
Abstract
Spontaneous coronary artery dissection is a rare but important cause of acute coronary syndrome. Its relevance for women during the puerperium mandates awareness and understanding amongst obstetric healthcare professionals. The aetiology of the increased risk in pregnancy has not been fully elucidated, but include medial eosinophilic angitis, pregnancy-induced degeneration of collagen in conjunction with the stresses of parturition, and rupture of the vasa vasorum. The risk of mortality necessitates prompt diagnosis, usually by angiography. There is no one-size-fits-all treatment; management must be individualised according to haemodynamic status and affected vessel(s) and includes conservative management, percutaneous coronary intervention, or bypass grafting. Recovery complications include extension of the haematoma or false lumen, valvular pathology secondary to ischaemia, and sudden cardiac death. Close post-operative surveillance is mandatory. We present a 41-year-old lady with post-partum spontaneous coronary artery dissection, complicated by ischaemic papillary rupture and mitral regurgitation requiring valve replacement. Additionally, we present a literature review, including guidance on management and critical analysis of potential complications.
Introduction
Spontaneous coronary artery dissection (SCAD) is a rare but important cause of acute coronary syndrome (ACS), commonly affecting young females. Acute myocardial infarction complicates one in 16,000 pregnancies, and one in four of these will be SCAD. 1 Pregnancy-related SCAD occurs most commonly during the peripartum period, mostly affecting older and multiparous pregnant women. 2 The condition can lead to unstable angina, acute myocardial infarction, and sudden death. As the patients are often relatively young without any risk factors for coronary artery disease, the diagnosis may occasionally be overlooked.
Modern case series have a low risk of mortality 3 and there are a number of reported cases with successful medical and surgical intervention.
The cause of spontaneous dissection remains uncertain but theories include a medial eosinophilic angitis, pregnancy-induced degeneration of collagen in conjunction with the stresses of parturition, and rupture of the vasa vasorum.1,2,4
Having a high index of suspicion for women presenting with chest pain during pregnancy or post-partum enables prompt diagnosis and early involvement of cardiology specialists. The majority of SCAD patients can be safely managed conservatively, although a small proportion will require percutaneous coronary angioplasty or bypass grafting. 5
Case presentation
We present the case of a 41-year-old female, whose postnatal course was complicated by SCAD, ischaemic papillary muscle rupture, and severe mitral regurgitation, necessitating mechanical valve replacement.
A 41-year-old Afro-Caribbean female with spontaneously conceived mono-chorionic diamniotic twins presented to a District General Hospital at 36 weeks’ gestation with reduced fetal movements. She had an uncomplicated pregnancy and was booked for elective caesarean section at 36+5 gestation. She was Gravida 3 Para 1 and had a previous elective caesarean section following laparoscopic myomectomy and a laparoscopic salpingectomy for ectopic pregnancy. Past medical history was relevant for sickle cell trait and a microprolactinoma which was managed conservatively with cabergoline prior to pregnancy. Of note, she was an ex-smoker.
Her caesarean section was expedited due to concern about reduced fetal movements. Intra-operative blood loss was 600 ml and she was anaemic at the time of discharge with haemoglobin of 8.6 g/dl (9.8 pre-operatively). Her post-operative course was otherwise unremarkable and she was discharged home on day 4.
Two weeks later, she presented to the Accident and Emergency Department complaining of crushing central chest pain radiating to her back. A CT angiogram of her aorta was arranged, which excluded aortic dissection. Her ECG showed dynamic lateral t-wave inversion, and her troponin I was 460 ng/l. She had a trans-thoracic echocardiogram (TTE) which showed no obvious regional wall motion abnormalities and normal valvular and left ventricular function. She was started on ACS protocol including 75 mg aspirin, 600 mg clopidogrel, 2.5 mg fondaparinux and glyceryl trinitrate (GTN) infusion, and intravenous morphine for symptom relief. The following morning, she had a coronary angiogram, which showed a dissection of the circumflex artery from its origin to the trifurcation of the distal obtuse marginal artery. Intravascular ultrasound confirmed no evidence of coronary artery disease, and therefore she was diagnosed with a spontaneous coronary dissection, which was treated with a drug-eluting stent. Her post-procedure course was complicated by pyrexia, which spontaneously resolved. She was discharged home the following day on dual anti-platelet therapy and statin therapy was not recommended in the absence of atherosclerotic coronary artery disease.
She re-presented to hospital two days later with pyrexia, cough productive of pink frothy sputum, dyspnoea, and orthopnoea. TTE showed severe mitral regurgitation and papillary muscle rupture, which was thought to be ischaemic in nature. Chest X-ray revealed a right pleural effusion and right lower lobe consolidation. Whilst awaiting surgery, she was continued on antibiotics for a hospital-acquired pneumonia, aspirin, low molecular weight heparin, and a furosemide infusion. The GTN infusion and clopidogrel were stopped.
After close monitoring in intensive care, six days after re-presenting, she underwent mitral valve replacement and coronary artery bypass graft. The operative findings included severe mitral regurgitation secondary to ruptured posteromedial papillary muscle head, extensive infarction of residual posteromedial papillary muscle, dilated right ventricle and right ventricle outflow tract, and left ventricular dysfunction. A single coronary artery bypass graft was performed with a saphenous vein graft to the obtuse marginal artery. A 29 mm St. Jude Masters mechanical mitral valve prosthesis was implanted. Trans-oesophageal echocardiogram confirmed satisfactory placement with no paravalvular leak.
Post-operative recovery was slow due to fluid overload and bilateral pleural effusions, which were treated conservatively with diuretics. In view of the mechanical mitral valve, she was commenced on warfarin with a target INR of 2.5–3.5 in addition to furosemide, bisoprolol, atorvastatin, and clopidogrel. She made a slow and steady recovery and was discharged home with community nursing input.
Six months post-cardiac surgery she continues to do well and has had no further cardiac problems, although TTE demonstrated a reduced left ventricular ejection fraction of 40%. She was started on the progesterone-only pill for contraception, with a view to changing to a progesterone implant as a more effective long-acting contraceptive.
Coronary angiography and percutaneous coronary intervention with a drug eluting stent. (a) Coronary angiography shows an occluded intermediate artery; (b) An angioplasty wire is placed in the distal intermediate with partial restoration of flow; (c) A stent is placed in position to treat the site of occlusion; (d) Angiographic appearance after stent implantation.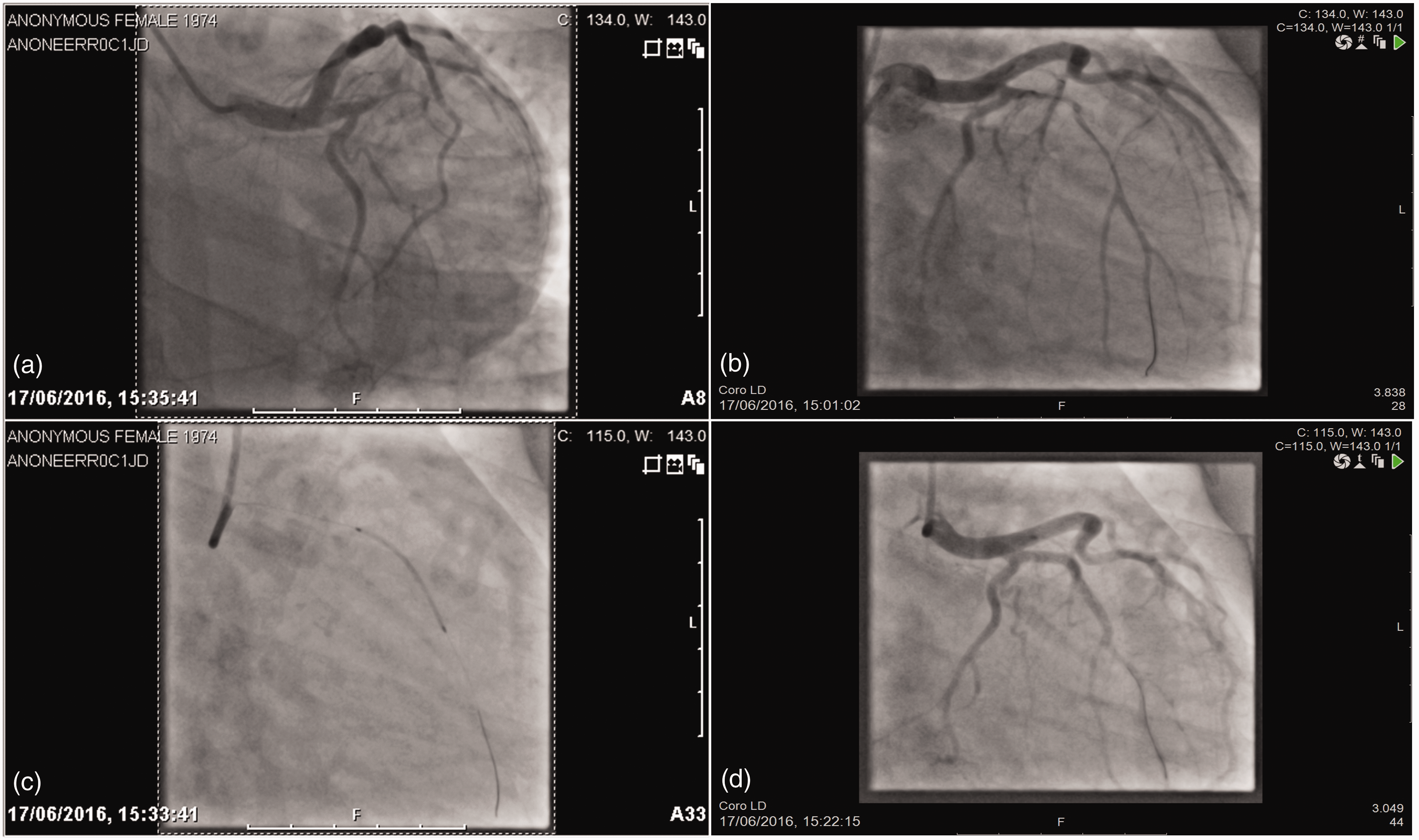
Discussion
SCAD is a rare condition where a false lumen is created due to non-traumatic or non-iatrogenic separation of the coronary artery walls. 6 SCAD has a significant mortality rate between 1 and 5%3,5,7 at presentation. Previously it had been thought that a third occur in women during the peripartum period8–10 although more recent studies have suggested that the proportion is as low as 2.4% of cases. 7 This has been attributed to advances in medical imaging and increasing awareness of the disease: cases are now being reported ante-mortem rather than post-mortem. 7
SCAD can be primary or secondary trauma during angiography.
The condition was first identified in 1931 during the autopsy of a 42-year-old woman who died after presenting with chest pain. 11 Since then about 1500 cases of SCAD have been documented. 3 The overall incidence of SCAD in angiographic series ranges from 0.28 to 1.1%.12,13 Commonly it involves a single coronary artery affecting the left anterior descending artery in 48–75% of cases, the right coronary artery in ∼20%, left circumflex in 4–35%, and the left main coronary artery in <1%.3,14,15 Multivessel SCAD is extremely rare, scantily recorded, and associated with high mortality rate.14,16 Apart from pregnancy-related SCAD, other factors linked with SCAD are sexual intercourse; vigorous exercise; isolated fibromuscular dysplasia; cocaine abuse; cyclosporine; combined oral contraceptive pill; recent chest trauma; Marfan and Ehlers–Danlos syndromes; and autoimmune diseases such as Kawasaki, systemic lupus erythematosus, and rheumatoid arthritis.1,16
Pregnancy-related coronary artery dissection is not typically connected with classic risk factors seen in coronary disease such as arterial hypertension, smoking, hyperlipidaemia, and diabetes, but mainly associated with multiparity and presumed changes to the arterial wall composition. Progesterone weakens the arterial walls by altering elastic fibre integrity, collagen synthesis, and fragmentation of reticular fibres resulting in a suboptimal composition of the tunica media. 7 Oestrogen both enhances the release of matrix metalloproteinase and induces a hypercoagulable state, and these factors with simultaneously increased cardiac output (up to 50% during pregnancy) and increased intraabdominal pressure are thought to be the cause of SCAD in pregnancy.1,17,18 Therefore, even patients with no risk factors of cardiac disease but reporting chest pain in pregnancy should have a low threshold to be investigated.
A relevant alternate hypothesis postulates that increased relaxin in pregnancy may play a role, either by blunting vasoconstriction through inhibition of endothelin-1, or by direct chronotropic and inotropic effects mediated by relaxin receptors.4,19 This increase in cardiac chronotropy and inotropy can lead to increased risk of coronary dissection. In addition, increased blood volume is further thought to predispose the patient to coronary artery dissection. These changes would potentially be exaggerated in a twin gestation.
Other theories regarding mechanisms of dissection include rupture of an atherosclerotic plaque or the vasa vasorum, disorders of the underlying connective tissue, and cystic medial necrosis. 2 Many cases occur in patients with no known risk factors and are seemingly idiopathic, although with improved assessment, this is becoming a smaller proportion of cases.7,20
The diagnosis of SCAD can be made by coronary angiography in most cases; however, using this technique alone, the true incidence of SCAD is likely to be underestimated and visualisation of the wall integrity and lumen is often needed. 21 Intravascular ultrasound is a complementary technique that can be used in the diagnosis, assessment, and treatment of coronary dissection. This technique can distinguish atherosclerotic stenosis from intramural haematoma, detect the medial dissection, false lumen, true lumen, and if present, the intimal flap. 13 Optical coherence tomography and multi-detector computed tomography coronary angiography have also been used in the diagnosis and follow-up of SCAD.22,23
The management of SCAD should be individualised to the patient’s presentation including, haemodynamic stability, site of dissection, number of vessels involved, and coronary flow status. 24 It has been documented in many studies that conservative treatment in haemodynamically stable patients is successful and should be preferred due to spontaneous healing of the dissection. 25
Rogowski et al. found that conservative management had superior results to PCI. Studies by Tweet et al., 23 Vijayaraghavan et al., 1 and Lettieri et al. 26 have all supported this recommendation. These studies have shown that success rates of PCI are less favourable due to extending the dissection, need for restenosis, catheter-induced dissections, and abrupt closure of the vessel after stenting. 5 Despite this, it is well documented in complex cases with refractory or ongoing ischaemia and/or atypical anatomy that revascularisation is the preferable first-line treatment. 27
Supportive medical treatment involves anticoagulation with aspirin, heparin, antiplatelet therapy, and a beta-blocker. Following heparin, the combination of acetylsalicylic acid and clopidogrel may be preferable to monotherapy. 28 The benefit of P2Y12 antagonists (prasugrel and ticagrelor) in SCAD is still unclear and therefore not routinely used. 7
In cases of haemodynamic instability, multiple vessel involvement, or large areas of myocardial compromise, PCI and coronary artery bypass grafting should be considered. 25 Decision making on procedural choice is complex and should be guided by clinical context and angiographic findings on a case-by-case basis. Drug-eluting stents are often used and the length often surpasses the dissection by 5–10 mm both proximally and distally in an attempt to overcome these possible complications. 1 Further complications include failure to ensure the guide wire is sited in the true lumen, catheter-induced dissections, and abrupt vessel closure after stenting. 5
Due to the risk of extension of a coronary haematoma and worsening of coronary spasm by vascular lumen compression, thrombolysis is not recommended. 29 Likewise, glycoprotein IIb/IIIa inhibitors are also contraindicated.
SCAD patients should receive supportive counselling as depression and anxiety are common with incidence as high as 37%. 23 Discussions should also take place in the follow-up pathway regarding the risks involved in future pregnancies should this be applicable. 23 Our patient does not plan to have any other children and indeed we would advise against further pregnancies as this would be extremely high risk in view of her residual impaired cardiac function.
In summary, the patient in this case had few cardiac risk factors, and yet she presented with SCAD complicated by myocardial infarction and subsequent ischaemic papillary muscle rupture. This highlights the importance of a high level of suspicion of SCAD in post-partum women, as well as appropriate management of SCAD, including monitoring for complications. 5
Conclusion
SCAD is a rare but serious cause of ACS, which is associated with pregnancy. In the peripartum period, SCAD should be included in the differential diagnosis in women presenting with signs and symptoms of acute coronary syndrome, even in the absence of risk factors. Prompt invasive diagnostic imaging will confirm the diagnosis of SCAD and determine optimal treatment. Close surveillance must be maintained in order to identify post-procedure complications, as in the case presented.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
MG.
Contributorship
MG and FT were involved in conception of this case report and literature search following the care of the involved patient and prompting the paper to be created. AH, FT, and CO were involved in data collection for the case report, which was written by AH and FT. FT, CO, AF, and DP performed the literature review. FT, AH, and DP edited the case report and literature review and wrote the introduction, as well as creating the initial draft of the article. Final approval of the article was a joint contribution between all listed authors.