
Abstract
Carcinoid tumours are rare slow growing tumours which arise from primitive neuroendocrine cells. The effect of the pregnant state on carcinoid tumours and vice versa remains unclear, as does the optimal management of carcinoid tumours during the pregnancy including labour. We report the rare case of a 36 year old primigravida woman with large bilateral pulmonary carcinoid tumours. The patient's disease was minimally symptomatic with no clinical suspicion of carcinoid syndrome. Under close observation, the pregnancy progressed well and the patient proceeded to a spontaneous vaginal delivery of a healthy child. We conduct the the first literature review in 30 years of all reported cases in this area and make suggestions as to assessment and monitoring of cases of carcinoid during pregnancy.
Case report
We report the case of the successful first pregnancy of a 36-year-old lady, notable for the presence of large bilateral pulmonary carcinoid. Five other reports of pulmonary carcinoid during pregnancy were found in the literature (1984–2014) with this case having more extensive disease and longer follow-up than other published reports in pregnancy.
The patient was referred to the obstetric medical department for co-management during her pregnancy. Carcinoid had been diagnosed incidentally three years earlier following an episode of pneumonia requiring inpatient treatment with intravenous antibiotics. Imaging had revealed a 4 cm mass in the left hilum and a 7 cm mass in the anterior right upper lobe causing complete obstruction of the bronchi and atelectasis (Figure 1). Bronchial washings stained positive for neuroendocrine markers (neuron-specific enolase (NSE), protein gene product 9.5 (PGP9.5), synaptophysin, chromogranin and CD56). Serum chromogranin A levels were significantly elevated at 62 U/L (reference range 0–17.2 U/L). There was no clinical suggestion of carcinoid syndrome and 5-hydroxyindoleacetic acid (5-HIAA) levels were in the normal range. Other than an elevated body mass index (BMI) and acne rosacea, her medical history was unremarkable.
Computerised tomography image of chest prior to pregnancy, showing bilateral pulmonary carcinoid tumours.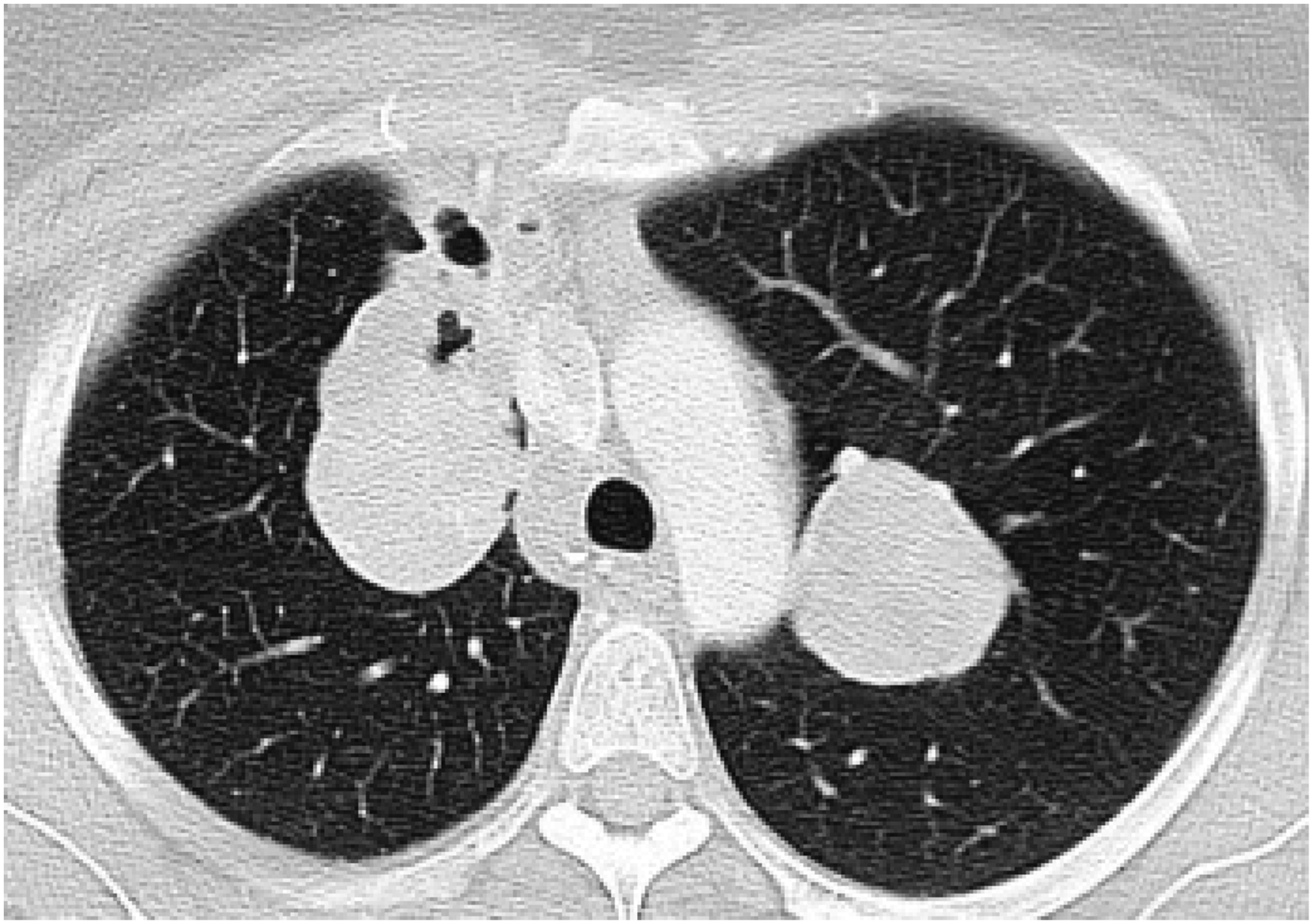
Clinically the patient's disease had been minimally symptomatic from the time of diagnosis, with a single episode of haemoptysis and occasional central chest discomfort on deep inspiration. Cardio-thoracic review concluded that surgery was not desirable because the extent of disease would require both a left pneumonectomy and right upper lobe resection. Bi-annual imaging did not reveal growth of the pulmonary lesions or the development of metastases or the development of carcinoid syndrome. Somatostatin analogue therapy was not indicated in the absence of carcinoid syndrome/symptoms or disease progression. Potential treatment with lutecium octreotate was also considered but not indicated in the absence of evidence of disease progression.
The patient did not report any symptoms at the initial obstetric medical review at 10 weeks’ gestation. On subsequent review at 15 weeks’ gestation, the patient did report mild shortness of breath. Clinical assessment at the time was unremarkable. An echocardiogram was performed at 20 weeks to exclude a cardiac cause for dyspnoea and was normal with an ejection fraction 62%, chromogranin A levels at 26 weeks and 32 weeks’ gestation were 76 and 89 U/L respectively (reference range 0–17.2 U/L), compared with 68 U/L two years prior with the rise being considered consistent with pregnancy rather than disease progression. 5-hydroxyindoleacetic acid (5-HIAA) levels were measured at 26 weeks (23 µmol/24 h, reference range <40 µmol/24 h), and 32 weeks (43 µmol/24 h).
Respiratory function tests were initially declined by the patient as she felt her symptoms were not severe enough to warrant this investigation. They were performed prior to the delivery and were normal. The patient's preference was for vaginal delivery, which was supported by treating clinicians. Spontaneous rupture of membranes occurred at 36 weeks, with a vacuum delivery of a healthy female under epidural anaesthesia. An octreotide infusion was not used, as there was no prior evidence of hormonal secretion. The patient was observed in the intensive care unit for 24 h of monitoring and discharged home after 48 h. The patient has now been followed for 12 months post-partum and her disease remains stable. At her next assessment, magnetic resonance imaging (MRI) showed a 10 × 11 × 13 mm solitary liver lesion and was non-specific. Nuclear imaging with (fluorodopa (FDOPA) positron emission tomography scan (PET) was done and did not show abnormal uptake prompting a plan for observation. Further imaging at five years post-pregnancy showed very minimal progress of her disease and she remained asymptomatic.
Discussion
Carcinoid tumours are rare slow growing tumours which arise from primitive neuroendocrine cells. The most common sites for growth are the gastro-intestinal tract (66%) and the pulmonary system (10%). The incidence of the condition has been reported at approximately 2.0 to 3.0 per 100,000 using national registry data in Sweden, the United Kingdom and the United States, but may be rising. 1 The sex distribution is approximately equal and diagnosis is most often made in those aged between 55 and 65. Ten per cent of cases are associated with Multiple Endocrine Neoplasia – Type 1(MEN1). MEN1 is an autosomal dominant disease characterized by parathyroid, pancreatic islet and anterior pituitary tumours, but may also cause other tumours such as adrenocortical and carcinoid tumours. 2
Patients with pulmonary carcinoid may be asymptomatic and be incidentally diagnosed or present with obstructive pneumonia, pain, shortness of breath or cough. Less than 10% of patients with carcinoid tumours present or develop carcinoid syndrome which is associated with flushing, diarrhoea, vomiting, abdominal cramps and bronchoconstriction. Diagnosis in pregnancy can be made more challenging by attribution of symptoms such as shortness of breath and vomiting to physiological changes of pregnancy rather than pathology. Furthermore, normal pregnancy is associated with increased levels of the key carcinoid tumour marker chromogranin A, partly due to a contribution from the placenta, an organ with neuroendocrine activity. 3 Decisions regarding imaging and biopsy procedures may be influenced by pregnancy, with a desire to minimise exposure to ionising radiation and procedural risk. In the absence of a histological sample, clinicians will have to consider all features of symptomatic, biochemical and radiological evidence in making a diagnosis.
Reported survival rates vary depend on whether the disease is localised or metastatic, with recent data reporting 80 to 95% survival at five years post-diagnosis.4–7 Surgical resection may be curative and is the treatment of choice where possible. Surgery (and required anaesthesia) during pregnancy is not associated with any increase in fetal malformations but is associated with an increase in fetal loss rates. Risks will vary according to trimester and type of surgery. 8 Somatostatin analogues such as octreotide and lanreotide and, more rarely, external beam radiotherapy are also used depending on symptomatology and location. The former therapy is generally recommended in carcinoid syndrome with recent evidence suggesting growth restraint with longer time to progression.9,10 However, the safety of octreotide in pregnancy is yet to be established with conflicting case reports published with both poor and positive outcomes.11–13 Both the long- and short-acting forms cross the placental barrier, with data indicating short acting octreotide is found in lower concentrations in umbilical cord serum, amniotic fluid, and newborn serum. Hepatic artery embolisation and radiofrequency ablation (RFA) are potential options for patients with liver lesions, with a median survival of five years. 14 Both treatments have been utilised in pregnancy, though RFA is best avoided during organogenesis.15,16 Treatments which are yet to develop a strong evidence base include inhibition of mTOR (mechanistic target of rapamycin) for non-functioning pancreatic, gastrointestinal and lung neuro-endocrine tumours. Radioisotope therapy with lutecium octreotate has been used in patients with progressive disease and has a growing evidence base.17,18
Summary of cases of carcinoid in pregnancy by site and other features.
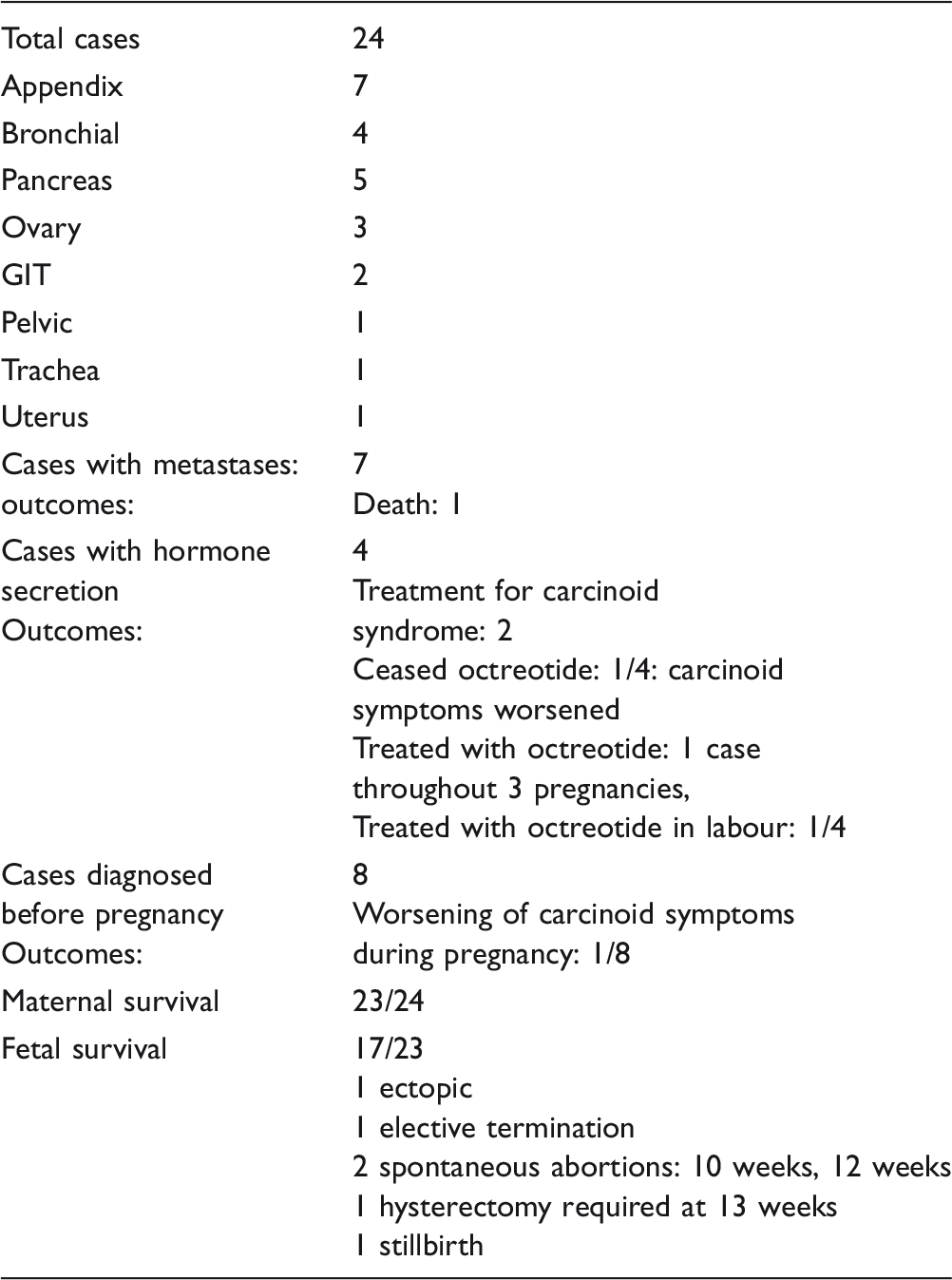
The effect of carcinoid upon pregnancy is not clear. Given the array of hormones associated with carcinoids such as serotonin, adrenocorticotropic hormone and cortisol, it is plausible that carcinoids could have an effect on smooth muscle (including uterine) function and placental growth. Whilst the effect of appendiceal carcinoids was not noted to be significant in Durkin’s series, primary uterine and metastatic hepatic carcinoid disease were associated with fetal loss. In our review of the 26 subsequently reported cases, five cases resulted in fetal loss and two in early delivery. Jurica et al.’s report 21 was of a small appendiceal tumour and a 21-week delivery of a 315 g infant; Chlamydia infection was thought to be the cause of fetal demise rather than carcinoid tumour. Gilboa et al. reported a case of spontaneous first trimester miscarriage five days after surgery for an appendectomy which resulted in a histological diagnosis of carcinoid. 22 In an ectopic pregnancy, Thompson and Hawe reported a case of dual pathology of acute inflammation and appendiceal carcinoid. 23 Poiana et al. 24 reported a case of appendiceal carcinoid, where the patient decided upon an elective termination of pregnancy.
In one of four reported cases of secretory carcinoid, Pistilli et al. reported that a patient suffered a spontaneous late first trimester miscarriage of an unplanned pregnancy after previously receiving six cycles of radioisotope therapy for an ovarian carcinoid with hepatic metastases. 25 Abraham et al. 26 reported a case of pancreatic carcinoid with PTHrP secretion presenting with hypercaclaemic crisis. The baby was delivered at 29 weeks and noted to suffer from hypercalaemia followed by hypocalcaemia requiring calcium supplementation for a month. Mild asymmetric cerebral palsy was noted at follow-up, attributed to prematurity. The mother underwent laparotomy for removal of the mass and survived the pregnancy. Yamamoto et al.’s 27 case of bronchial carcinoid also presented at 29 weeks with massive haemoptysis requiring emergency caesarean section and then resection of the tumour and tracheal anastomosis. Cornell and Chhajed reported separate cases of pulmonary carcinoid diagnosed close to term (36 and 38 weeks, respectively).28,29 Both cases were successfully managed by caesarean section and then surgical intervention to remove the carcinoid tumour.
The effect of pregnancy upon carcinoid tumour progression is also unclear. Only eight cases were diagnosed prior to pregnancy, and with the possible exception of the case reported by Le where the patient self-ceased therapy, 30 no case reported significant disease progression. This stability was evident in all three cases of bronchial carcinoid diagnosed prior to pregnancy. Sewpaul et al. reported a case of spontaneous regression of a pelvic carcinoid, cautiously postulating that changes to B and T cell cytotoxity during pregnancy could be a potential mechanism. 31 Limited weight can be put on these cases, as it may be that small carcinoids grow during pregnancy and thus present during gestation as per the majority of reported cases. Complicating this issue further is the fact that most women have significant contact with health professionals during pregnancy which allows scope for investigation of pre-existing but previously uninvestigated stable symptomatology. Diagnosis during pregnancy in such cases may have no relationship with disease progression. Interestingly, the majority of seven cases of metastatic disease did not have adverse outcomes. In one case of extensive metastatic disease, the mother passed away from meningeal carcinomastosis.
Anaesthetic reports demonstrate the potential management option of octreotide that may assist in a successful and safe delivery for secretory tumours, though this was not necessary in our case. 30 However, despite the extent of disease in our case, the pulmonary carcinoid remained stable during and after pregnancy.
Clinical details of cases of carcinoid in pregnancy.

Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Written patient consent was obtained for publication.
Guarantor
DK.
Contributorship
DK and MC drafted the report. NF, DW and KL reviewed and provided references.