
Abstract
Background
Shortness of breath is a common physiological pregnancy presentation, secondary to both hormonal and mechanical effects. Its pathological causes are common (asthma exacerbation or infection); new-onset cardiac pathology is rarely considered.
Case
JC, a 39-year old G4P2T1, presented at 34 weeks’ gestation with shortness of breath unrelieved by salbutamol. History included asthma, poly-drug abuse and smoking. Initial presentation was consistent with asthma exacerbation and she was treated as such. There was deterioration of symptoms and on re-examination raised jugular venous pressure was noted with bibasal lung crepitations and cardiac systolic murmur. Echocardiogram showed severe cardiomyopathy (left ventricular ejection fraction 20%). JC was commenced on diuretics, digoxin and fluid restricted. Labour was induced at 35 weeks’ gestation, with birth of a healthy female infant (BW 2475 g) by elective assisted vaginal delivery. Cardiac function improved in subsequent weeks, confirming peripartum cardiomyopathy.
Conclusion
Peripartum cardiomyopathy affects 1 in 2500–4000 live births. Over 90% of women regain normal cardiac function postpartum with optimal medical management. Peripartum cardiomyopathy presents a diagnostic conundrum as its primary symptoms mimic not only those of normal pregnancy but also a number of other, more common conditions.
It is important to consider cardiac causes of shortness of breath initially, and vital to revisit an initial non-cardiac shortness of breath diagnosis if there is no sustained improvement with treatment. In this case, asthma history and initial wheeze on examination impeded correct diagnosis; however, the situation was re-evaluated and correct diagnosis made when the patient’s shortness of breath deteriorated.
Subsequent multidisciplinary management and birth in an appropriate setting facilitated the best outcome for both mother and baby.
Background
Shortness of breath (SOB) is a common physiological pregnancy presentation, secondary to both hormonal and mechanical effects. Its pathological causes are commonly asthma exacerbation or infection; rarely exacerbation of known, or new-onset, cardiac pathology. This case is a reminder of its many diagnostic possibilities.
Case
JC, a 39-year old G4P2T1, presented at 34 weeks’ gestation with SOB unrelieved by salbutamol. History included asthma (prn salbutamol), poly-drug abuse, and 24 pack-years of smoking. Obstetric history included two term live births, 24-week stillborn twins and poor attendance for antenatal care. Antenatal serology (including virology) was unremarkable.
Blood results during admission.
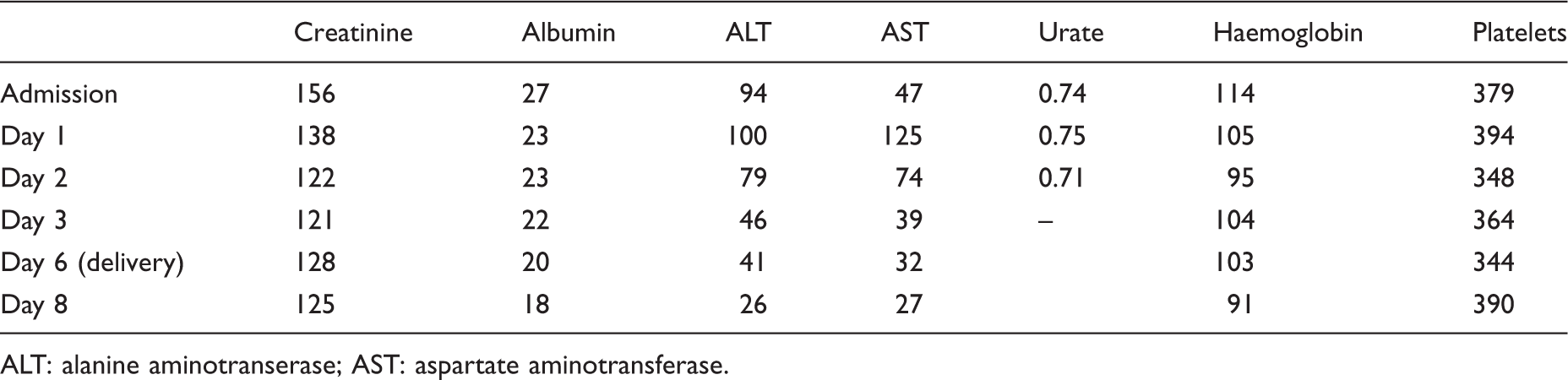
ALT: alanine aminotranserase; AST: aspartate aminotransferase.
JC was admitted for asthma exacerbation treatment and investigation of AKI, with initial differentials of an underlying chronic glomerulonephritis perhaps secondary to illicit drug use, infection and pre-eclampsia. As blood pressure normalised without medication and renal function stabilised with hydration (Table 1), the respiratory symptoms in the context of a known asthmatic became the dominant acute issue. These initially responded to increased salbutamol, but deteriorated again, and on day 2 bibasal lung crepitations, raised jugular venous pressure and cardiac systolic murmur were noted. Echocardiogram (Figure 1) showed dilated cardiomyopathy with dilated left ventricle with global systolic dysfunction (left ventricular ejection fraction 20%) and moderate functional mitral valve regurgitation and no vegetations; chest X-ray showed significantly enlarged cardiac silhouette and evidence of pulmonary congestion but no pleural effusions; she remained afebrile.
Transthoracic echocardiogram image showing dilated left ventricle.
Transfer to coronary care for monitoring and management of peripartum cardiomyopathy (PPCM) occurred; diuretics, digoxin and 1.2 L fluid restriction were commenced. Labour was induced at 35 weeks’ gestation, with birth of a healthy female infant (BW 2475 g) by elective assisted vaginal delivery. Cardiac function improved in subsequent weeks to an ejection fraction of 40% confirming PPCM. Post-natally, management has remained conservative; medications were rationalised to account for the non-pregnant state and the completion of breastfeeding. JC continued on perindopril, digoxin, aldactone and bisoprolol. Further investigations regarding renal function are planned.
Discussion
PPCM affects 1 in 2500–4000 live births; over 90% of women regain normal cardiac function postpartum with optimal medical management. 1 As exemplified, it continues to present a diagnostic conundrum, as primary symptoms mimic those of normal pregnancy and also a number of other more common conditions 2 including asthma and anaemia.
Diagnosis
The major challenge of this case was presented not by the finding and treatment of PPCM but by arriving at the diagnosis. PPCM is accepted as a diagnosis of exclusion; however, arriving at this conclusion requires consideration as a differential for SOB. 3
JC presented with a known history of asthma, as such exacerbation of a known pathology is not an unreasonable initial diagnosis. Asthma exacerbations occur in approximately one-third of pregnancies of women with asthma, most commonly in the late second and third trimesters, with triggers including viral infection and non-compliance with inhaled steroid regimes.4,5 Impetus for further investigation in this case was provided when there was no adequate response to escalating asthma treatment. At this time, JC was re-examined and found to have a murmur with subsequent echocardiogram suggesting PPCM. Compensated cardiomyopathy can persist for months with no significant symptoms. 3 In this case, given the patient’s 6-week history of cough and mild SOB, it is probable that the additional intravenous fluids unmasked signs of previously subtle cardiac dysfunction in a volume depleted state, precipitating an acute decompensation.6,7 How frequently PPCM demonstrates a similar, more subacute initial clinical course is uncertain. However, time from symptom onset to diagnosis averaged 2.3 weeks (standard deviation 4.4 weeks) in a prior retrospective study, suggesting rapid cardiac decompensation is not always the PPCM presentation. 8
Given the complications in this pregnancy, future pregnancies are not advised. PPCM is characterised by good recovery; however, recurrence risk is high, particularly in those with recovery to ejection fraction of <55% such as this patient, 9 and PPCM mortality rates are 5–10%. Additionally, in some women PPCM is actually an unmasking of idiopathic dilated cardiomyopathy with serious implications for future health. 2
Multidisciplinary management
Management of such cases should be two-fold, with the focus first on the mother and then the safe delivery of the fetus. In this case, initial maternal stabilisation was vital. The patient was moved to an appropriately monitored ward where high-level cardiac care could be provided. Given the severity of disease (left ventricular ejection fraction <30%), delivery was deemed necessary and planned for 35 weeks with steroid cover. Through discussion with involved teams, assisted vaginal delivery was thought safest given previous normal vaginal deliveries and the haemodynamic shifts associated with caesarean section. 2 This was carried out in an appropriate area (high-dependency unit) under the care of relevant teams. Post-natally, the patient’s care continues to be informed by a multidisciplinary team to ensure a beneficial outcome. 6
Conclusion
As achieving a good outcome in PPCM relies on correct diagnosis, it is important to consider cardiac causes of SOB initially, and vital to revisit an initial non-cardiac SOB diagnosis if there is no sustained improvement with treatment. In this case, asthma history and initial wheeze on examination impeded correct diagnosis; the situation was re-evaluated and correct diagnosis made when the patient’s SOB deteriorated.
Subsequent multidisciplinary management and birth in an appropriate setting facilitated the best outcome for both mother and baby.
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of the staff of departments involved in the patient’s care.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Formal written consent was sought and received from the patient for the development and publication of this manuscript. Details have been de-identified to ensure patient confidentiality is maintained.
Guarantor
AH
Contributorship
The authors of this manuscript were directly involved in the care of the patient throughout her pregnancy and have contributed towards the acquisition and interpretation of facts of the case and revision of the manuscript. All authors consent to the publication of the manuscript herein submitted.