
Abstract
Background:
Postpartum screening for diabetes in women with gestational diabetes (GDM) improves with use of reminder systems. Our primary objective was to identify predictors of diabetes screening in the first year after delivery.
Methods:
A retrospective study was performed of 556 women with GDM who received outpatient prenatal care between 2007 and 2009. A mailed reminder system was utilized at two sites. Rates of postpartum glucose testing at 6 and 12 months postpartum were measured.
Results:
Site of care and non-smoking status were identified as the only predictors of postpartum diabetes screening (p<0.001 and p = 0.02, respectively). Rates of OGTT completion at one year (38% vs. 19% p<0.001) were higher in women who attended clinics with postpartum reminders.
Conclusions:
The site of diabetes care in pregnancy is a major predictor of adherence to diabetes screening postpartum. Health care delivery should be considered in the development of strategies to increase screening rates.
Keywords
Introduction
Gestational diabetes (GDM) impacts approximately 2–10% of all pregnancies 1 and confers a 7-fold increased life-time risk of type 2 diabetes. 2 Current practice guidelines by the Canadian Diabetes Association recommend screening for type 2 diabetes with a 75 g oral glucose tolerance test (OGTT) between 6 weeks and 6 months postpartum, along with counselling for healthy lifestyle behaviours for all women with a diagnosis of GDM. 3 The American Diabetes Association guidelines are similar, but differ in that screening is advised between 6 and 12 weeks postpartum. 4
Despite increased awareness of the risk of future type 2 diabetes following a pregnancy affected by GDM, screening rates postpartum remain sub-optimal. A recent systematic review of 11 studies, involving a total of 32, 240 women, reported a median rate of any glucose assessment postpartum of 48%. 5 Our group, using a focused survey at a large tertiary care centre, identified that the most common reason primary care providers (PCPs) gave for not screening was no postpartum visit from the patient – for any reason. 6 Time pressures associated with caring for a newborn, especially if breast-feeding, were the most common reasons provided by patients for not completing a glucose screening test. Counselling GDM patients during pregnancy of their risk of future type 2 diabetes is imperative to improve diabetes screening rates.7,8 Several studies to date have shown that use of an automatic reminder system improves postpartum diabetes screening rates.9–15
Identification of clinical predictors of diabetes testing is required to target high risk populations, create effective models of patient care postpartum and develop interventional strategies. We designed this study to address two important clinical questions: (1) do maternal characteristics, obstetrical factors, GDM care delivery or utilization of health services postpartum predict if a woman with GDM will complete a screening test in the first year postpartum? and (2) Do women delay their diabetes screen with a 75 g OGTT outside the recommended time period of 6 months (i.e. between 6 and 12 months postpartum)?
Methods
A retrospective cohort study was performed of 556 women with a diagnosis of GDM who received prenatal care in Ottawa, Ontario between 1 July 2007 and 30 June 2009. Ethics approval for this study was obtained by the Research Ethics Committee of both The Ottawa Hospital and Queensway Carleton Hospital (Protocol #: 2009392-O1H). No individual patient consent was required as this was a retrospective chart review linking to an anonymized provincial administrative dataset.
Characteristics of the three clinical sites.

A reminder package, consisting of a letter and an outpatient laboratory requisition form for a 2-hour OGTT, was mailed within three months of delivery to women who attended the diabetes education class at sites A and B. Results of the OGTT were sent to the ordering physician and patient's PCP. The reminder letter explained the need for postpartum diabetes screening following a pregnancy affected by GDM. Women who attended site C (non-reminder site) did not receive a written reminder, but were educated during pregnancy of the importance of diabetes screening between 6 weeks and 6 months postpartum. Patients were also instructed to follow-up on test results with their PCPs.
Women were excluded (i) if they did not attend any diabetes education class or assessment at one of the participating Obstetric Medicine clinics; (ii) if they did not possess provincial health care coverage through the Ontario Health Insurance Plan (OHIP) and (iii) if their recorded OHIP health card number was invalid.
Maternal characteristics and obstetrical outcomes were collected by individual patient chart reviews. Baseline maternal characteristics included age, rural residence (determined by postal code at time of delivery), family history of type 2 diabetes, previous history of GDM, pre-pregnancy body mass index (BMI), GDM therapy (diet versus pharmacotherapy), parity and smoking status. Socioeconomic status was estimated ecologically using the patient's home postal code to determine the neighbourhood median household income, divided into quintiles. Obstetrical outcomes collected were gestational hypertension or pre-eclampsia, delivery by caesarean section, admission to the neonatal intensive care unit (NICU) and macrosomia (birth weight ≥ 4000 g). Postpartum health care utilization included attendance by the infant at a well-baby visit with a pediatrician, attendance by the mother to an ambulatory visit with her obstetrician, PCP, internist or endocrinologist; and completion of a Papanicolaou (PAP) test was derived from provincial physician service claims data from the Ministry of Health and Long-Term Care, held at the Institute for Clinical Evaluative Sciences. Because of the single-payer health care system in Ontario, these data comprehensively include all fee-for-service billing claims from physicians in Ontario. Patients were linked to these data using their unique health card number. We hypothesized that greater contact with the mother's PCP (e.g. using primary care rather than paediatrician for well-baby care) and participation in other health care screening behaviours (e.g. PAP testing postpartum) would be associated with increased likelihood of diabetes screening.
The primary outcome of interest was screening for type 2 diabetes with a 75 g OGTT for 2 h. The secondary outcome of interest was screening using the OGTT, other tests (random glucose, fasting glucose or HbA1c) or any glucose test (any of the above). Two sources were used to verify whether patients received postpartum diabetes screening – the hospital-based electronic record system (for tests done in hospital laboratories) and records of billing claims from community laboratories through provincial health care data as above. Results of laboratory tests were not available from the latter data source, only whether or not a test was performed.
The baseline characteristics of the patients were compared using chi-squared testing. Cox proportional hazards models were used to determine the independent effects of the baseline variables on the time to the primary and secondary outcomes, up to one year. Patients were censored at 12 months after delivery. Postpartum characteristics were treated as time-varying covariates in the models. The assumption of proportionality was verified by plotting log [–log (survival)] vs. log (time) to assess parallelism.
Results
We identified a total of 743 cases of women with GDM who attended a diabetes education class and were assessed at one of the three specialized clinics. A total of 188 cases did not meet inclusion criteria, leaving a total of 555 women. Of the 555 patients, 6 were excluded because the health card number did not correlate with the age and gender of the patient recruited (e.g. health card number linked to an elderly male patient instead – likely due to recording error). Three cases of stillbirths were excluded as neonatal and some postpartum predictors could not be measured (e.g. well baby paediatric visit in the first 6 months). An additional four cases were omitted from the Cox hazards model due to missing patient data for GDM pharmacotherapy and parity, leaving 542 patients (181 women at site A, 157 at site B, and 208 at site C) for the final analyses.
Baseline maternal and obstetrical characteristics by site.
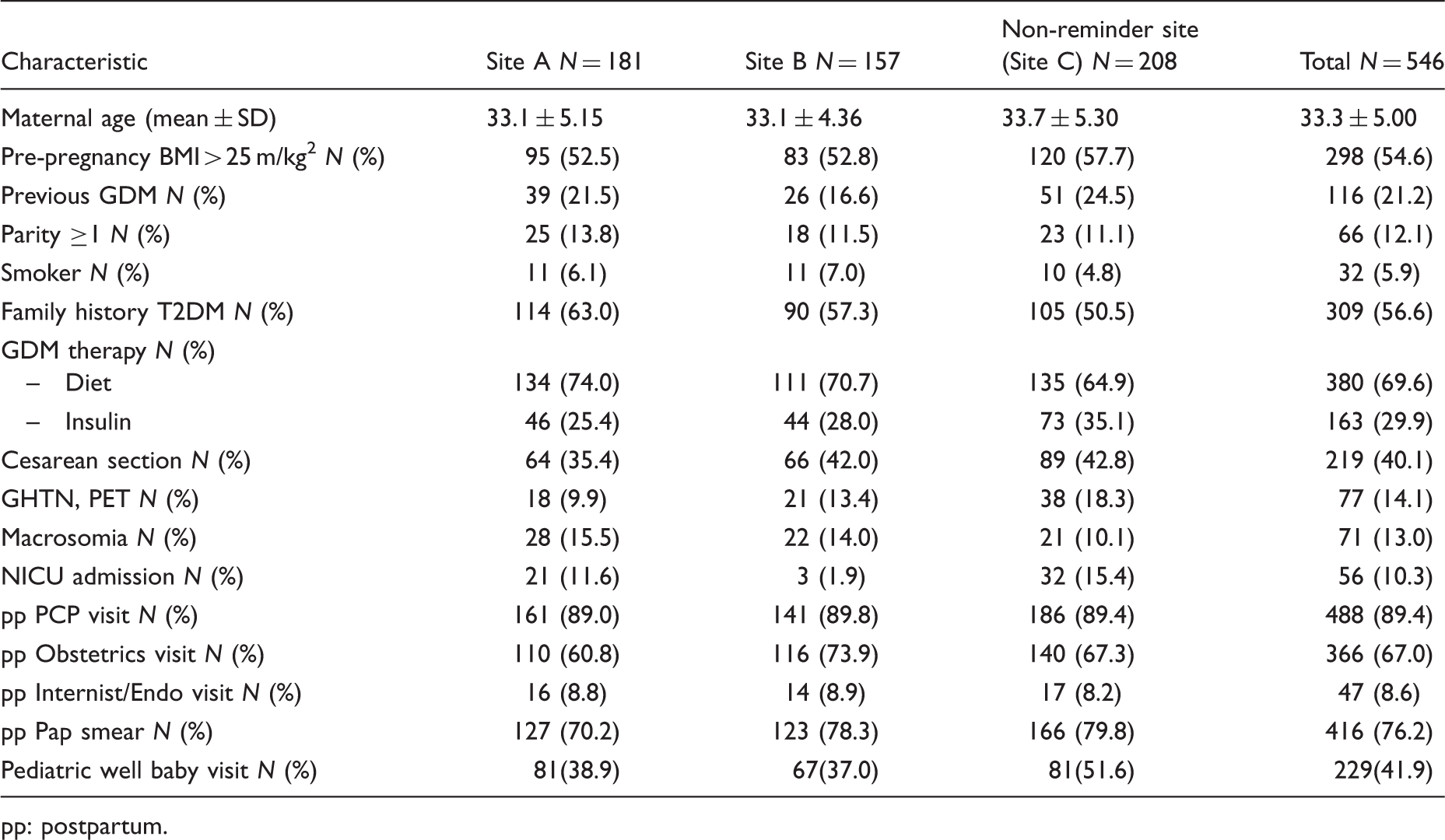
pp: postpartum.
Diabetes screening rates in the first year postpartum by clinic site.

Clinical predictors of testing by Cox hazards model.

CI: confidence interval; pp: postpartum.
Discussion
We have previously demonstrated the impact of reminders on postpartum screening rates.9,10 This study attempted to identify if other factors, including access to providers in the postpartum period and participation in other screening behaviors (PAP tests), influenced postpartum OGTT rates. Smoking status, which may reflect health behaviours and attitude towards primary prevention, was the only maternal factor associated with screening rates. We identified that the site of care delivery for women with a previous diagnosis of GDM was the strongest predictor for whether a woman completed the recommended test for postpartum screening within one year. Maternal age, socioeconomic status, postpartum follow-up with an obstetrician and completion of a PAP test in the first year of delivery demonstrated positive trends, but did not reach statistical significance. These findings suggest that interventions to increase screening rates do not need to be individualized to target subsets of this high risk population, but rather should focus on how care is delivered.
It is difficult to know specifically which element of the health care model was responsible for the difference in screening rates. Aside from implementation of a patient reminder system at sites A and B, there are several notable differences between the clinic sites that participated in this study. Sites A and C provided outpatient clinics within university-affiliated tertiary care hospitals. The primary provider at site A was a general internist and/or endocrinologist, compared to site C where care was provided by an obstetrician who specialized in maternal fetal medicine. Differences in medical training of the provider may have resulted in different priorities and emphasis for postpartum care, and communication of long-term diabetes risk – despite GDM being considered within the scope of practice for both specialties.16,17 However, it should be noted that the importance of postpartum testing is highlighted in educational classes at all three sites. Sites A and C are university-affiliated, so patients often interact with medical and obstetrical residents trainees under the direct supervision of the staff physician. The delivery of care at these clinics may be more variable given the interaction with trainees. In contrast, site B was located in a local community hospital and the same team (consisting of an endocrinologist, diabetes nurse educator and dietician) managed all patients. It should also be noted that patients seen at site B were generally of a higher socioeconomic status and presumably education level. However, this difference did not reach statistical significance.
Others have looked at predictors of glucose screening postpartum, primarily focusing on non-modifiable factors such as age, treatment of GDM, ethnicity and socioeconomic status and found conflicting results.5,18 Very few studies, mostly centred in academic care institutions and non-universal health care coverage, have looked at impact of care delivery model on screening rates. Two studies found a small effect of practice location on glucose testing which was not significant after adjustment for potential confounders.19,20 Two groups at Kaiser Permanante have implemented system changes (i.e. case managers, reminders, provider education) and shown benefit.15,19
It is important to recognize that the postpartum period is a time of transition between providers. Perceived barriers for not completing postpartum testing include not attending postpartum visits/being lost to follow-up.6,21 In different settings, the responsibility for screening postpartum could fall to the obstetrician or endocrinologist/internist responsible for the care of the GDM or to the PCP. This may be in part determined by health care coverage. In our region, where universal health care is provided to all individuals, patients and providers feel strongly that the PCP is the preferred option. 6 In other models, it may be the obstetrician or endocrinologist/internist looking after the GDM during pregnancy who is felt to be responsible for ordering postpartum testing. Some studies where this is the accepted model have demonstrated higher screening rates in women who attended their postpartum visit with the obstetrician or endocrinologist.19,22–24 Our study did not demonstrate any significant association of postpartum health care utilization of the obstetrician, PCP or completion of the PAP smear. Thus, it does not appear that attending visits postpartum translates into test completion. We hypothesize that receiving a reminder and laboratory requisition in the postpartum period enabled the woman to complete the test independently, as it did not need to be requested by her PCP.
Our study focused on whether the recommended OGTT was completed, whereas most others have only reported if a fasting glucose or any glucose testing was done. When compared to the OGTT, single glucose and haemoglobin A1c levels have consistently been shown to be insensitive screening tests for type 2 diabetes in the postpartum period.25–33 Recently, Capula et al found that 32.3% of women with previous GDM completed an OGTT within 6 and 12 weeks postpartum. Prepartum counselling and a diagnosis of polycystic ovarian syndrome were the strongest predictors of adherence to completing a postpartum OGTT. 34
The role of timing of glucose testing was a secondary objective of this study. To determine the impact of interventions to improve postpartum screening, it is important to determine appropriate timeframes. Although guidelines suggest screening before 6 months, it is possible that women, especially those that are breastfeeding, may not be able to meet that timeframe. An additional 12% of women in our study completed their OGTT at 6–12 months postpartum. Thus, 37% of all women screened with an OGTT within the first year did so between 6 and 12 months postpartum. In our study, the impact of site of practice continues throughout the first year even though no further intervention was provided after the reminder letter was sent. There is very little information on long-term impact of postpartum interventions. Chittleborough et al. (2010) examined diabetes screening rates over five years postpartum. 35 Study participants and their PCP's received an initial reminder letter at 15 months postpartum, and then a subsequent reminder letter every 12 months thereafter. Self-reported rates of any blood glucose testing (not OGTT) increased from 56.3% to 75% with mailing of a second reminder letter. 35 Our results may not be transferrable to other jurisdictions. There is no limit or change in health care insurance for our women postpartum and many women take advantage of a one-year maternity leave policy.
There are several limitations to our study. The study is of a retrospective design, which did not allow for the analysis of potential confounders, including maternal characteristics such as ethnicity, occupation, education, marital status, past medical history and breastfeeding rates. Although our total sample size is modest, the multicultural and diverse population in the Ottawa geographic region permits our results to be generalized to other populations. Lastly, as with any postal system, we could not confirm that the mailed reminder packages were received by the intended patient, but data were analysed as intention to treat.
In summary, although adherence to current practice guidelines for diabetes screening in women with a history of GDM remains less than ideal, on-going research continues to provide insight into strategies that reduce both health care provider and patient barriers to screening. The model of care delivery has tremendous impact on implementation of screening recommendations and should be a focus of future research.
Footnotes
Acknowledgments
Our paper was presented as an oral abstract at the Canadian Diabetes Association Annual meeting held in Vancouver BC, October 2012.
Declaration of conflicting interests
The opinions, results, and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred.
Funding
This study was funded by the Ministry of Health and Long-Term Care of Ontario and Canadian Institutes of Health Research. This study was supported by the Institute for Clinical Evaluative Sciences (ICES), which is a non-profit research institution funded by the Ontario Ministry of Health and Long-Term Care (MOHLTC).
Ethical approval
Ethics approval for this study was obtained by the Research Ethics Committee of both The Ottawa Hospital and Queensway Carleton Hospital (Protocol #: 2009392-O1H). No individual patient consent was required as this was a retrospective chart review linking to an anonymized provincial administrative dataset.
Guarantor
Patricia Peticca.
Contributorship
All authors contributed to the design and interpretation of the study. All authors reviewed the final manuscript.