
Abstract
Background
Pregnant victims of childhood maltreatment are more likely to deliver preterm. The mechanisms explaining this relationship are unclear. The goal of the current pilot study was to investigate whether momentary stress and cortisol serve as mechanisms linking maltreatment history to gestational length.
Methods
Seventeen women enrolled in the study (35% maltreated). Women completed two study sessions at 27 and 34 weeks gestation. Following each session, at four times/day over two days, women reported their momentary stress levels by text message and provided corresponding salivary cortisol samples. Gestational length was determined by medical chart review.
Results
Higher reports of momentary stress were associated with shortened gestational length. High stress predicted lower cortisol concentrations for women with maltreatment histories but higher concentrations among women without maltreatment.
Conclusion
Results from this pilot study provide preliminary evidence for understanding mechanisms explaining increased risk for preterm birth among childhood maltreatment victims.
Preterm birth (PTB) is the most significant predictor of infant morbidity and mortality in the US. Women who were victims of childhood maltreatment are up to three times more likely to deliver preterm1,2 even after accounting for current abuse, substance abuse, and low socioeconomic status. 2 Thus, childhood maltreatment is a robust, unique, prevalent, and underestimated risk factor for PTB. Researchers have hypothesized that maternal stress and concomitant hypothalamic-pituitary-adrenal (HPA) activity in pregnancy may be key mechanisms linking maltreatment history to PTB. 1 Our group recently published the first studies to show that pregnant women with childhood maltreatment histories display dysregulated diurnal HPA activity over pregnancy, 3 and that child maltreatment history moderates the relation between average daily stress and diurnal cortisol. 4 The aim of the current study was to extend this work by examining the role of momentary daily stress and cortisol in relation to gestational length among pregnant women with and without maltreatment histories. Momentary stress is an important consideration in HPA regulation because it is a closer approximation of how the HPA axis reacts in stressful situations and also minimizes recall bias. Past studies have reported that momentary assessments in pregnancy are better predictors of adverse birth outcomes and provides more accurate evaluation of HPA functioning than traditional one-time measures.5,6 No studies, to our knowledge, have used ecological momentary assessment (EMA) methodology among pregnant victims of childhood maltreatment history to assess momentary stress or cortisol functioning. We hypothesized that greater momentary stress and higher cortisol levels would predict shortened gestational length, particularly among women with maltreatment histories. Due to the exploratory nature of this pilot study, we also explored the relationships among momentary stress and cortisol between groups.
Methods
Participants
Participants were 17 women from a pilot study on the impact of everyday stressful experiences on gestational length (everyday events study [EVE]). Participants were randomly recruited from a larger, ongoing study of maternal smoking and infant development (Behavior and Mood in Babies and Mothers II). Participants completed two study visits as part of the larger study at 27 weeks (SD = 2) and 34 weeks gestation (SD = 1). A total of 100% of the sample completed the first study session and 82% completed the second study session. Three participants relocated prior to delivery; gestational length is missing for these individuals. This study was approved by Women and Infants Hospital and Lifespan Hospital Institutional Review Boards (Board Reference Number: 023512). All women provided written consent prior to their participation.
Procedure
Information on age, race, relationship status, socioeconomic characteristics, and obstetric conditions was collected through the ongoing study. For the pilot study, participants were interviewed about their current symptoms of depression in the previous week (assessed using the Quick Inventory for Depressive Symptomatology [QIDS], total scores range from 0 to 27 7 ) and self-reported their perceived stress levels over the previous month using Cohen’s Perceived Stress Scale (PSS) (total scores range from 0 to 40). 8 At four times per day for two days following each study visit, participants in the pilot study reported perceived momentary stress and provided corresponding salivary cortisol samples using EMA methodology. 9 Thirty minutes following the recording of their momentary stress level, participants provided a salivary sample that was later assayed for cortisol. Women were asked to refrain from eating and drinking between the recording of their stress level and their saliva sample.
Measures
Maternal history of childhood maltreatment
Participants completed a self-report measure of childhood abuse history that included items from the Adverse Childhood Experiences (ACE) scale. 10 Participants were asked how often they experienced childhood sexual abuse, physical abuse, neglect, or witnessed domestic violence, before the age of 18. Response options ranged from 1 (never) to 5 (very often). Childhood sexual and physical abuse have been shown to exert the greatest effects on HPA responses to stress. 11 Therefore, women with sexual and/or physical abuse were included in our maltreatment group. The comparison group included women with no history of maltreatment and women who reported a history of neglect or who witnessed domestic violence.
Gestational age at birth
We collected gestational age at birth on 14/17 (82%) of enrolled participants. Gestational age at birth was defined as the number of days between the last menstrual period and delivery date. PTB was defined as <37 completed weeks of gestation.
Ecological momentary assessment (EMA) of momentary stress
Participants were asked to record their momentary stress level via text message at four times/day for two days following the two study sessions (16 times/participant). We utilized a web-based, secure, and encrypted text messaging program to send and receive text messages to participants’ cell phones. Texts were delivered at semi-random intervals between 9 am and 6 pm (time intervals were ∼9 am–11 am, 11 am–1 pm, 1 pm–3 pm, 3 pm–5 pm). To record momentary stress, participants were asked to respond to the question “How stressed are you feeling right now?” on a scale of 0–10 (0 = none, 10 = very stressed). Participants completed 72% of EMA assessments of momentary stress. Compliance with the EMA protocol in this study was comparable to other EMA studies conducted in pregnancy.5,12 Texts were received, on average, 4 minutes after they were delivered (SD = 8 minutes), indicating that women were compliant with the text messaging protocol.
Salivary cortisol
Participants were asked to provide a saliva sample following each measure of momentary stress (16 times/participant). Thirty minutes after the “stress” text, women were sent another text message asking them to provide a saliva sample (passive drool) into a tube that had been provided to them at the study session and text “done” when the sample was complete. This information was used to confirm that samples were being collected as per study protocol. Saliva samples were completed on average 39 minutes after “stress” text. Salivary cortisol samples were then frozen at −80°C until they were analyzed in duplicate using immunoassay at Brandeis University (laboratory of Nicolas Rohleder, PhD). Intra-assay variability was 4.53% and inter-assay reliability was 11.4%. In all, 199 samples (80% completion rate) were assayed for salivary cortisol concentrations.
Statistical analyses
Descriptive statistics were conducted using SPSS v.20 software. Cortisol values were not significantly skewed and therefore were not log transformed (skewness and kurtosis <2). Independent samples t-tests and Chi square analyses were used to examine whether maltreatment groups differed on maternal characteristics, stress measures, and gestational length. Pearson correlations and linear regression analyses were performed to examine associations between momentary stress scores (averaged over 16 time points), average QIDS and PSS scores, and gestational length. We used hierarchical linear modeling software (HLM) 13 to examine within-person associations between each momentary stress measure and corresponding cortisol concentration (level-1), and whether associations differed by maternal childhood maltreatment history, QIDS or PSS score, or gestational length (level-2). Results were considered statistically significant if the p value fell below .05. Gestational age at each session and sampling time were considered time-varying covariates in HLM models to account for effects of GA and time of day on cortisol concentrations.
Results
Sample characteristics
Maternal characteristics by maltreatment group.
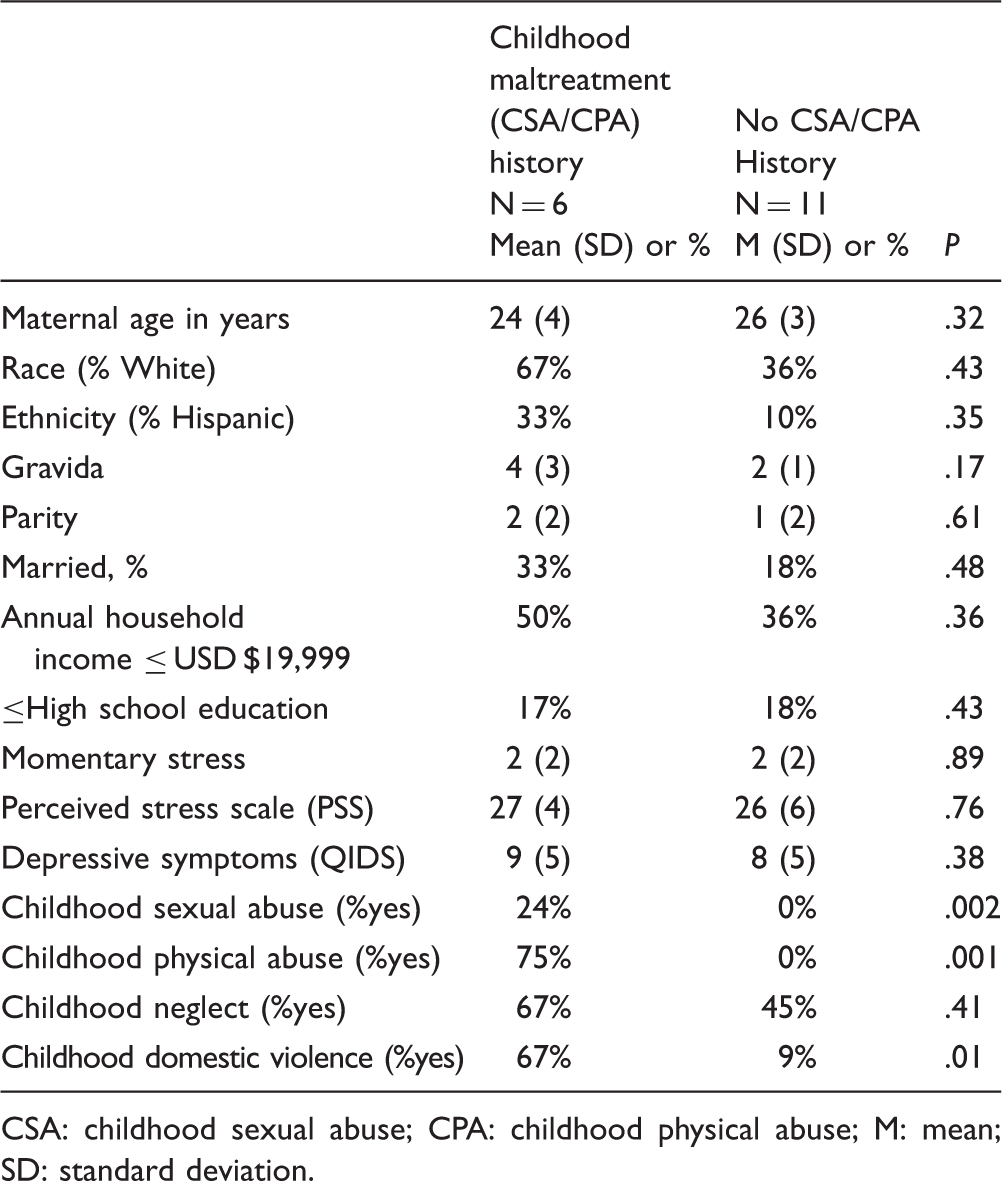
CSA: childhood sexual abuse; CPA: childhood physical abuse; M: mean; SD: standard deviation.
Average maternal symptoms of depression on the QIDS was 8 (SD = 5) (out of a possible score of 27) indicating that women were experiencing mild depressive symptoms in pregnancy, and average score on the PSS was 27 (SD = 5) (out of a possible score of 40), indicating that women were reporting high stress in pregnancy. Across the sixteen time points, participants reported an average momentary stress level of 2 (SD = 2, range: 0–8), indicating mild momentary stress. On average, infants in this sample were born at 39 weeks gestation (SD = 2, range: 34–41 weeks). One baby was spontaneously born preterm (<37 weeks; 7% of sample). Of the sample 24% experienced sexual abuse, 35% experienced physical abuse; 52% experienced neglect, 29% witnessed domestic violence, and 22% did not experience abuse. Of the sample, 35% (N = 6) reported experiencing childhood sexual abuse and/or contact physical abuse and were included in the maltreatment group.
To test for potential covariates, we examined whether average momentary stress scores or gestational length was associated with maternal characteristics. Higher momentary stress was only associated with higher parity (r = .60, p = .02). Parity was included as a covariate in subsequent analyses.
Maternal characteristics by maltreatment history
Childhood maltreatment groups did not significantly differ by maternal characteristics of age, race, ethnicity, parity, marital status, annual income, or education (p > .16). Childhood maltreatment groups did not significantly differ on reports of average PSS, QIDS, total momentary stress score, gestational diabetes mellitus, delivery mode (c-section vs. vaginal), or induction of labor (p > .34). Maltreatment groups did not significantly differ by gestational length (t = −.85, p = .42); therefore, we were not able to test whether momentary stress or cortisol mediated this association.
Maternal stress and gestational length
Average momentary stress scores were associated with shorter gestational length (β = −.69, p = .05); women who reported momentary stress scores in the highest quartile delivered 18 days sooner than women in the lowest quartile. Associations among PSS, QIDS, and gestational length were not significant (p > .77).
Associations between momentary stress and cortisol in pregnancy
We used HLM to examine within-person associations between momentary stress and corresponding cortisol concentrations. Momentary stress and cortisol were inversely associated (b = −.55, SE = .24, p = .04), such that, as momentary stress levels increased, corresponding cortisol concentrations decreased. This association was moderated by childhood maltreatment history (b = −.90, SE = .40, p = .04); as momentary stress increased, cortisol concentrations decreased for women with maltreatment history, whereas for women without maltreatment histories, as momentary stress increased, corresponding cortisol concentrations increased (see Figure 1). Associations between momentary stress and cortisol did not differ by gestational length (b = .01, SE = .02, p = .54), PSS (b = .03, SE = .04, p = .40), or QIDS score (b = .07, SE = .06, p = .25).
Associations among momentary stress and cortisol in pregnancy differ by childhood maltreatment history. CSA/CPA: childhood sexual abuse and/or physical abuse history. Note: Momentary stress scores were examined as a continuous variable. Low and high stress on the X axis of the figure correspond to 25th and 75th percentile of momentary stress scores.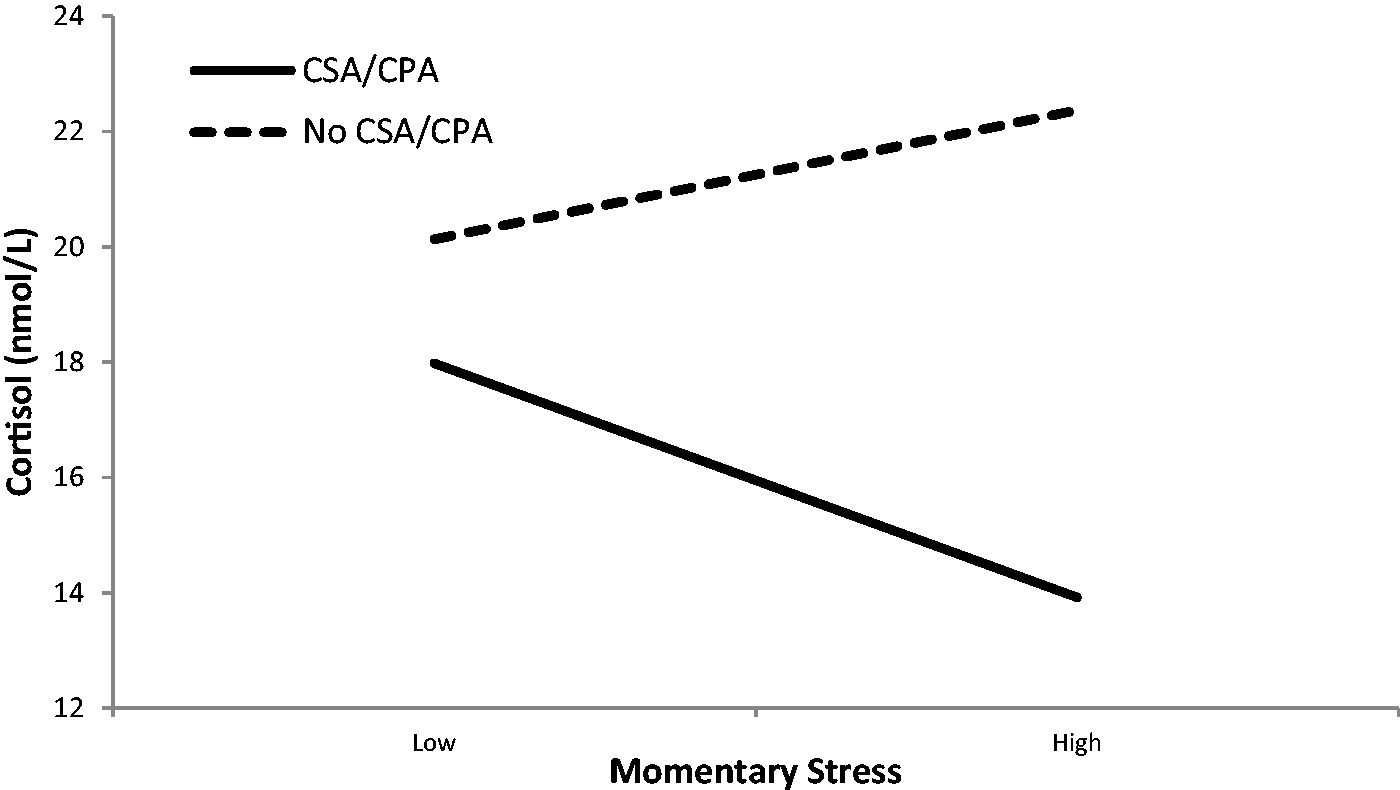
Discussion
This pilot study is the first, to our knowledge, to examine ecologically-valid perceptions of stress in pregnancy and corresponding cortisol levels among pregnant women with childhood maltreatment histories. Results from this study provide preliminary evidence that momentary stressful experiences, but not retrospective accounts of stress, may be significantly associated with shortened gestational length. Specifically, in this study, women who reported momentary stress levels in the highest quartile delivered approximately 18 days earlier than women with stress levels in the lowest quartile. We and others speculate that maternal stress signals may signal to the fetal compartment that the host environment is unsafe, triggering earlier onset of parturition. 14
These findings are in contrast to findings from Entringer et al. who utilized EMA methodology to collect momentary measures of affect and cortisol over pregnancy; they reported that negative affect was not associated with gestational length, but was associated with increased cortisol in pregnancy (5). We found a similar pattern of results among women without childhood maltreatment histories; however, among women with histories of childhood maltreatment, increased stress was associated with attenuated cortisol concentrations over pregnancy. Entringer et al. 5 did not report on the maltreatment history of the participants.
The observed lower cortisol concentrations in relation to higher momentary stress among maltreatment victims may represent dysregulation in the ability of the HPA axis to mount an adaptive physiological response to challenge. Previous research among non-pregnant individuals with childhood maltreatment histories has demonstrated a similar attenuation of basal HPA activity15,16 and attenuation of cortisol responses to laboratory-based stressors. 11 According to the attenuation hypothesis, 17 victims of childhood maltreatment demonstrate an initial period of heightened HPA activation following abuse, followed by HPA down-regulation and subsequent hypo-activity as an adaptive response to protect biological systems from the damaging effects of high levels of circulating cortisol. 18 More studies are needed that examine HPA activity over gestation among women with childhood maltreatment histories.
While results from this study are novel and contribute to the extant literature by indicating that momentary stress measures may be important in understanding how maternal psychological experiences impact gestational length among women with childhood maltreatment histories, findings should be interpreted in light of several limitations. First, our sample size was small and results are preliminary. These preliminary findings need to be followed up by a fully powered study with a larger sample. Second, given the high rates of maltreatment in our sample, our comparison group included some women who reported having experienced neglect and/or witnessed domestic violence. In the future it is important that studies include a comparison group with no maltreatment experience. Third, this sample was at low-risk for obstetric complications and therefore we may not have had the variability in gestational length to adequately examine associations between maltreatment history and PTB.
In conclusion, despite several limitations, results may have important implications for the development of stress management interventions aimed at reducing risk for preterm birth among women with childhood maltreatment histories. Such interventions could be tailored to a text-messaging format. However, findings are preliminary given the small sample size and the limited number of EMA assessments. Future larger studies are needed that utilize EMA methodology to collect a broader battery of stress and mood information among childhood maltreatment victims in order to further understand pathways to shortened gestational length.
Footnotes
Acknowledgements
The authors thank the women in the study for their participation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Miriam Hospital Foundation Lifespan Seed Grant to MHB and by NIDA grant R01DA031188 to LRS.
Ethical approval
This study was approved by Women and Infants Hospital and Lifespan Hospital Institutional Review Boards (Board Reference Number: 023512). All women provided written consent prior to their participation.
Guarantor
MB
Contributorship
MB was responsible for the literature review, data analysis, and writing the first draft of the manuscript. GB provided mentorship and guidance on the design of the pilot project and was involved in the writing and revising of the manuscript. CV-L provided significant assistance with data analyses and was involved in the writing and revising of the manuscript. LS is the principal investigator of the parent study. She was responsible for all aspects of study oversight of the parent study, provided mentorship on the pilot project, and was involved in the writing and revising of the manuscript.