
Abstract
The commercial availability of tests in the first trimester of pregnancy that predict the later development of pre-eclampsia has prompted considerable debate regarding their clinical utility and the degree to which they fulfil the longstanding principles of screening. Such tests have been shown to achieve detection rates for early pre-eclampsia (requiring delivery prior to 34 weeks) of over 90%, for a false positive rate of 10%. However, their capacity to predict later onset pre-eclampsia, which accounts for the bulk of the disease burden, is much more limited. The relatively few studies validating the performance of these tests in different populations have demonstrated significant variations in performance. Moreover, prospective research confirming that the administration of aspirin to those screened to be high risk reduces the incidence of pre-eclampsia is yet to be completed, and there may be harms in restricting aspirin therapy to this group, given its broader beneficial effect. In light of these limitations, further development of these tests is recommended prior to their introduction to clinical practice.
Introduction
The commercial availability of tests in the first trimester of pregnancy that predict the later development of pre-eclampsia has prompted considerable debate regarding their clinical utility and the degree to which they fulfil the longstanding principles of screening, first outlined by Wilson and Jungner. 1 The genesis of these tests, which combine maternal clinical factors, biophysical parameters and biomarkers, is inextricably interwoven with the development, implementation and performance of multiparametric screening strategies for Down syndrome, allowing useful parallels to be drawn in evaluating the former. 2 This review outlines strategies for pre-eclampsia screening and discusses their relative advantages and disadvantages. It highlights the limitations of currently available screening tests for pre-eclampsia, and concludes with a perspective on how such tests might evolve in the future.
Why screen for pre-eclampsia?
‘Routine’ antenatal investigations, such as maternal viral serology and fetal morphological ultrasonography, are generally considered to be screening tests on the grounds that they are offered universally to an asymptomatic population. However, most such tests seek to identify pathology that is already present, rather than predict disease that is yet to develop, as is strictly required for a screening test. As a complication that evolves later in pregnancy, and one which may be ameliorated by prophylactic therapy, pre-eclampsia is a worthy candidate for screening tests, with much research effort having been expended in this area as a result. The three commonest justifications for pre-eclampsia screening are that it would allow for:
The timely initiation of preventative agents, namely aspirin and calcium, Appropriate triaging to different models of antenatal care, and The recruitment of truly ‘high risk’ patients to trials of novel prophylactic therapies for pre-eclampsia.
3
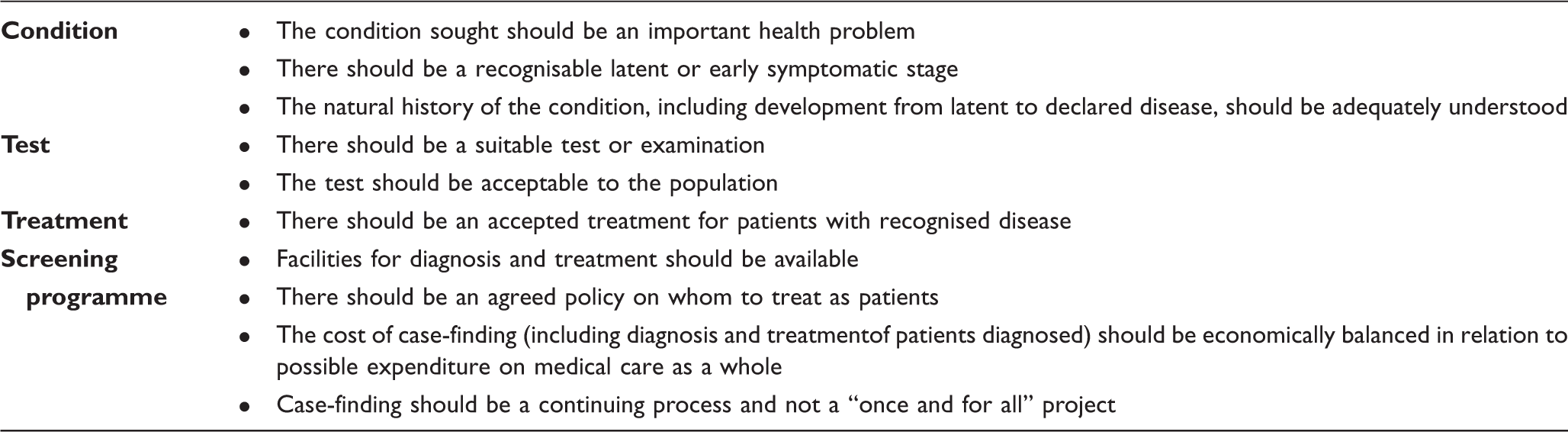
World health organisation principles of screening. 1
The performance of a screening test in predicting disease is related not only to its inherent characteristics – its sensitivity and specificity – but also to the background rate of the disease in the population to be tested (and thus the ‘pre-test probability’ of the disease occurring). Even highly sensitive and specific tests will have low positive predictive values (PPVs) if the disease in question is uncommon. In these circumstances, the vast majority of positive screening test results will be false positives, resulting in very large ‘numbers needed to screen’ to identify and potentially prevent one case of the disease. This is the situation for the general antenatal populations in which commercial pre-eclampsia screening tests are being promoted: although such tests are relatively sensitive and specific in detecting early onset pre-eclampsia, the low incidence of this complication in high-income countries (at around 0.4% 4 ) results in very low-PPVs.
Prophylactic therapies for pre-eclampsia
Despite broad consensus that aspirin will prevent the development of pre-eclampsia in some women, disagreement persists as to who should be thus treated. 5 The United States Preventive Services Taskforce, 6 the Canadian Hypertensive Disorders of Pregnancy Working Group, 7 and the UK National Institute for Health and Care Excellence 8 (inter alia) recommend that aspirin be given to pregnant women with a broad range of risk factors for pre-eclampsia, whereas the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy 9 recommends that it only be given to women with a history of pre-eclampsia requiring delivery prior to 34 weeks, and/or recurrent pre-eclampsia. There is also debate as to the time of day that aspirin should be taken, 10 its optimal dose, and the gestation at which it should be started.11–13 The Cochrane review of antiplatelet agents for the prevention of pre-eclampsia among women at high risk of developing this condition (46 trials, 32 891 women) identified a relative risk of 0.83 (95% CI 0.77–0.89), with a number needed to treat (NNT) of 72 to prevent one case of pre-eclampsia. 14 A subsequent meta-analysis of individual patient data from the perinatal antiplatelet review of international studies (PARIS) collaborators found a relative risk of 0.9 (95% CI 0.84–0.97), and a NNT of 114. 15 Neither of these studies demonstrated a difference in benefit relating to whether therapy was commenced before or after 20 weeks’ gestation, in contrast to a 2010 meta-analysis that suggested aspirin’s benefit is only achieved if treatment is started prior to 16 weeks. 12 However, this meta-analysis has significant limitations: studies in the pre-16-week subgroup were small and very few were negative (suggesting publication bias), and the results were confounded by significant systematic differences in the risk profile of the pre- and post-16-week subgroups, with a 20% rate of pre-eclampsia in the control arm of the former, but only 8% in that of the latter. 16 A subsequent meta-analysis identified benefit with aspirin commenced both before and after 16 weeks, but with greater benefit in the earlier group (RR of 0.47 vs. 0.78). 13
The only other agent shown to prevent pre-eclampsia is calcium. The Cochrane review identified a relative risk of 0.45 (95% CI 0.31 to 0.65) with calcium supplementation as against placebo (13 trials, 15,730 women). 17 Women at high risk derive greater benefit (five trials, 587 women: RR 0.22, 95% CI 0.12 to 0.42), as do those with low baseline calcium intake (eight trials, 10,678 women: RR 0.36, 95% CI 0.20 to 0.65).
Screening strategies
Maternal history
The most predictive risk factor for pre-eclampsia is a history of this disease in a previous pregnancy, which confers a relative risk of 7. 18 This is clearly of no use in nulliparae, who by definition cannot have had pre-eclampsia before, but who have a higher incidence of the disease. Using a range of other risk factors recommended by clinical guidelines, 8 such as age, body mass index, ethnicity and use of assisted reproductive technology, will predict a majority of cases of pre-eclampsia 19 – up to 89% of early (requiring delivery before 34 weeks) and 93% of late pre-eclampsia, at the cost of a significant ‘false positive’ rate of 64%. 20 A multivariate approach with a false positive rate (FPR) of 5% necessarily reduces the detection rates to 37% and 29% for early and late pre-eclampsia, respectively. 20
Maternal mean arterial pressure
In low-risk women, mean arterial pressure (MAP) is more sensitive in the prediction of pre-eclampsia than either the systolic or diastolic blood pressure alone. 21 MAP alone performs relatively poorly in predicting pre-eclampsia, achieving a 37.5% detection rate for a 10% FPR. 22 However, the combination of MAP and maternal factors in a multivariate model can predict 62.5% of all pre-eclampsia, for a 10% FPR. 22 This approach forms the basis of all subsequently developed screening strategies.
Uterine artery Doppler analysis
The predictive utility of Doppler ultrasound interrogation of a range of vascular beds has been evaluated, but the most commonly used is the uterine artery, which can conveniently be assessed at the time of the 12-week fetal scan. Increased resistance, typically assessed by the pulsatility index, may reflect suboptimal placentation, which has a well-established association with pre-eclampsia, particularly that which occurs at earlier gestations. 23 Assessment may be performed transabdominally or transvaginally, with different reference ranges for each approach. 24 The sensitivity and specificity of abnormal first trimester uterine artery flow-velocity waveforms for the prediction of pre-eclampsia were assessed in a recent large meta-analysis. 25 Although this test demonstrated relatively high specificities for both early onset (92.1% (95% CI 88.6–94.6%)) and all (93.4% (95% CI 90.4–95.5%)) pre-eclampsia, its sensitivity was limited (47.8% (95% CI 39–56.8%) for early onset disease, and 26.4% (95% CI 22.5–30.8%) for all pre-eclampsia), and in isolation it is insufficiently predictive to be of clinical utility.
Serum biomarkers
The predictive value of an extensive array of first trimester maternal serum markers has been evaluated, with new candidates regularly appearing in the literature. The breadth of such markers reflects the varied determinants and systemic effects of pre-eclampsia, which can be measured even before clinical disease is evident. Commonly studied serum biomarkers include pregnancy-associated plasma protein A (PaPP-A, which is also used in Down syndrome screening), placental growth factor (PlGF), and soluble fms-like tyrosine kinase 1 (sFlt-1). 26 No single serum biomarker performs adequately in the prediction of pre-eclampsia to be of clinical use.27,28 Similarly, combining serum biomarkers with maternal factors and blood pressure has not allowed the development of any sufficiently predictive algorithms, with a recent prospective study that employed this approach among low-risk nulliparae reporting a sensitivity of only 46.1% (95% CI 38.3–54.0) for the prediction of pre-eclampsia, for an 80% specificity. 29
Novel markers
The advent of the ‘–omics’, such as proteomics and metabolomics, may allow for more efficient generation of serum and urinary predictive biomarkers,30,31 although it remains unlikely that a single marker will be identified that can predict all forms of pre-eclampsia, given the heterogeneous nature of the disease.
Cell-free DNA screening is rapidly gaining traction in first trimester aneuploidy screening, given its very high specificity and sensitivity, especially for trisomy 21. 32 Early research suggests that the quantity of cell-free DNA, which is actually placental rather than fetal in origin, may predict pre-eclampsia, with 11 out of 13 studies in a recent systematic review recording this finding, although the heterogeneity of these studies precluded meta-analysis. 33 The clinical utility of this test for predicting pre-eclampsia remains to be determined.
The multiparametric approach
No single test currently performs adequately in the prediction of pre-eclampsia. However, multivariate analysis allows the development of multiparametric algorithms that combine a range of predictive tests to achieve improved disease detection rates at a lower false positive rate. This is analogous to the first trimester combined screening approach for aneuploidy, which incorporates maternal factors (such as age) with the fetal nuchal translucency and maternal serum levels of PaPP-A and beta-hCG. 34 Indeed, prior to the advent of cell-free DNA screening, multiparametric screening for pre-eclampsia may have represented a resource-efficient extension of aneuploidy screening regimens, although this potential efficiency does not by itself justify the clinical introduction of such testing, and does not negate the importance of the other principles of screening outlined earlier.
Detection rate (DR) of early pre-eclampsia at a 10% false positive rate using various multiparametric predictive models (reproduced from Khong SL et al. 24 ).

PlGF: placental growth factor; PAPP-A: pregnancy-associated plasma protein A; MAP: mean arterial pressure. *FPR of 5% in this study.
External validation of multiparametric models for the prediction of early pre-eclampsia (<34 weeks) (reproduced from Khong SL et al. 24 ).
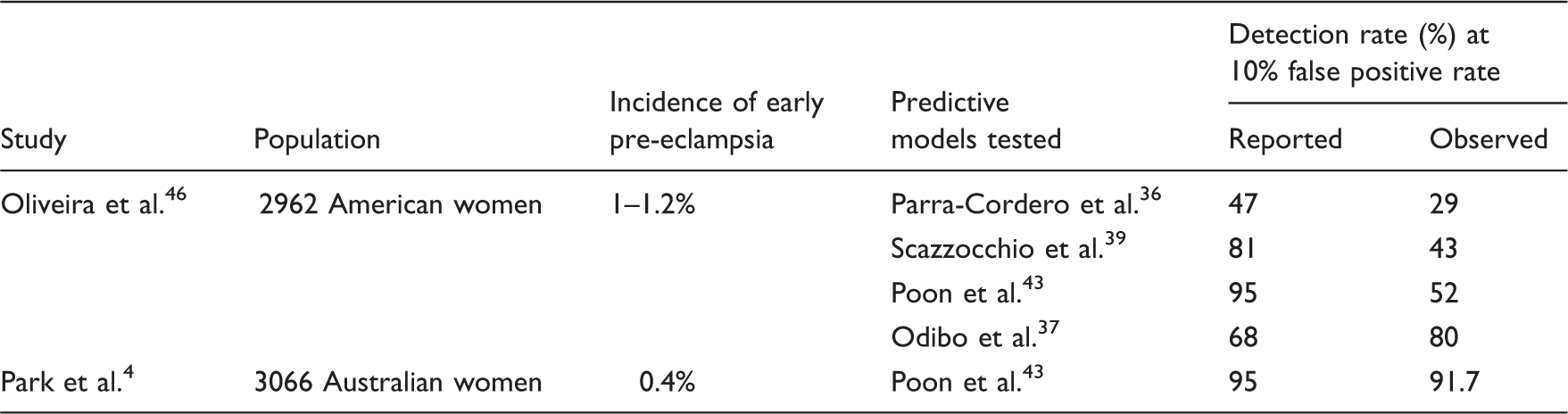
These potentially wide discrepancies highlight the importance of validating testing algorithms in particular populations, as algorithms are likely to be overfitted to the cohort in which they were initially developed, whereas validation studies reflect their ‘real world’ performance.
The effect of the administration of aspirin to women deemed high risk for pre-eclampsia by these screening tests was assessed in an Australian study that retrospectively compared the outcomes of a screened but untreated (‘observational’) cohort 4 with those of women in a subsequent ‘interventional’ cohort, who were screened and treated if at high risk. 47 This study demonstrated a reduction in the incidence of pre-eclampsia requiring delivery before 34 weeks from 3.65% to 0.38% (p < 0.01) among those deemed high risk by the screening algorithm. Of note, rates of aspirin use (if any) in the observational cohort were not reported, and compliance in the interventional group was not assessed.
Limitations of current screening tests
Although currently available multiparametric screening tests for pre-eclampsia show much promise, their limitations are such that numerous professional entities, including ACOG 48 and SOMANZ, 49 have advised against their clinical introduction. In addition to the variable performance of these tests in the limited validation studies performed to date (cf. Table 3), a wide range of other inadequacies has been identified, 50 mostly relating to the poor alignment of these tests with the principles of screening (cf. Table 1). 1
Scope of prediction
Despite being marketed as screening tests for pre-eclampsia in general, multiparametric tests only achieve adequate performance in the prediction of early onset pre-eclampsia requiring delivery prior to 34 weeks’ gestation. Although this subgroup of patients would generally be considered to have severe disease, and are certainly at significant risk of adverse maternal and neonatal outcomes, it comprises only a small proportion of the overall disease burden, most of which occurs at or near term.51,52 Later onset pre-eclampsia is generally of lesser neonatal concern, as it is not associated with fetal growth restriction. 53 In contrast, maternal risks are potentially substantial, with all nine Australian deaths from pre-eclampsia in the latest quinquennium having occurred postpartum in women who had delivered after 37 weeks. 54 Given the different placental pathophysiology that appears to underlie later onset pre-eclampsia, 55 predicting this spectrum of the disease may only be possible in the third trimester, 56 with screening at this gestation potentially allowing for stratification of subsequent antenatal care and thus improved management of those likely to develop pre-eclampsia. 52
The low incidence of pre-eclampsia requiring delivery by 34 weeks confers relatively low PPVs on tests that screen for this outcome (3.6% at an FPR of 10% in the Australian study 4 ), despite their reasonable detection rates. These low PPVs contribute significantly to recommendations that such screening tests not be introduced to clinical practice. 48
Practical impediments
A key component of multiparametric predictive tests for pre-eclampsia is Doppler analysis of the maternal uterine artery. This is a specialised sonographic technique, 57 results of which have been shown to vary significantly if the site of interrogation is only slightly distal to the internal cervical os. 58 Access to high-quality sonography is already challenging in many areas, and widespread availability of appropriately performed uterine artery Doppler studies is unlikely to be achievable.
Lack of RCT-level evidence of benefit
As noted earlier, there is clear evidence to support aspirin’s role in preventing a proportion of pre-eclampsia.14,15 Given the association between defective placentation and early onset pre-eclampsia, and the function aspirin likely plays in improving placentation in early pregnancy, it is probable that aspirin will prevent more early rather than late-onset disease. 13 What has not been established prospectively, however, is the extent to which screening tests will predict those patients in whom aspirin is effective in preventing pre-eclampsia. Although retrospective Australian data are encouraging in this respect, 47 prospective randomised studies will be required to assess the benefit of this approach. The ASPRE project (ISRCTN13633058), run by the Fetal Medicine Foundation in the UK, seeks to answer this question: 33,680 pregnancies will be screened to identify 3368 ‘high risk’ women, who will be offered randomisation to aspirin 150 mg or placebo. If 50% agree to participate, the 1684 participants will confer a power of 90% to identify a 50% reduction in pre-term pre-eclampsia. This project will allow analysis of the efficacy of the intervention, namely aspirin prophylaxis. It will not, however, demonstrate the efficacy of the overall screening program, 56 which in this context would require a comparison of outcomes between those randomised to receive the current standard of care – i.e. aspirin prescribed on the basis of risk factors for pre-eclampsia 6 – and those treated with aspirin following a high-risk screening test result. Such a trial would be difficult to perform, but would be necessary to define the true impact of these new tests.
Cost effectiveness
Economic arguments for pre-eclampsia screening are difficult to mount, given the low cost of its associated intervention, namely aspirin. It would be cheaper to treat everyone and test no-one, 59 but such an approach may not be compatible with the principle of primum non nocere, even if the risk of harm is negligible. Previous arguments regarding the economies of scale for combined pre-eclampsia and first trimester aneuploidy screening have been challenged by the paradigm shift of cell-free DNA screening for aneuploidy, which requires neither the maternal biochemistry nor the 12-week scan that comprise conventional first trimester aneuploidy screening tests (although there is significant value in the latter beyond screening for aneuploidy alone 60 ). Overall, the limited analyses that have been performed on pre-eclampsia screening strategies so far have not demonstrated consistent economic benefit, 61 although the identification of other, more expensive prophylactic agents may shift this balance. Similarly, it has been argued that pre-eclampsia screening tests would allow for an inversion of the ‘pyramid of care’, 62 resulting in a more efficient use of limited resources by reducing the number of antenatal visits for those deemed ‘low risk’. Although a worthy goal, this will not be achievable any time soon – leaving other obstetric concerns to one side, the poor performance of current screening tests in predicting later onset pre-eclampsia would continue to necessitate an increasing frequency of visits in the third trimester for all women.
Possible harms?
It has been suggested that receiving a ‘high risk’ pre-eclampsia screening result may lead to increased levels of maternal stress and anxiety. Although this certainly seems to be the case for Down syndrome screening, 63 qualitative evidence to date would suggest that the same is not true for pre-eclampsia. 64
The safety of not prescribing aspirin prophylaxis to women with a history of early onset pre-eclampsia but whose screening tests return low-risk results has not been established. As such, until further studies are performed, the only potential role for pre-eclampsia screening tests in this a priori high-risk population is the provision of reassurance to those few patients who will receive a low-risk screen result, rather than any alteration in management.
More broadly, there is the potential for pre-eclampsia screening tests to render some women ‘ineligible’ for antenatal aspirin therapy, even though it may be of benefit in reducing their risk of adverse perinatal outcomes other than pre-eclampsia. Aspirin demonstrates a modest but consistent effect in reducing rates of fetal growth restriction, pre-term birth, and perinatal death.12,15,65 There is substantial cross-over in the risk factors for these conditions and for pre-eclampsia, and the inherently high ‘false positive’ rate of any risk factor-based screening strategy for the latter 20 will maximise the chance that women at risk of these other complications will also receive aspirin. In contrast, the enhanced specificity of pre-eclampsia screening tests result in just over 10% of those screened (true and false positives combined) being labelled high risk and therefore prescribed aspirin prophylaxis. The extent to which pre-eclampsia screening tests also capture those at risk of other adverse perinatal outcomes has not been established, and although there will certainly be a degree of cross-over, it is unlikely to be absolute. As a result, pre-eclampsia screening may deny some women the potential benefit of aspirin, unless it is also prescribed on the basis of risk factors for these other adverse outcomes, which would in turn negate the major putative benefit of pre-eclampsia screening.
Future directions
The limitations of currently available multiparametric screening tests for pre-eclampsia render their clinical introduction difficult to justify, when risk factor-based screening will identify a significant majority of those destined to develop this complication. Taking a comprehensive history and performing a physical examination remain the cornerstones of clinical medicine, and do not require access to expensive, complex tests – an especially important consideration in this context given that the overwhelming burden of pre-eclampsia occurs in low-income countries.66–68 Aspirin is safe 69 and cheap, with perinatal benefits beyond the prevention of pre-eclampsia alone: promoting its widespread use for those at any risk of adverse perinatal outcome is likely to yield far greater benefits 70 than investing in current pre-eclampsia screening tests. This is not to suggest, however, that research in this domain should not continue. On the contrary, research to date has provided important insights into the pathophysiology of the early onset phenotype of pre-eclampsia, and the role aspirin plays in its prevention. Further study into the various phenotypes of this condition, 71 and appropriately targeted prophylactic strategies for each, will likely yield significant advances in the prevention of pre-eclampsia. 72 Such strategies must, however, be subjected to rigorous assessment against the principles of screening prior to their clinical introduction. Until then, our patients – extant and nascent – will best be served by a ‘back to basics’ approach that incorporates the meticulous application of current knowledge and evidence.
Footnotes
Acknowledgements
Tables 2 and 3 have been reproduced without modification from Khong SL et al.
24
(http://www.hindawi.com/journals/dm/2015/679730/), under the auspices of the Creative Commons Attribution License (![]() ).
).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author is supported by a Postgraduate Scholarship from the Australian National Health and Medical Research Council (APP1093639). His PhD research project is supported by grants from the Research Foundation of the Royal Australian and New Zealand College of Obstetricians and Gynaecologists, and from the Australasian Society for Ultrasound in Medicine.
Guarantor
SCK