
Abstract
Background
Intrahepatic cholestasis of pregnancy is a cholestatic disorder with an increased risk for adverse perinatal outcome. The mechanism underlying intrauterine demise is poorly understood.
Case
A nulliparous woman with gestational age of 36 plus 6 weeks presented with suspected intrahepatic cholestasis. Continuous CTG monitoring evolved from a normal pattern towards a non-reassuring pattern. A male neonate was delivered by caesarean section. Apgar scores 0, 1 and 4 at 1, 5 and 10 min. Fetal cord gas analysis showed pH 6.98, base deficit –15 mmol/L. Blood results showed maternal serum bile acid concentration of 220 µmol/L.
Conclusion
Our case suggests gradual evolution towards hypoxia and acidosis. It is unknown whether certain components in the bile acid concentrations might contribute to a fetal metabolic component of the acidosis.
Keywords
Introduction
Intrahepatic cholestasis of pregnancy (ICP) is a cholestatic disorder unique to pregnancy. It is characterised by pruritus, elevated serum aminotransferases and bile acid levels. While maternal prognosis is favourable with rapid resolution after delivery, there still remains debate about possible adverse fetal outcomes. Earlier studies reported increased incidence of preterm delivery, meconium stained liquor, fetal distress and intrauterine death, leading to a more interventional obstetric management. 1 While the association with increased fetal risks has been challenged in recent studies, case reports of unexpected intrauterine death still remain frequent and the deaths often occur shortly after normal non-stress tests. Therefore, a general impression of increased risk for adverse perinatal outcome remains when serum concentrations of bile acids exceed 40 µmol/L. 2 The mechanism underlying intrauterine demise is poorly understood.
In this article, we report the condition of a fetus evolving from a reassuring state to severe acidosis despite continuous CTG monitoring without any other indicative cause other than the maternal intrahepatic cholestasis.
Case report
A 40-year-old normotensive nulliparous woman was admitted at 36 weeks plus six days gestation with minimal abdominal discomfort. Her history included systemic lupus erythematosus, treated with prednisone, azathioprine and hydroxychloroquine. Her body mass index was 24 kg/m2 and during pregnancy the blood glucose levels were normal with no signs of gestational diabetes. The family history only reported hypertension. As she reported mild pruritus the previous day in outpatient clinic, blood tests were initiated, indicating marginally elevated transaminases, with bilirubin and bile acids still pending. There were no signs of pre-eclampsia. Intrahepatic cholestasis was suspected and the patient was admitted for further workup and fetal monitoring.
The first hour of the non-stress test was reactive with baseline fetal heart rate 140 bpm, variability of 15 bpm and occasional accelerations without decelerations (Figure 1(a)).
(a) Reassuring CTG with baseline fetal heart rate of 140 bpm, variability of 15 bpm and occasional accelerations without decelerations. (b) Variable deceleration at 08:50 hours lasting 90 s to a nadir of 100 bpm, with a slow but reactive recovery to the baseline. (c) Increased baseline of 150–160 bpm. (d) Reduced variability with alternating episodes lasting 40–60 min of absent to again minimally acceptable short-term variability. (e) CTG with even more reduced variability and shallow decelerations without accelerations. A caesarean section was decided upon this CTG.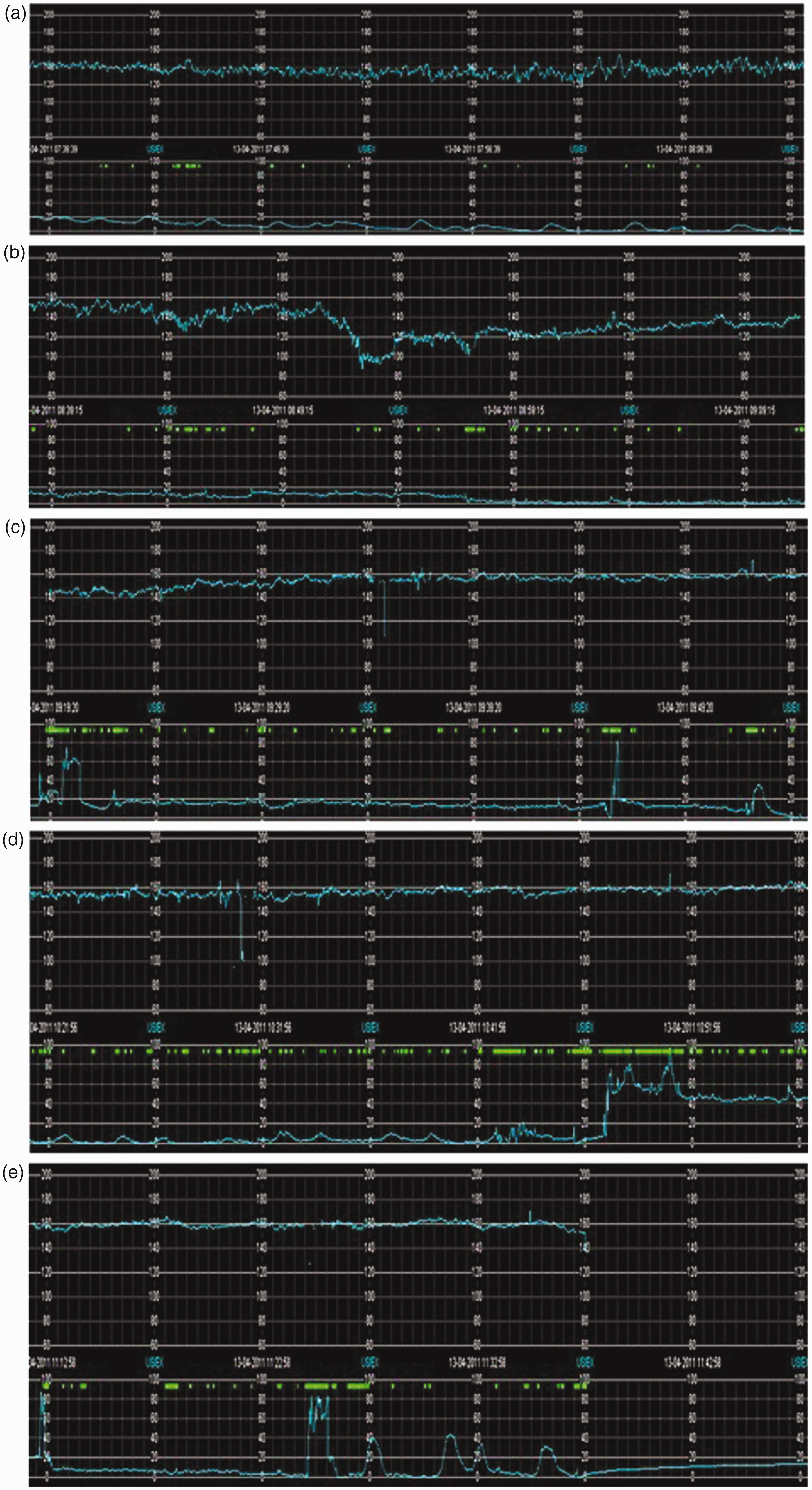
Due to other activities on the maternal ward, the patient was not disconnected after 30 min of reassuring non-stress test. After approximately 1 h, there was a slight elevation in baseline fetal heart rate to 150 bpm with sustained variability but without clear accelerations. Thirty minutes later, a variable deceleration occurred lasting 90 s to a nadir of 100 bpm, after a maternal change in position, with subsequent appearance of a slow but reactive recovery to the baseline (Figure 1(b)).
The patient was shortly disconnected for a sanitary pause after which fetal heart rate returned to a baseline of 150–160 bpm (Figure 1(c)).
The variability was reduced with alternating episodes lasting 40–60 min of absent to again minimally acceptable short-term variability. The patient did not complain of abdominal or uterine pain, there was no blood loss or uterus en bois and tocography showed minimal uterine activity (Figure 1(d)).
As the CTG remained non-reassuring with even more reduced variability and possible shallow decelerations without obvious cause, further assessment by ultrasound was decided upon (Figure 1(e)). There were no signs of abruption of the placentae.
However, as fetal movements and respiratory movements remained absent, a decision was made for delivery by caesarean section.
The patient was transferred to theatre where spinal anaesthesia was administered. Fetal heart rate monitoring before and immediately after the spinal anaesthesia showed an FHR of 150 bpm without signs of deceleration. Five minutes later, a male neonate was delivered, weighing 2460 g (p16–20) with Apgar scores 0, 1 and 4 at 1, 5 and 10 min. The initial fetal cord gas analysis was pH 6.98, base deficit – 15 mmol/L. At resuscitation, airway clearance proved to be difficult. The infant was intubated at 5 min and a pulse was detected at 8 min after two doses of epinephrine. Subsequent arterial gas 4 h later showed pH 7.17, base deficit –14 mmol/L. The neonate was admitted to the neonatal intensive care and received therapeutic hypothermia for 72 h. Fenobarbital was initiated for subclinical epileptic seizures. Ultrasound and MRI scan showed signs of damage to the caudate and dentate nuclei, the thalamus and cerebellar vermis with normal appearance of white matter and cortex, compatible with moderate to severe asphyxia. The infant had a good clinical recovery and could be discharged to a medium care department at 12 days of age. Follow up at six and 10 months revealed a mild hypertonic hemiparesis on the left side.
At the caesarean section, thick yellowish meconium stained liquor was noted. The placenta weighed 426 g and appeared grossly normal, with yellowish staining of the membranes overlying the placenta. There were no signs of abruption of the placentae.
A day after the delivery maternal blood results showed a very high total serum bile acid concentration of 220 µmol/L, confirming the diagnosis of intrahepatic cholestasis of pregnancy.
Discussion
The pathophysiology of adverse fetal outcome in ICP is still poorly understood. An accumulation of bile acids in the fetal circulation and amniotic fluid occurs through an increased flux of bile acids from the maternal to the fetal circulation as well as decreased placental clearance through vectorial transfer.1,3 This increased level of fetal bile salts, which is more prone to occur with increased maternal levels, is probably related to the adverse outcome, but the exact mechanism remains unknown.
Sudden arrhythmia has been suggested, as previous cases of intrauterine demise were often unexpected, within hours after a normal non-stress test. Studies in neonatal rat cardiomyocytes showed that tauro-conjugated primary bile acids can acutely alter the rate and rhythm of cardiomyocyte contractions. It was hypothesised that raised fetal serum bile acids in ICP cause fetal arrhythmia and sudden intrauterine death. 4 Another study suggests a marginally prolonged PR interval in fetuses of mothers with ICP compared to healthy controls, which could eventually precede ventricular arrhythmias. Still, the increase in PR interval remained well within normal limits for healthy fetuses.5,6 Despite these studies, the explanation of sudden fetal death in ICP due to arrhythmia remains hypothetical as any substantial evidence is still lacking.
In our case, the neonate showed complete absence of heart activity with extremely difficult cardiac resuscitation despite sustained fetal heart rate of 150 bpm minutes before delivery. While we cannot exclude sudden arrhythmia as a cause for the poor neonatal start, we still believe that the combination of acidosis and hypoxia along with difficulty to create a patent air entry are more likely to have caused the problem. The occurrence of meconium stained fluid in pregnancies complicated with ICP is much higher than in uncomplicated pregnancies.1,2 Meconium penetrates deep into placental and umbilical cord tissue in less than 3 h, causing vasoconstriction of the vessels. 7 In ICP, the meconium contains elevated levels of bile acid, known to cause vasoconstriction of the placental chorionic vessels leading to a rapidly progressive reduction in oxygenated blood flow. 8 Therefore, it is possible that placental vasoconstriction leading to hypoxia and acidosis is the mechanism for adverse fetal outcomes.
Up to now, all reported cases of ‘sudden intrauterine death’ were days to hours after normal non-stress test. It is conceivable that the progression to acidosis is more rapid in ICP as compared to other pathologic conditions, due to the high bile acid concentrations in the fetal circulation and amniotic fluid.
While unfortunate from a clinical point of view, the uniqueness of our case lies in the continuous CTG monitoring gradually evolving from a normal pattern towards a non-reassuring or even pathological pattern until minutes before the outcome. It gave us the new opportunity to observe the potential pathophysiological mechanism behind ICP. Our case, with a progressive rise in fetal heart rate and reduced variability, without severe decelerations, suggests a rapid but gradual evolution towards hypoxia and acidosis. It is unknown whether certain components in the bile acid concentrations might contribute to a metabolic component of the acidosis. In conclusion, we can say that an unexpected fetal acidosis is a possible explanation for adverse fetal outcome in intrahepatic cholestasis of pregnancy.
Footnotes
Declaration of conflicting interests
None declared.
Funding statement
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
We have obtained the written consent from patient for publication.
Guarantor
JC.
Contributorship
KS wrote this case report, analysing previous cases and reports about intrahepatic cholestasis of pregnancy. WV analysed the case from the perspective of internal medicine and she revised the article critically. LS wrote the neonatal outcome. She is the paediatrician who was involved in the treatment of the neonate. She also revised the article critically. JC analysed data about intrahepatic cholestasis of pregnancy, writing the article together with KS and revising it critically several times.
All authors accept the responsibility for the article as published.