
Abstract
Introduction
The process of labour and delivery is the most common emergency in a woman’s life. The millennium development goal (MDG) 5 is a reduction of maternal mortality by 2/3 by the year 2015. The most effective strategy suggested by WHO to achieve this goal is provision of Emergency Obstetric services. There is a wide regional variation in maternal mortality rates as well as the causes of maternal deaths worldwide and also in India. Analyzing the maternal deaths helps to understand the profile of patients who sought the services of emergency obstetric care (EmOC) and informs reorganization of our EmOC services to tackle the causes effectively. The Institutional Maternal Mortality Rate (MMR) is high when compared to the National average or Global average, 1 as the Institutional delivery rate is increasing gradually in India. 2 According to the National Family Health Survey III, institutional deliveries have increased by 25% during the years 2001–2006 and the national MMR decreased by 15%. The rate of decrease is not yet adequate to attain the goal of 2015. The objective of the present study was to determine the trend in MMR over the past five years at JIPMER (Jawaharlal Institute of Postgraduate Medical Education and Research) Hospital and to find out the proportion of maternal deaths in relation to emergency admissions. JIPMER Hospital is a tertiary care teaching centre in South India which provides free services to a large population all over South India and also other parts of India and is equipped with all comprehensive EmOC facilities.
Material and methods
This is a retrospective analysis of maternal deaths that occurred between January 2008 and December 2012. The maternal death records were retrieved from the medical record section of the JIPMER hospital and the data were analysed with respect to the type of admission, referral and cause of death. The clinical profile of the patients was also studied. MMR was expressed as the number of maternal deaths per 100,000 live births. WHO classification of maternal deaths was followed to classify the cause. The results are expressed as percentages and proportions. Ethics committee/IRB approval was not obtained as this was a retrospective analysis and the results were presented in the National conference ISMET 2013 hosted by our institute.
Results
Maternal mortality rate.

Clinical profile.
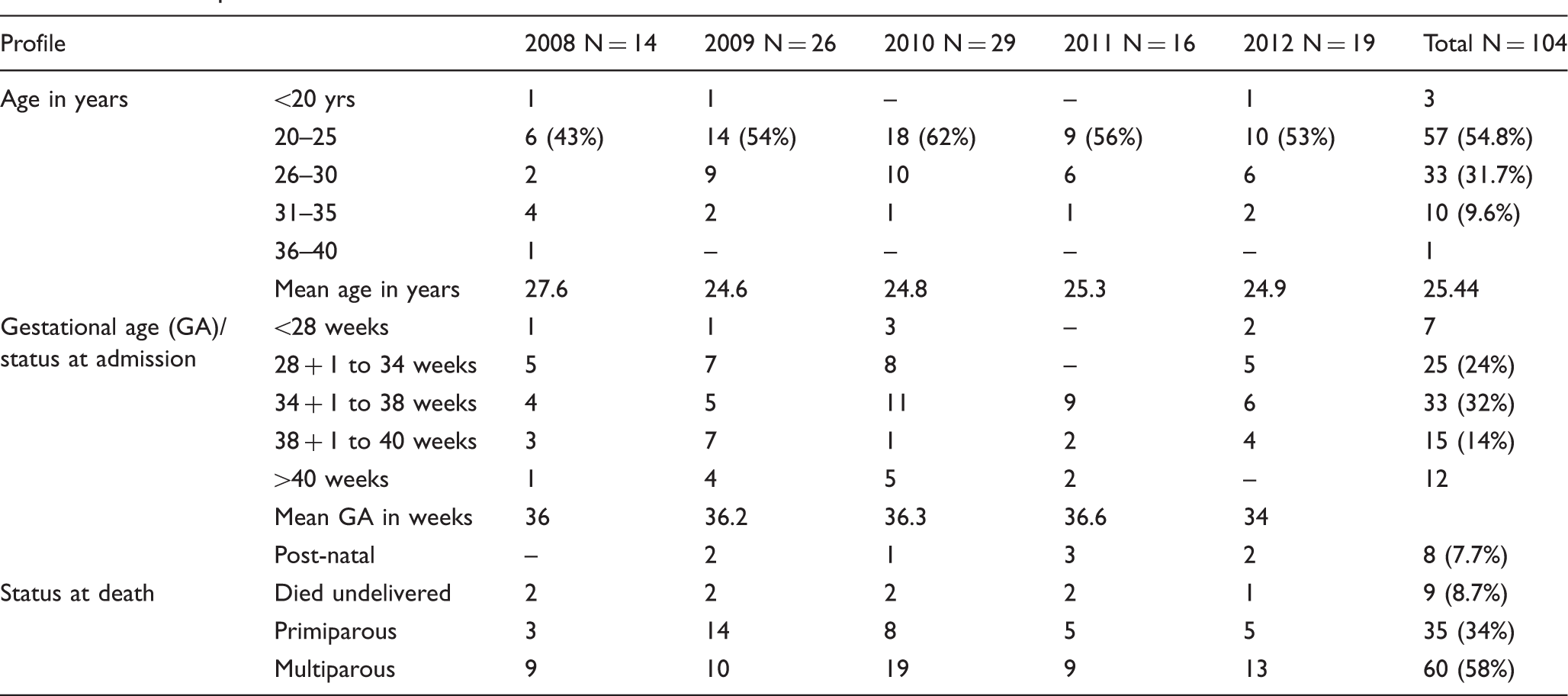
Admission profile and hospital stay.
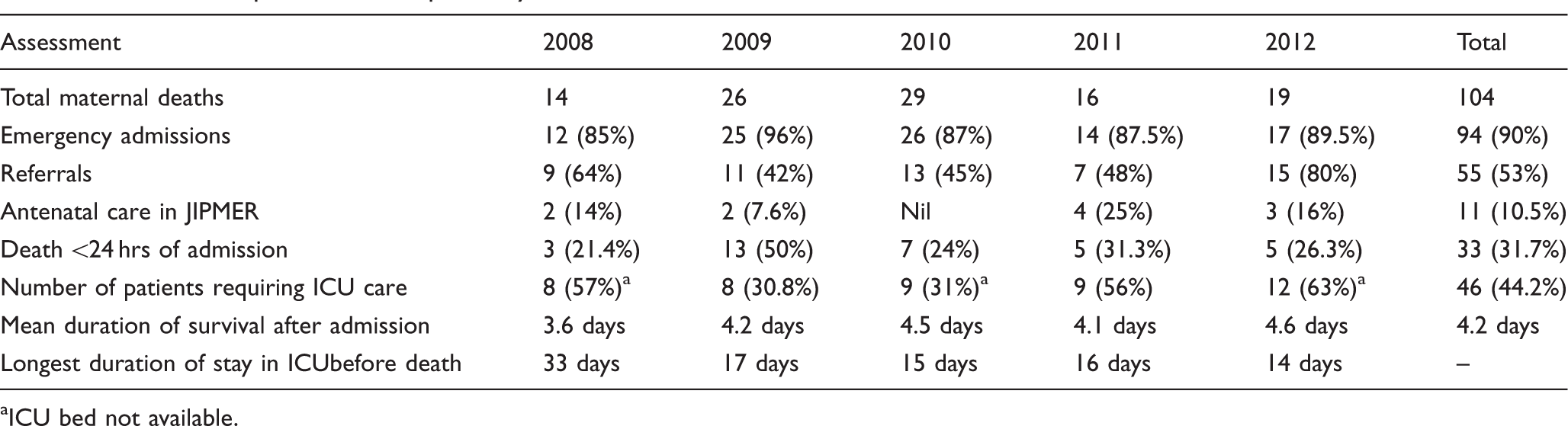
aICU bed not available.
Overall, 32% of the patients died within 24 h of admission and 44% were admitted to ICU (Intensive Care Unit). ICU admissions showed an increasing trend from 2009. The mean duration of ICU stay was 4.2 days and the longest duration was 33 days. The patient in ICU for 33 days was an unwed mother at term admitted with eclampsia with intrauterine death at term who had persistent convulsions. Her CT brain showed hydrocephalous and she was found to be HIV positive. There was lack of ICU beds for three patients. Status at death showed 58% to be multiparous and 34% primiparous; 92% died after delivery and 8.7% died undelivered.
The causes of maternal deaths are shown in Table 4. The commonest cause is obstetric hemorrhage followed by hypertensive disorders of pregnancy including eclampsia. Overall direct causes accounted for 60% of deaths and indirect causes for 40%. The most common indirect cause is heart disease complicating pregnancy followed by severe anaemia and jaundice. Infectious causes (malaria, tuberculosis and HIV) accounted for 2%. There were two cases of liver secondaries; one from breast cancer and the other from osteogenic sarcoma of femur. Both of them occurred after primary treatment was given. The trend over the five years is a decrease from direct causes and increase in indirect causes. The trends in MMR, admissions and causes are depicted in Figures 1, 2, and 3, respectively.
Trend in MMR. MMR and trend in admissions. Trend in causes of MMR. Causes of maternal deaths. One patient who was admitted as eclampsia was subsequently diagnosed to be HIV with hydrocephalous (neurological involvement).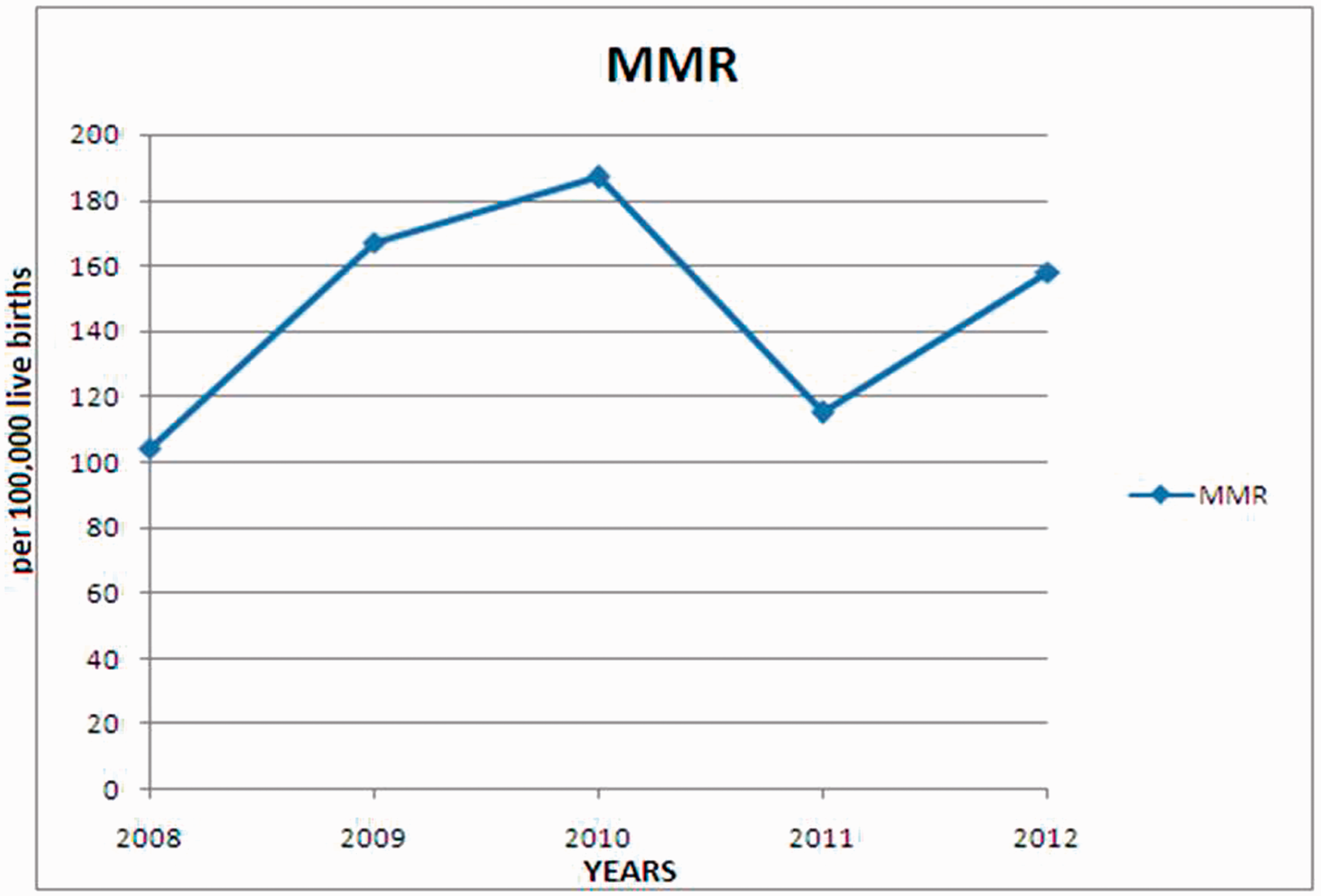



Discussion
MMR is considered to be high if it is ≥300 maternal deaths per 100,000 live births and extremely high if it is ≥1000 maternal deaths per 100,000 live births. India is one of the countries in the world with high maternal mortality and is responsible for one-third of global maternal deaths along with Nigeria. Maternal mortality in India has a wide regional variation; it is highest in northern Indian states like Assam and lowest in southern Indian states like Kerala. 3 Mortality depends on many factors including social, economic, literacy rates and also on the availability of health care facilities. The three or four delay model emphasizes the factors and possible prevention. The third or the fourth delay depends on the availability of skilled personal and facilities. In the present study, reaching health care facility late is an obvious contributor, as 90% of the deaths occurred among emergency admissions and 32% of them died within 24 h of admission. This is similar to the study by Sikdar and Konar where 32% died within one day. 4 This highlights the need for correcting the first delay in this region so as to improve access to quality care. Quality care is a major determinant of health outcomes and is adversely affected when the health care facility is overcrowded 5 and this situation prevails in our institute. Government programmes are still focusing on antenatal care, high-risk approach, trained birth attendants neglecting delivery care and EmOC. Lack of facilities to perform a CS at peripheral health centres (PHC), no CTG, facilities for blood transfusion or paediatrician, with only one medical officer to look after all kinds of cases everyday and the lack of transport facilities in remote places are some of the barriers which contribute to high maternal mortality. 6 Provision of comprehensive emergency obstetric services within the reach of all pregnant women is one of the strategies employed to reduce the maternal mortality worldwide. The public is made aware of the availability of such services free of cost in government institutions.
Fifty percent of the women were referred in a critical condition requiring ICU care. However, even though our healthcare facility is a tertiary care institute, it lacked obstetric ICU and there were delays in instituting immediate ICU care, as ICU for these patients is dependent on the availability of beds in respiratory intensive care unit (RICU) which delivers care for all other specialty patients in critical condition. Some patients were ventilated in the labour room itself due to lack of beds in RICU. Lack of intensive care facilities for critically ill obstetric patients leading to mortality is also one of the factors reported in the large multicentre study by Hiralal and Baran. 1 According to WHO, provision of basic as well as comprehensive EmOC care is one of the strategies to be employed to reduce MMR. But comprehensive EmOC care does not include the provision of ICU care as one of the requirements. 7 A community-based death review in India recently reported on the lack of lifesaving treatment for obstetric complications at the appropriate level in government facilities. 8 Similar findings are reported from Kenya and Jambia.9,10 Presence of skilled birth attendants and facilities for properly resourced EmOC is of prime importance to prevent maternal mortality. Though complications of pregnancy cannot be eliminated altogether, reorganization of the health system is essential 11 to face the increasing load of complications causing both direct and indirect maternal deaths particularly the expected rise in indirect causes.
The finding of the commonest causes of death as postpartum haemorrhage hypertensive disorders of pregnancy is similar to the global causes of maternal deaths. 12 The 60:40% proportion of direct and indirect causes and the trend of increasing indirect maternal deaths is similar to the study by Chakraborthy and Sebanthi. 13 Banagal et al. found 50% of direct causes and 50% of indirect causes of maternal deaths. 14 A WHO systemic analysis on global causes of maternal deaths revealed indirect causes and haemorrhage are the major causes of maternal mortality worldwide. 15
In the present study, 90% of deaths were in the postpartum period and this is close to the observation of Purandarare et al. 16 This is in contrast to the study by Kassebaum et al. who reported only one quarter of deaths occurring intrapartum and immediately postpartum. 11 Very young women lost their lives as 55% of the present cohort were less than 25 years of age and almost 90% percent were less than 30 years of age. This is similar to other studies in India. Though the MMR in the present study is less than the national average, some of the deaths could have been prevented by the provision of timely dedicated ICU care. Although some states like Kerala and Tamil Nadu have achieved MDG goal 5, India as a whole has to make continuous efforts to attain MDG 4 and 5. 17 In the Obstetric transition, India is in stage III 5 and each healthcare facility has to concentrate on provision of quality care, correcting the intrahospital issues especially the third delay.
Conclusion
The majority (90%) of maternal deaths were among the emergency admissions and there is an increasing trend of referrals in critical condition requiring ICU care. In this analysis, there is an increasing trend of indirect causes of maternal deaths and decreasing trend in direct causes. Strengthening and upgrading of EmOC facilities are required to reduce MMR and inclusion of obstetric intensive care facilities in the comprehensive EmOC is essential to achieve the goal.
Footnotes
Acknowledgements
I would like to acknowledge the permissions given by Professor Syed Habeebullah (unit I head), Professor Rani Reddy (Unit III head) and Professor S. Raghavan (Unit IV head) for collating the maternal death records of their respective units. I also express my gratitude for the staff of MRD who retrieved all the maternal death records. I am thankful to Dr. John Davis for preparing the figures and checking the data.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sector.
Ethical approval
NA (as it is a retrospective study based on hospital records and the subjects are no more—Mortality study).
Guarantor
PD.
Contributorship
PD conceived the idea for this study, reviewed the literature, analysed each maternal record retrieved from JIPMER medical record section with the help of staff working in MRD section, received consent from the other three unit heads to analyze the maternal deaths from their units also as per the requirement of medical record section of JIPMER to allow to access to the records.