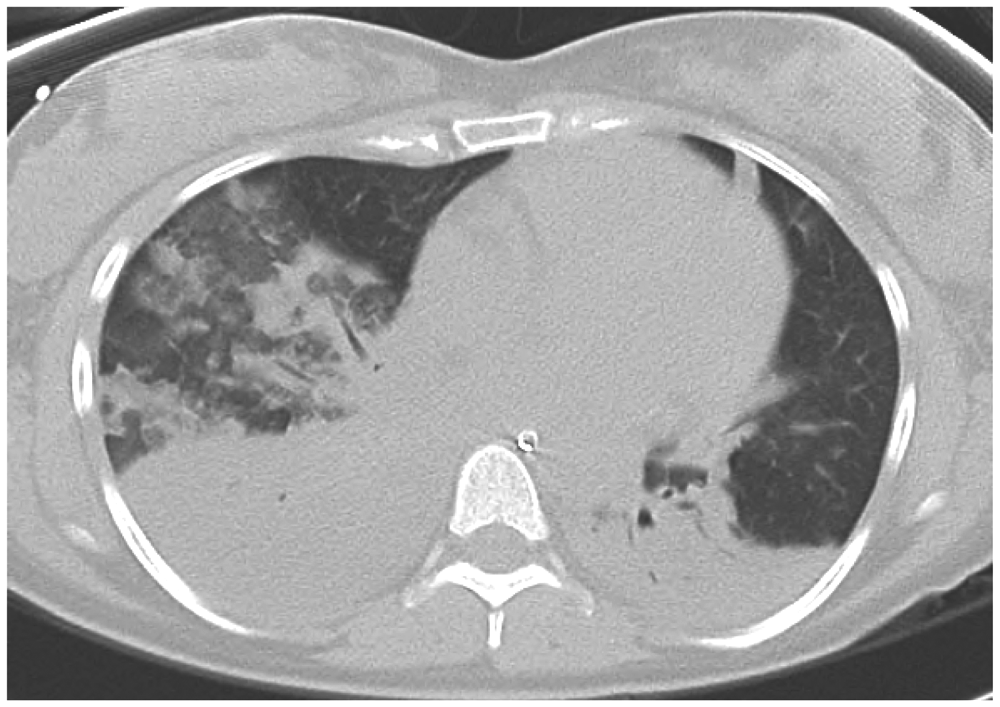
There were no intraoperative complications and the patient was extubated after less than 24 h. Thirty-six hours after surgery she developed respiratory distress and bilateral pulmonary infiltrates. Her condition worsened and necessitated re-intubation and high-frequency oscillatory ventilation. Bronchoscopy revealed no bleeding from the airway or alveoli, but polymerase chain reaction (PCR) testing from bronchoalveolar lavage was positive for influenza A. Treatment with oseltamivir was started. The patient’s condition gradually improved, and she was discharged two weeks later.
Histopathological analysis of the surgical specimen yielded fresh bronchocentric bleeding, respiratory bronchiolitis, and elements of chronic and acute airway inflammation possibly from infection. There were no signs of malignancy, vasculitis or capillaritis. The lesion within the intermediate bronchus was determined to be a thrombus. Cultures from one of the specimens yielded Mycobacterium gordonae, which was considered to be a contaminant since it is ubiquitous in tap water and soil and since no granuloma were found.
The rest of her pregnancy was complicated with late mild preeclampsia and she was induced at 40 weeks, delivering a healthy 3750 g baby boy.
Discussion
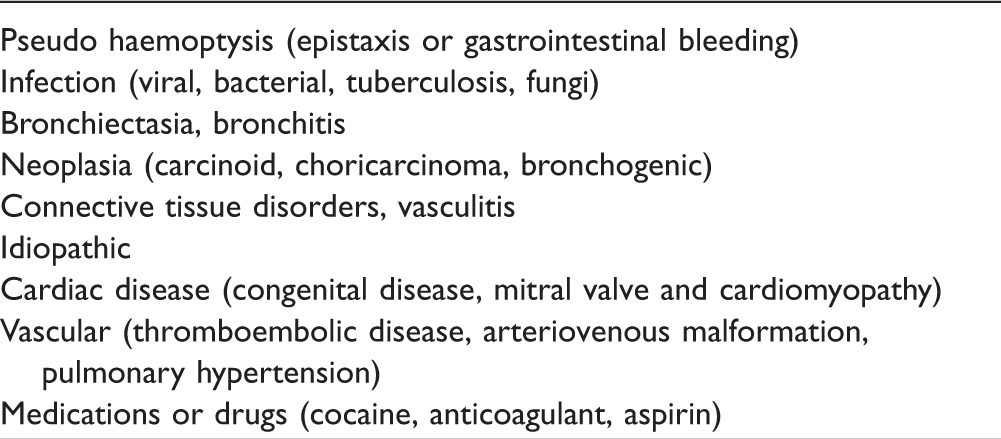
Etiology of haemoptysis in pregnancy.
Idiopathic haemoptysis related to pregnancy has also been suggested as a distinct entity by some authors. Hormonal changes during pregnancy might increase the risk of haemoptysis by encouraging angiogenesis and increasing cardiac output. 3 These factors may have played a role in the initial presentation of our patient.
Influenza and pregnancy
Historically, mortality and morbidity appeared to be disproportionately increased among pregnant women during influenza pandemics, 4,5 probably due to changes in their immune systems. Even in non-pandemic influenza seasons, pregnant women tend to have a higher rate of hospitalization from respiratory illness. 6,7 Data from the 2009 H1N1 influenza pandemic seems to confirm worse prognoses for infected pregnant women. Although pregnant women make up less than 1% of the population in the United States, during the 2009 pandemic up to 10% of hospitalized patients were pregnant and accounted for 5% of the mortality. 1,2,8 –12 Markers of worst prognosis include: (1) young age, (2) underlying conditions including asthma, obesity or diabetes, (3) illness onset in the second or third trimester and (4) initiation of antiviral treatment beyond four days after disease onset. 1,2,8 –12 It is noteworthy that our patient presented at the end of her first trimester with badly controlled asthma, and started receiving oseltamivir around five days after symptom onset.
Haemoptysis and influenza
Few reports from the influenza A H1N1 pandemic described haemoptysis and diffuse alveolar haemorrhage as symptoms, and no clinical or bronchoscopic descriptions were provided. 13 –15 Gilbert et al. 16 described a case of diffuse alveolar haemorrhage confirmed by bronchoscopy in a 57-year-old African American woman who also presented cardinal symptoms of influenza.
Pathological studies have described changes seen in severe, influenza viral pneumonia. 17 Hemorrhagic tracheitis and bronchitis have been reported, 18 with zones of oedema, haemorrhage, or necrosis in the upper respiratory tract on the internal surface of the larynx and trachea. 19 Our patient did not present changes characteristic of primary influenza viral pneumonia initially; however, her deterioration to adult respiratory distress syndrome (ARDS) after extubation could have been a manifestation of viral pneumonia.
Conclusion
This is a rare case of a severe complication from seasonal interpandemic influenza in a pregnant woman. It stresses the importance of immunization for pregnant women, particularly those with additional risk factors such as smoking or asthma. Hormonal and physiological changes due to pregnancy may have contributed to the clinical manifestations of this patient. In retrospect, lobectomy could have been averted through angioembolization, but the possibility of an endobronchial lesion being the source of bleeding weighed heavily in the decision-making process.