
Abstract
Background
A published audit demonstrated that a pilot psychiatric clinic failed to capture predicted numbers of women with severe and enduring mental illness.
Methods
On the basis of recommendations from this audit, along with those from the Royal College of Psychiatrists and NICE guidelines, a more comprehensive psychiatric service was developed to meet this demand and therefore manage risk more effectively.
Results
Over the course of a year, the new service attracted a higher rate of referrals of pregnant women with severe and enduring mental illness. The majority referral source continued to be midwifery-led.
Conclusions
Audit is a useful tool for evaluating and informing service development and helped us identify further improvements needed to deliver an effective mental health service.
Introduction
Psychiatric disorders are one of the leading causes of maternal mortality during the perinatal period. 1 –4 Development or relapse of maternal mental illness can therefore have severe consequences for mother, baby and family. Psychotropic drug use must be justified by predictable benefits that outweigh the teratogenic and obstetric risks to the unborn baby. Doses may need to be adjusted because of pregnancy-associated altered pharmacokinetics and treatment plans may need to be revised to minimise withdrawal syndromes and incorporate plans for breastfeeding.
Perinatal mental health provision presents a complex set of challenges, with need for integrated management, particularly between maternity, psychiatry and primary care services. 5 Treating women in the perinatal period involves specialist understanding of the presentation and consequences of severe mental illness at this time. Postpartum psychosis has a distinct psychopathology often with more sudden onset and greater severity than other psychotic illnesses. There is often the opportunity to identify patients at risk antenatally and refer to perinatal mental health services, where these exist. Patients require multiagency care planning including attention to child safeguarding issues. Personality disorder can impact parenting, necessitating the involvement of perinatal mental health services in child protection and care proceedings. National policy initiatives emphasise the requirement for maternity services in every community to deliver an effective perinatal mental health strategy. 1,2,6,7 However, recent restructuring of UK mental health services has resulted in many patients, who would formerly have been cared for within Community Mental Health Teams (CMHTs), being discharged back to primary care where general practitioners (GPs) may lack confidence or experience to manage severe mental illness in the puerperium.
Background
In 2003–2004, a perinatal mental health clinic was set up in response to national guidelines and the unfortunate occurrence of two local maternal deaths secondary to mental illness. The aims of the clinic were to identify and treat severe mental illness in women receiving antenatal care at the Whittington Hospital, in North London. This was an unfunded pilot model, comprising one special interest session per week from a dedicated specialist registrar (SpR) working from within the hospital’s Mental Health Liaison Team (MHLT). The service accepted referrals from the antenatal clinic only, and provided capacity for a once-weekly outpatient clinic for two new referrals and three follow-ups. An audit of the year’s activity showed that 75 referrals to the service were made of which 19% met eligibility criteria for onward referral to secondary mental health services. Of the 57 patients assessed, 39% had no mental illness, thus identifying the need for a more robust service and training of referrers, especially maternity staff. 8
Since February 2010, a more comprehensive service has been instituted, funded by Islington Primary Care Trust and functioning from within Camden and Islington NHS Foundation Trust. Based on the guidance from NICE 7 and the Royal College of Psychiatrists, 1 the current Perinatal Mental Health Team provides a multidisciplinary mental health service for adult pregnant and postnatal women with severe and complex mental illness who are receiving maternity services from the Whittington Hospital. One of the authors (NS), who was involved with the pilot model, currently leads the team as consultant perinatal psychiatrist (0.5 whole-time equivalent (WTE)). The small team provides a service for approximately 4000 births per year and comprises a specialty grade psychiatrist (0.5 WTE), one full-time perinatal clinical specialist nurse (Band 6) and 0.5 WTE administrative support. It should be noted that an ideal multidisciplinary perinatal mental health team would also include psychology, social work and occupational therapy input, as well as access to specialist in-patient beds in a Mother and Baby Unit.
Emphasis is placed on working collaboratively with women and their families to plan care for pregnancy and the early postpartum period, functioning in partnership with maternity services, psychology, Children and Family Social Services, primary care services and other relevant agencies. The team operates from Monday to Friday, 9 a.m to 5 p.m. Outside working hours, cover is provided by emergency services including the MHLT a team providing psychiatric input for all patients under the care of the acute trust, i.e. all medical and surgical patients. Referrals of pregnant women having their maternity care at the Whittington Hospital or up to six months postnatally are accepted from any professional within the maternity service, from mental health services and from primary care. Referrals are made using an easily accessible referral form and triaged at a weekly meeting using the eligibility criteria for the service. Clinicians deliver regular midwifery and obstetric training sessions to improve the quality of referrals and also participate in multidisciplinary meetings with obstetricians, paediatricians and social workers. There are no dedicated Mother and Baby Unit beds but the service facilitates transfer of patients to local in-patient units when necessary.
In keeping with mental health trust policy, under 18s or women with primary diagnoses of alcohol or drug dependence are triaged directly to specialty services (and to the hospital Children and Family Social Services department). Assessment by a member of our team is offered to all out-of-borough women who are then referred on to local mental health services. Ongoing review and care planning is offered to Islington residents only, though women receiving maternity care at the Whittington Hospital receive birth plans and reviews as appropriate, and demands are often made of our team to remedy deficiencies in out-of-borough services.
Islington secondary mental health teams vary in their capacity to work jointly with perinatal mental health services and some women are transferred to us for sole care and risk management until they are discharged at six months postpartum to either primary or secondary mental health care. During the ante and postnatal period, Islington residents are eligible for domiciliary visits if there is difficulty travelling to appointments. These are mainly conducted by the specialist nurse or sometimes by a doctor, with due attention paid to risk, and joint visits with midwifery or other staff facilitated when appropriate.
Where engagement is problematic and high-risk women fail to attend appointments, communication and liaison with other relevant services is undertaken, and children and family social services alerted when necessary. Midwives can often assist in engagement if women are reluctant to meet with mental health professionals.
Women with mild to moderate non-psychotic illnesses can be referred directly to women’s health psychology which operates an opt-in system. With non-pregnancy-related difficulties, there is a direct referral pathway to the Improving Access to Psychological Therapies (IAPT) programme, to which patients can also self-refer.
Collaboration with social services is a central part of the work of any perinatal mental health team. Child protection and safeguarding procedures add significantly to the workload of the team and reflect the complexity of the issues presented by many patients.
The aim of this study was to look at the operation of the current service in light of the shortcomings of its predecessor pilot model.
Methods
Referrals to the service during a one-year period from 1 April 2010 to 31 March 2011 were identified. Patient information was collated from paper referral forms and electronic patient records (RiO), which also uploads clinic letters. Data collection included: socio-demographic data; origin of referral; gestational age at referral; referral outcome; diagnosis (if subsequently assessed); information on drug and alcohol use; and any history of domestic violence.
Results
A total of 315 new patient referrals were received, with a mean age of 31.2 years (range 17–48 years). One hundred and seventeen (37.1%) were White British, 42 (13.3%) were from Black or Asian minority ethnic groups, 54 (17.1%) were from other ethnic backgrounds and in 102 cases (32.4%) patient ethnicity was not recorded. One hundred and twenty eight referrals (40.6%) were for patients in the mental health trust catchment area of Islington, with a slightly higher number (n = 141; 44.8%) from the neighbouring borough of Haringey. The remaining 46 patients (14.6%) were from other London boroughs.
The mean gestational age at referral was 17.4 weeks (range 5–39 weeks). Twenty eight referrals (8.9%) were made postnatally (mean 18 days; range 1–98 days) and 11 of these referrals were for women on the postnatal ward who had recently given birth. There was one referral for preconception counselling.
The majority of referrals were made by midwives (n = 229, 72.7%), with obstetricians referring 33 (10.5%) cases. The remaining sources of referral (n = 25; 7.9%) were from a variety of disciplines including psychiatrists in CMHTs, GPs, psychologists, social workers, occupational therapists, paediatricians and neonatologists. In 28 cases (8.9%) the designation of the referrer was unknown.
Fifty seven women (18.1%) had a history of alcohol use, 12 of whom (3.8%) admitted to current alcohol use in pregnancy. In 24 cases (7.6%) there was a history of domestic violence. The mean time from referral to appointment was 24 days (range 0–111 days).
Figure 1 summarises the referral outcomes: 53 patients (16.8%) were seen for one assessment; 65 (20.6%) were assessed and subsequently received follow-up care throughout pregnancy and the postnatal period if necessary; 49 (15.6%) defaulted from all appointments; 67 referrals (21.3%) were triaged straight to psychology services; and 81 referrals (25.7%) were referred back to primary care.
Outcomes of referrals.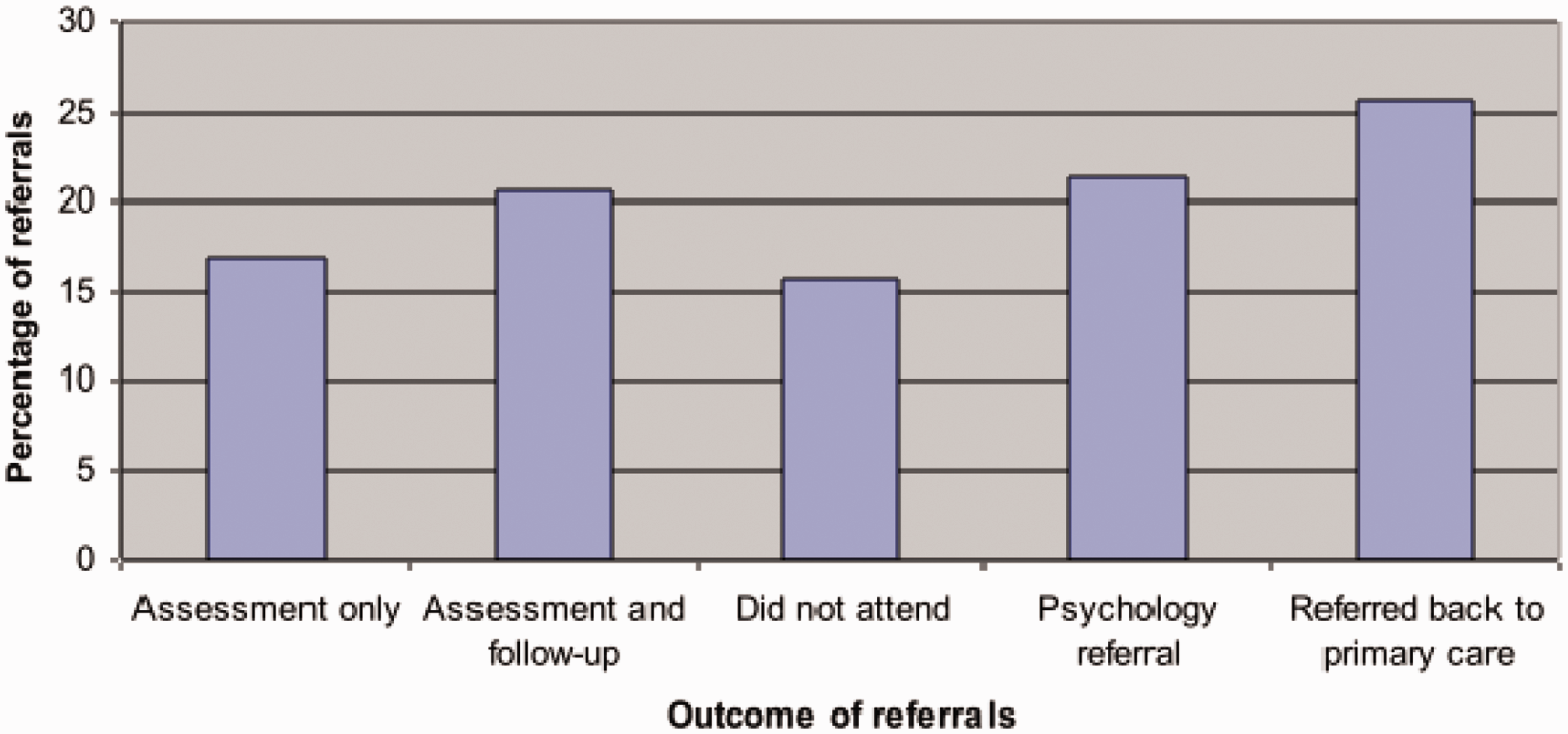
The majority of women were seen as outpatients in the hospital’s antenatal department, although the clinical specialist nurse also holds clinics at the local Women’s Crisis Centre. Urgent postnatal reviews were undertaken on the maternity inpatient ward, with the hospital MHLT providing cover when no team member was available. Nine domiciliary visits were carried out.
Of the 81 patients referred directly to primary care, 56 (69.1%) were considered not to be unwell based on the clinical information on the referral form, 21 (26%) were already under the care of appropriate specialty services, and in four cases (4.9%) the patient subsequently moved out of area. There were only three patients who were subsequently re-referred.
Primary diagnoses (ICD-10).
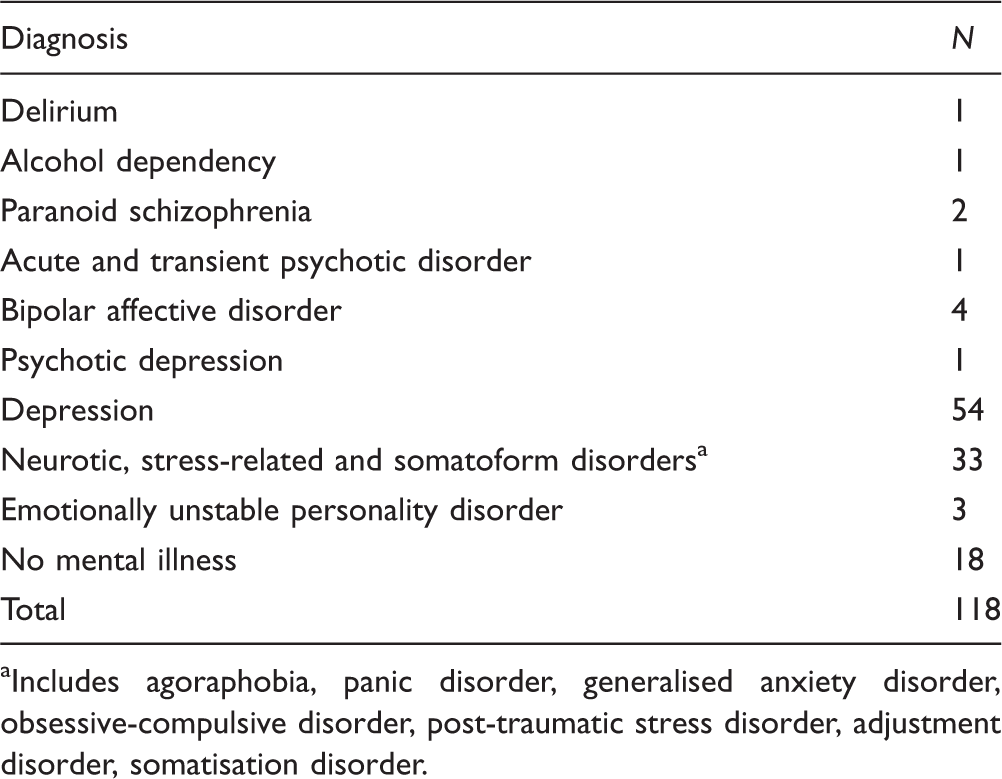
Includes agoraphobia, panic disorder, generalised anxiety disorder, obsessive-compulsive disorder, post-traumatic stress disorder, adjustment disorder, somatisation disorder.
Comparison with pilot study
As expected, the new perinatal service has received a higher number of referrals (n = 315) than the pilot service (n = 75). Whereas previously women from Islington comprised the majority of referrals (55%), we are now being referred a higher proportion of women from outside the borough (59.4%) and the mean age of referral has increased slightly (29.7 years (range 17–43 years) versus 31.2 years (17–48 years)), which is in keeping with the increasing national mean average age at first childbirth. 4 The pilot service only accepted referrals from midwives and obstetricians. The new service accepts referrals from more multidisciplinary sources although the vast majority are still maternity-driven.
The limited capacity of the pilot service providing one session of SpR time per week meant all women who required secondary care were referred on to local CMHTs, which occurred in 19% of referrals. Women from Islington requiring ongoing follow-up and care are now taken on to the team’s caseload and represent a similar proportion (20.6%) of the total number of referrals. Comparing rates of diagnoses, depression remains the most frequent diagnosis (30% and 46% of the women seen in the pilot and new service, respectively).
In the original study there was only one case of a patient referred with a severe and enduring mental illness (bipolar affective disorder) out of a total of 57 patients seen (1.8%). Capture rates in the new service compare more favourably, with 8 out of 118 women seen (6.8%) having diagnoses of severe and enduring mental illnesses. There has been an increase in the proportion of referrals triaged directly to psychology services from 14.7% to 21.3%. Finally, there has been a large and important reduction in the proportion of women in the pilot study who were not found to have any mental illness from 39% to 15%. These results suggest an improvement in quality of referrals.
Discussion
This service, in common with all perinatal mental health services, was set up to identify and manage maternal mental illness, thus improving obstetric care and reducing risk. It was shaped in accordance with national guidelines and also has benefitted from lessons learned by audit, as its predecessor model failed to identify appropriate patients. 8 Embedding the service and gaining recognition amongst well-established maternity services has been a progressive task but the small team performs well to meet the clinical needs of its patients and other allied health care professionals, whilst at the same time monitoring its own progress, successes and shortcomings.
The service has inbuilt systems to formalise necessary interfaces. The numbers and quality of referrals have increased and we are now identifying a higher proportion of pregnant women with severe and enduring mental illness. Fifty three per cent of women referred are offered appointments and a further 21% are correctly identified as requiring psychological intervention. On average routine referrals are being seen within four weeks.
Routine UK antenatal care involves first contact with a midwife for a booking appointment by 12+6 weeks gestation, yet the mean age of gestation at referral was over 17 weeks. This raises the issue of whether use of the Whooley prediction questions (regarding past or current psychiatric illness and treatment or family history) or detection questions (‘During the past month, have you been bothered by feeling down, depressed or hopeless?’; ‘During the past month, have you often been bothered by little interest or pleasure in doing things?’), as recommended by NICE 7 for use by healthcare professionals, are an effective screening method at booking.
The service is currently receiving more out-of-borough referrals than patients from Islington. Local funding agreements mean the service is restricted for a significant proportion of women, often with lengthy referral processes to appropriate out-of-borough services. In reality, many of these women are, out of necessity, actually managed predominantly by the hospital team (MHLT), as per all general liaison psychiatry services, but accessing funding from local commissioners will be vital in order to continue to meet this increasing demand.
The next logical step to improve service provision is to secure funding from future Clinical Commissioning Groups, enabling all women, irrespective of their place of residence, to receive timely, equitable and high-quality antenatal and postnatal care. The establishment of Mental Health Payment by Results 9 will challenge us to ensure that the diversity of our work is reflected accurately. Development of meaningful outcome measures is a current challenge being addressed nationally. Centralised funding of mother and baby unit beds will eliminate arbitrary patient postcode division and may provide a model for maternity service commissioning to be aligned to mental health services in the community too.
Other essential considerations include the provision of adequate administrative support which is key. Efficient communication underpins robust multiagency interfacing for effective and safe patient care. In addition, the role of the clinical nurse specialist is evolving and now includes care co-ordinating a group of local vulnerable women, with outreach clinics for assessment, triage and follow-up as well as smoking cessation advice.
An audit by the Maternity and Perinatal Partnerships in Mental Health (MAPPIM) Team, 10 a perinatal mental health service at St Thomas’ Hospital, London, which functions as part of the acute trust maternity service with an annual delivery rate of approximately 6000 at the time of data collection, identified a cohort of 45 women with a history of psychosis or at risk of postpartum psychosis who were referred to the service during its first two years between November 2002 and November 2004, representing 6.7% of total referrals. The eight high-risk patients identified in this audit represent only 2.5% of the total number of referrals (though 6.8% of the women seen). It was noted in the MAPPIM study that during the fourth year of the service the number of women with psychotic illness doubled, which may have represented under-referral of some women already in contact with mental health services during the first two years.
A further MAPPIM audit in 2007–2008 (L. Green, personal communication) demonstrated that 38% of women offered assessments were under a CMHT at referral, compared to less than 8% of our women. Based on published prevalence rates, 11 it is estimated that there would be approximately 20 women with psychotic illness within our maternity service, which is more than double the number of women identified from this re-audit.
There are plans therefore to liaise more closely with consultant psychiatrists from all local areas in order to increase the identification of pregnant women with serious mental illness and we will continue to raise the profile of our service in order to attract referrals from multidisciplinary sources. Resource issues currently limit the capacity of such a small team to provide training to GPs and mental health teams in addition to that delivered to midwives, though the referral of only one woman for preconception advice in this audit highlights the need for such education. The high proportion of midwifery referrals underlines the importance of local midwifery training and has been reinforced by our frequent training sessions, which are tailored to midwives’ specified learning objectives and well evaluated.
UK perinatal mental health services represent a heterogeneous group in terms of demographic, financial and operational characteristics, which means generalisations from other models, is problematic. This highlights the importance of collecting more local evidence to improve a service such as ours, and of carrying out frequent audits such as this, which help better inform optimal perinatal mental health service development. This audit has revealed that the establishment of our new perinatal team has gone a long way towards meeting the mental health needs of women under the care of maternity services where a pilot model failed, but that there are aspects of service provision still to be addressed. Not only has the audit cycle been completed, but it will continue, as it should, when we re-audit in two years’ time in the light of these findings.
Footnotes
Author contributions
All authors contributed to data collection and reviewing of submissions.
Acknowledgements
The authors thank the reviewers for helpful comments and Lucinda Green for provision of comparative data.