
Abstract
The association of granulomatosis with polyangiitis and pregnancy is rare and therapeutic options are limited by the risk of teratogenicity and fetotoxicity. There is a paucity of published literature to guide clinical decision-making in these cases. We report the case of a 26-year-old woman with no medical history who presented at 21 weeks of gestation with a bilateral sudden loss of hearing and erosive rhinitis. The diagnosis of granulomatosis with polyangiitis was confirmed radiologically and biologically. Corticosteroids were not enough to stabilize the disease and she received intravenous immunoglobulins with remission. A successful delivery of a healthy male newborn was done at 36 weeks. A review of all published literature on granulomatosis with polyangiitis in pregnancy between 1970 and 2017 is presented.
Introduction
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis is a group of diseases characterized by destruction and inflammation of small vessels. This group includes microscopic polyangiitis (MPA), granulomatosis with polyangiitis (GPA) (previously known as Wegener’s granulomatosis) and eosinophilic granulomatosis with polyangiitis (EGPA) according to the Chapel Hill nomenclature. 1
GPA is more frequent in the fifth and the seventh decade and therefore rarely encountered in women of reproductive age. 2 It can manifest as a systemic disease with head and neck symptoms (nose stuffiness, rhinorrhea, sinusitis, otitis, tracheitis), pulmonary (bloody sputum, cough, dyspnea) and renal symptoms (hematuria, renal insufficiency). 2 However, in 30% of GPA, the manifestations are confined to the upper respiratory tract and have a good prognosis. 2
Untreated GPA has a mortality at one year of 70%. 3 With treatment, remission is obtained in more than 80% of cases. Even though relapses are frequent (50%), the survival rate is currently 75% at 10-year follow-up. 3 The treatment involves corticosteroids alone when the disease is limited to the upper respiratory tract. 3 In other cases, it is standard practice to combine corticosteroids with an immunosuppressant such as cyclophosphamide, rituximab and azathioprine, but intravenous immunoglobulins (IVIgs) can also be used.
The association of GPA and pregnancy is rare. 4 Several case reports have been published since 1970 reporting the new onset of disease during pregnancy. Herein, we report the case of a young woman in whom the disease was diagnosed during the second trimester, accompanied by a review of the literature to date.
We aim to define the main characteristics of GPA and its effect on pregnancy and vice versa. We also briefly examine reported treatments and their outcomes as a guide to future management.
Methods
We reviewed cases of GPA in pregnancy published from 1970 to 2017, including all those identified using hand searching of key journals; electronic searching of main databases especially Pubmed, including the use of free-text, index terms and named author; and reference scanning. We included women who met the diagnostic definition of GPA by either the American College of Rheumatology (ACR) criteria 1990 (Table 1) 5 and/or the Chapel Hill nomenclature. 1 We retrospectively analyzed baseline patient characteristics, including age and obstetric history as well as the initial clinical manifestations, severity as defined by the Birmingham Vasculitis Activity Score (BVAS), 6 and initial treatment of GPA.
American College of Rheumatology 1990 criteria for classification of granulomatosis with polyangiitis. 5

Every new manifestation of GPA in pregnancy was considered a flare. Information was collected on the timing, clinical presentation, and specific treatment of any flare.
Cases which did not result in a live birth were divided into four groups:
Termination of pregnancy in the first trimester on the grounds of maternal health Miscarriage before 12 weeks of gestation Late miscarriage between 12 and 21 weeks of gestation Stillbirth after 21 weeks of gestation
A pregnancy outcome was considered unfavorable when there was fetal loss (miscarriage, late miscarriage or stillbirth) or premature live birth (before 35 weeks of gestation). Preeclampsia was defined as the association of gestational hypertension and significant proteinuria (more than 0.3 g/24 h). A newborn was considered small for gestational age when birth weight was under the 10th percentile for gestational age according to Fenton preterm growth chart. 7
Case report
A 26-year-old Caucasian woman in her first pregnancy presented at 21 weeks of gestation. She complained of bilateral sudden hearing loss which was initially considered to be due to otitis media. She later developed an erosive rhinitis. Both manifestations were refractory to treatment which included antibiotics and local anti-inflammatory agents.
She also described inflammatory arthralgia of her wrists with diffuse myalgia, paresthesia of the legs and weight loss of 3 kg in two weeks. Her clinical examination was otherwise normal. She had no significant medical history.
Laboratory results were as follows: white blood cell count 12.7 g/l with 88.8% neutrophils; hemoglobin 88 g/l; hematocrit 28%; platelet count 336 × 109/l. No proteinuria was present on urinalysis and no red blood cells or casts were seen on urine microscopy. The serum chemistry revealed normal electrolytes (urea 3.3 mmol/l (1.18 mg/dl), creatinine 35 µmol/l, C-reactive protein 64 mg/l). Concurrently, indirect immunofluorescence assays showed positive classic antineutrophil cytoplasmic antibody (c-ANCA). Enzyme-linked immunosorbent assay (ELISA) showed the proteinase 3 level (PR3) was 176 IU (normal < 20 IU). Sputum culture was negative for mycobacteria along with a negative intradermal reaction and negative blood cultures. Thoracic computed tomography done at 25 weeks demonstrated numerous bilateral nodular densities without evidence of alveolar hemorrhage (Figure 1). Electromyography was normal.

Thoracic computed tomography showing multiple bilateral nodular cavitating lesions.
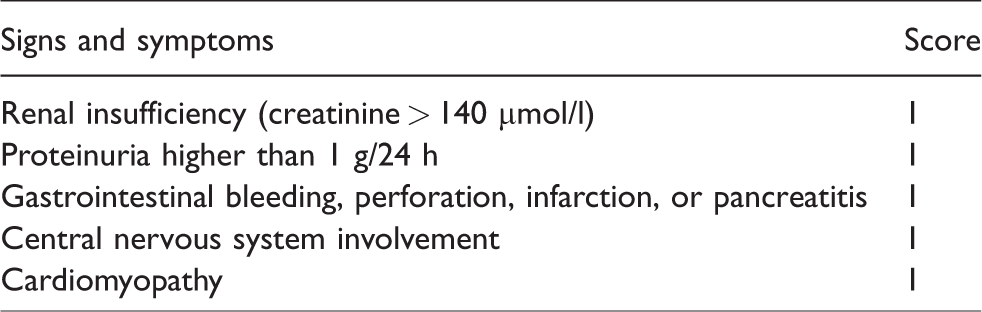
GPA was diagnosed based on clinical, biological and radiological evidence. A biopsy was not done. As she had a Five Factor score (FFS) (Table 2) 8 of zero with no serious manifestations, oral prednisone was started at a dose of 1 mg/kg. Azathioprine is a steroid-sparing agent that can be used in pregnancy, but it is not indicated to induce remission. It was decided to avoid rituximab until after delivery to avoid decrease in fetal lymphoid tissue B-cells and immunosuppression. 9 The patient’s condition improved remarkably after the initiation of corticosteroids. However, a relapse of the upper respiratory tract symptoms occurred at 28 weeks after the dose was reduced to 25 mg per day. Oral prednisolone was started again at 1 mg/kg (60 mg per day) with no improvement and IVIg 2 g/kg over four days was initiated. A further marked improvement of the symptoms was seen 48 h after the induction therapy and a slow tapering of corticosteroids was started again. The patient developed gestational diabetes mellitus controlled by dietary modification. The remainder of the pregnancy was uncomplicated and a healthy infant weighing 2300 g (>25th percentile) was delivered vaginally at 36 weeks after the spontaneous onset of labor. She was on 35 mg of prednisolone at the time of delivery.
Five factor score (FFS). 8
Three weeks after delivery, arthralgias and erosive rhinitis recurred on 20 mg of prednisolone daily. Rituximab was initiated at a dose of 375 mg/m2 per week with prompt resolution of all symptoms. Breastfeeding was not desired by the patient.
Results
We reviewed data on 87 pregnancies in 72 women, reported between 1970 and 2017. The pregnancies were divided into four groups: those who had GPA diagnosed during the current pregnancy,10–27 those who had their GPA diagnosed during the puerperium,27,28 those with a prior diagnosis and active disease at conception27,29 and those with a prior diagnosis but inactive disease at conception27,30–50 (Figure 2).
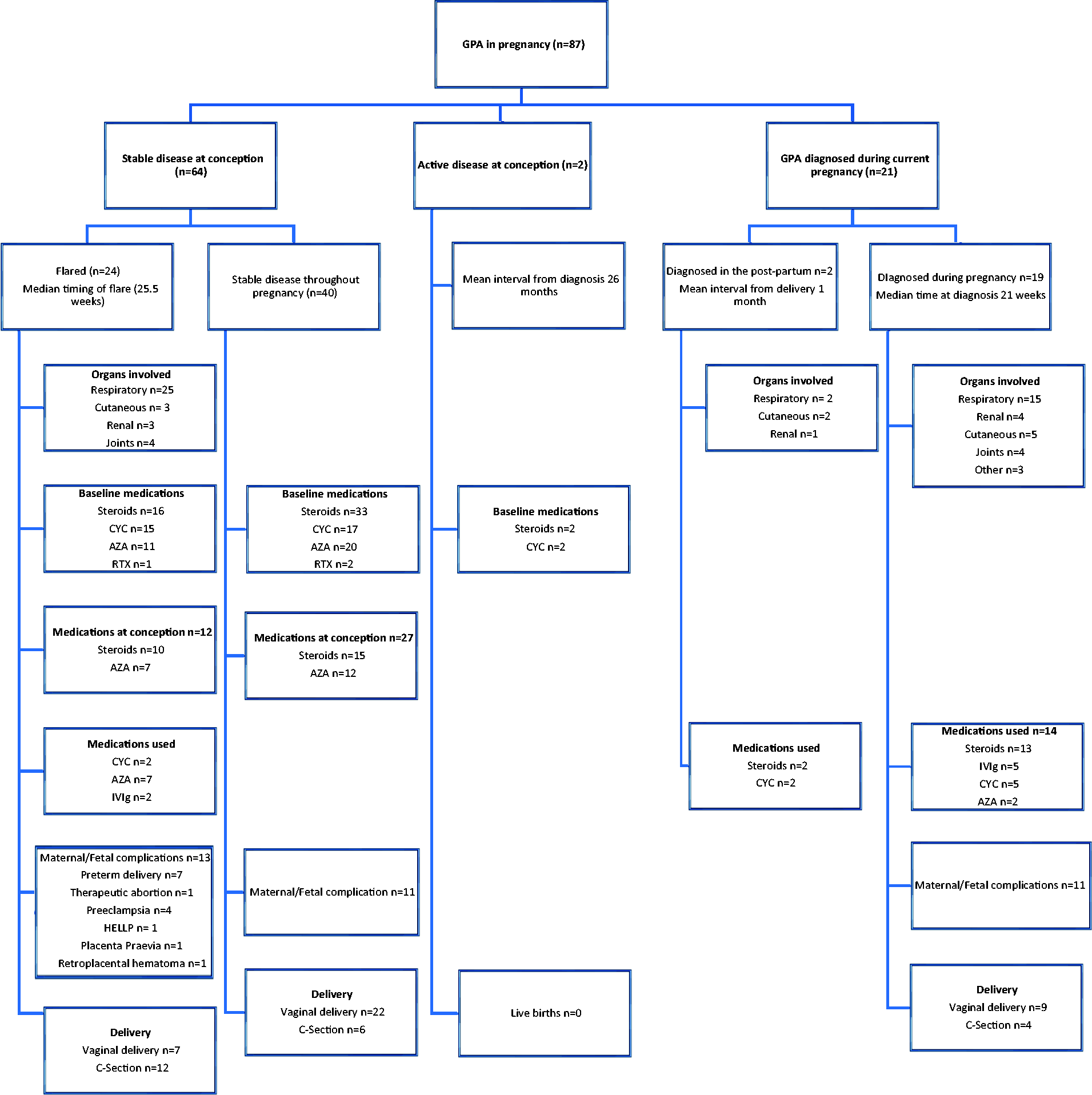
Summary of all published case reports in literature according to disease activity during pregnancy.
GPA diagnosed during pregnancy
Nineteen women with GPA presented for the first time during pregnancy. The median gestation at presentation was 21.6 weeks and it was diagnosed in the second trimester in 43.8% of cases. Almost all cases involved the respiratory system, more frequently the upper respiratory tract (79%) except in one woman in whom the disease manifested as bowel ischemia. 22 The pulmonary symptoms were non-severe except in two women where alveolar hemorrhage was diagnosed. Of the women with renal involvement, one had a termination of pregnancy, two had preterm deliveries and two pregnancies were complicated by severe maternal renal insufficiency.
No treatment was needed in four patients. Head and neck symptoms resolved with local surgeries (myringotomy and middle ear meatotomy) in four women. Cyclophosphamide and IVIg were each used in five women. In the group where cyclophosphamide was used, there were two premature deliveries (at 28 and 33 weeks of gestation at delivery, the reasons for the early delivery were not given) and one woman developed pre-eclampsia (the gestational age at which this developed was not given). Among women treated with IVIg, one had a termination of pregnancy because of renal impairment at 12 weeks of gestation and one pregnancy was complicated at the 34th week of gestation by preeclampsia and preterm planned delivery resulted. There was one maternal death, reported in 1986, from bilateral intracerebral hematomas (which is a rare complication of GPA) at 25 weeks in a woman diagnosed with GPA following severe bloody rhinitis for which azathioprine and corticosteroids were started as an induction therapy. She died one month after initiation of therapy while her disease was still active. 16
Another woman underwent a termination of pregnancy at 13 weeks to avoid any substantial harm for her life. 15 In total, live births occurred in 79% of the pregnancies.
GPA diagnosed during puerperium
We identified two cases of GPA which manifested for the first time in the post-partum period. Both occurred one month post-partum. One patient had respiratory symptoms with arthralgias while the other one had pulmonary, renal, ocular and neural symptoms. Both had good outcomes after treatment with a combination of corticosteroids and cyclophosphamide.
GPA with active disease at conception
Two pregnancies were started with active disease with a BVAS of 10 and 4. The interval between the initial diagnosis and conception was 48 and 4 months respectively. Both had been treated with corticosteroids and cyclophosphamide before pregnancy and were on a pregnancy safe dose of corticosteroids (15–25 mg) at the time of conception. One pregnancy ended with a late miscarriage at 20 weeks 29 and the other one with a stillbirth at 25 weeks. 27 Moreover, the former woman had an immediate pulmonary flare after the fetal loss which responded well to corticosteroids and cyclophosphamide.
GPA with inactive disease at conception
There were 64 pregnancies in 51 women with GPA described in the literature. The interval between the initial diagnosis and conception was 62.6 months. There were 51.5% of women who had completed treatment with cyclophosphamide prior to conception. More than half of the women (51.5%) known to have GPA were on a maintenance treatment from the first day of pregnancy.
Flares complicated 24 pregnancies. These occurred more frequently in the third trimester (66.5%) but the median gestation was 25.5 weeks. The clinical manifestations were mostly exacerbations of tracheal stenosis. Table 3 summarizes treatment before and during pregnancy and its relationship with the occurrence of flares.
Summary of treatment received before and during pregnancy and their relationship to flares.
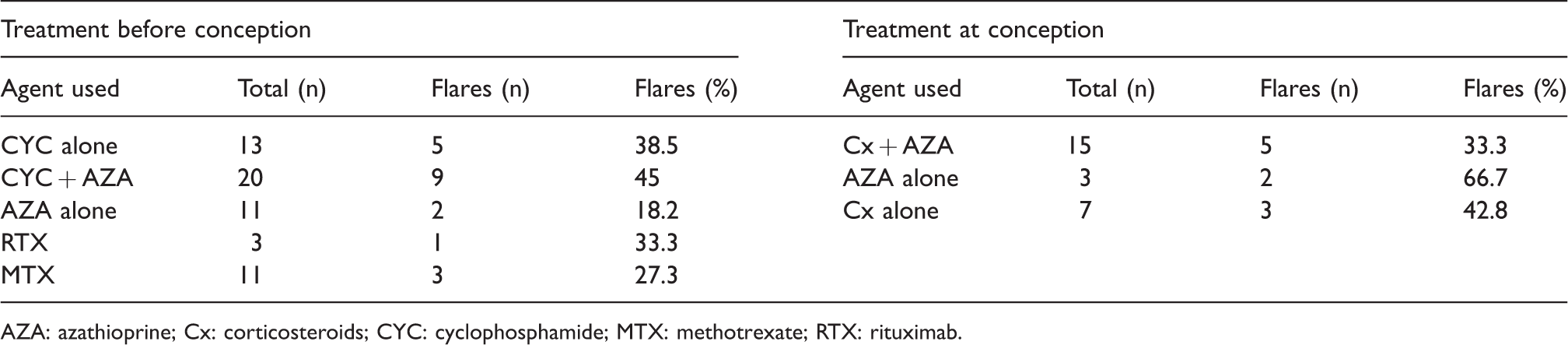
AZA: azathioprine; Cx: corticosteroids; CYC: cyclophosphamide; MTX: methotrexate; RTX: rituximab.
Flares were mild in 29% of women with no need for treatment. Both twin pregnancies were treated with IVIg with complete recovery; however, they were complicated with preeclampsia at 31 weeks’ gestation. Cyclophosphamide was used in two women after the first trimester without maternal or fetal complications. Azathioprine was used alone in seven women. In these women, there were three pregnancies complicated by preeclampsia and one developed placenta previa. Among women who flared, 54.2% had an otherwise uncomplicated antenatal course. Caesarean section was the mode of delivery in 50% of cases; the reason could not be retrieved in half of the cases while preeclampsia was found to be the cause in 30%. Despite the flares, there was a more favorable prognosis than those women with active disease at conception, with a high live birth rate of 96%, although 29.2% of babies were delivered prematurely. Prematurity was mainly secondary to obstetric complications (placenta previa, abruptio placentae) (71.4%). Among women with inactive disease at conception, 14 (22%) had a flare in the post-partum period (six months after delivery). Half of these women had flared during pregnancy.
Stable inactive disease
Forty women with known GPA were stable throughout pregnancy. Fifty percent were on treatment to maintain disease remission since conception; 35% of whom were on corticosteroids alone at low dose (mean of 10.5 mg) and 50% were on azathioprine and corticosteroids at conception. One woman inadvertently conceived on methotrexate and had a miscarriage at eight weeks and another woman was on azathioprine alone. There was no complication in 72.5% of pregnancies. Mode of delivery was by caesarean section in 21.4% of cases, the main indication being pre-eclampsia. Overall, 92.5% of pregnancies resulted in live births.
Discussion
Effect of pregnancy on GPA
Even though GPA disease is rare before 50 years of age, it can occur in younger individuals and has been reported de novo in 21 women during pregnancy in our database (24%). The effect of pregnancy on the disease is unpredictable.
While most of the flares in women with a pre-pregnancy diagnosis occurred at the third trimester (66.5%), the diagnosis de novo was mainly made in the second trimester (43.8%). The difference may be explained by the physiopathology of GPA which involves two elements of the disease: the focal granulomatosis and the more systemic inflammatory vasculitis. In the reported cases, de novo symptoms were mostly systemic, with the main upper respiratory tract manifestation being erosive rhinitis. Conversely, the flares were mostly granulomatous with tracheal stenosis being the most encountered manifestation. The immune system and cytokines are altered in pregnancy mainly via the balance between T helper1/T helper 2 cells (Th1/Th2). Cellular immunity via Th1 occurs in the first and the third trimester and may therefore favor granulomatous manifestations while humoral immunity predominates in the second trimester via Th2 and therefore may explain the more common manifestation of inflammatory vasculitis.
Flares of known GPA are also frequent in the six months following delivery (26.5% of reported cases).
Even though flares occur, the significant maternal morbidity and mortality remains rare with only one maternal death, 16 one limb amputation 17 and one patient commencing hemodialysis for severe renal disease. 10 Fetal prognosis was very poor when conception occurred in the presence of active disease, as is seen in other auto-immune diseases such as systemic lupus erythematosus (SLE). Both pregnancies occurring during an active phase ended in miscarriage. Of those who had inactive disease at the time of conception, there was no significant difference between the group who flared and the group who were stable in either maternal or fetal complications (Table 4).
Statistical comparison between stable disease and flares in known GPA.
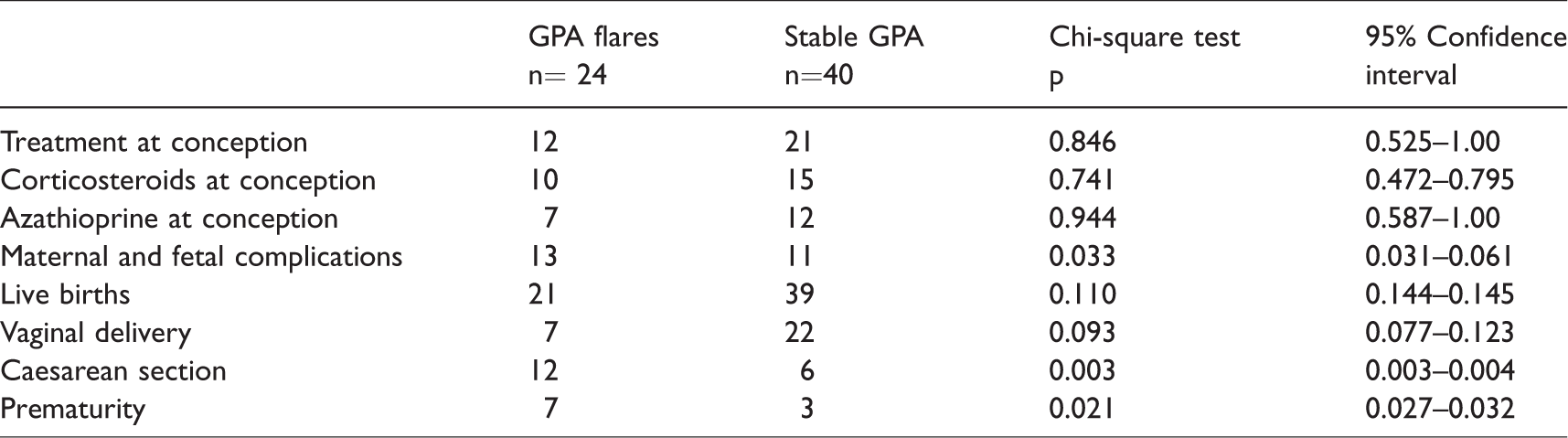
There was no statistically significant difference between the risk of flares in women with inactive disease on medication and women with inactive disease on no medication (Table 4). Sixty-three percent of women on azathioprine were stable throughout pregnancy. 51 It is possible that the benefits of maintenance therapy may be masked by women with severe disease being over-represented in the treatment group, and therefore having a higher baseline risk of flare.
Pregnancy is considered an independent risk factor for disease flares and evolution. Ideally, it should be planned during an inactive period of the GPA.
Effect of GPA on pregnancy
Among 87 pregnancies, 62 (71%) ended in live birth. A flare of previously recognized disease and newly diagnosed disease had the same prognosis for the fetus.
The pregnancy prognosis was considered unfavorable in 25 patients (28.7%): there was fetal loss in 10 pregnancies (11.5%) and premature live birth in 15 pregnancies (17.2%). Compared to active disease at conception, inactive disease has also a high risk of complication (37.5%). Flares in the first trimester were associated with more fetal losses (67%). In fact, among the six flares in the first trimester, one ended in miscarriage and three had a termination of pregnancy due to concerns about maternal health.
Pre-eclampsia is not considered a flare of the disease. However, it is more frequent in women known to have GPA and was not related to flares of the underlying condition (15%), knowing that it occurs in 5% of healthy pregnancies. 52 It is associated with use of corticosteroids during pregnancy (30% of women using corticosteroids presented with pre-eclampsia vs. 4% not using corticosteroids), although this may reflect the severity of underlying disease (Table 5).
Relation of steroid use with pre-eclampsia occurrence.

Delivery by caesarean section was significantly more frequent in women who had a flare during pregnancy, mainly due to pre-eclampsia and other obstetric complications (p = 0.003; CI: 0.003–0.004) (Table 4).
Pregnancy in a woman with GPA should therefore be considered a high-risk pregnancy; close follow-up is mandatory to prevent major obstetric complications.
Therapeutic implications
A multidisciplinary approach is essential in this situation. The choice of the treatment is limited by the need to induce remission without being teratogenic or fetotoxic. Corticosteroids alone are not indicated in the treatment of GPA unless it is localized to the upper respiratory tract, and in our observation, their use in this setting was beneficial for both the woman and the pregnancy outcome.
In systemic disease when symptoms occur in the first trimester, therapeutic options are limited due to the high risk of teratogenicity with commonly used agents. In fact, cyclophosphamide (teratogenic) and rituximab (decreased fetal B lymphocytes) are better avoided during this period while azathioprine can be safely given. 9 In severe disease occurring in the third trimester, early delivery followed by treatment with cyclophosphamide was the most frequently reported approach, but cyclophosphamide does not have to be withheld until after delivery, and indeed was also used in the second and third trimester in some women with few complications (mainly prematurity) and good overall prognosis. In the one case where azathioprine was used as an induction treatment along with steroids for four weeks, the outcome was maternal death from constant active disease. This is an important reminder that mortality in GPA remains high in untreated disease and potentially life-saving therapies should not be withheld solely due to fetal concerns.
IVIg offer a promising alternative. This can be used for induction therapy in the first trimester with no side effects reported. This showed good efficacy (85.7%) in seven pregnancies in our study including two twin pregnancies.
Interestingly, there were no cases of rituximab use during pregnancy for GPA reported. Use in pregnancy has been reported in many different conditions (rheumatoid arthritis, SLE, lymphoma, autoimmune cytopenias, multiple sclerosis and Castleman disease in patients positive for HIV) without adverse fetal outcomes.53–55 The use of rituximab is usually postponed until the second trimester. 47 In our patient, the choice of IVIg over rituximab was taken following the decision of the national reference center for vasculitis in Paris (Hôpital Cochin).
A publication bias is likely; the reported cases are probably the most severe and consequently it is difficult to generalize our findings. A multicenter prospective study aiming to describe the experience of women with vasculitis who become pregnant, is in progress (https://clinicaltrials.gov/ct2/show/NCT02593565).
Conclusion
From currently available published cases, 39% of women known to have GPA will flare during pregnancy. Pregnancy outcomes are linked to the status of the disease at conception and the timing of flares. The most common fetal complication is prematurity and pre-eclampsia is frequent.
Planned pregnancies are strongly advised and close multidisciplinary follow-up is necessary. Maintenance treatment with azathioprine should be considered to limit flares of the disease. Treatment options, particularly in the first trimester are limited by the risk of teratogenicity. In this situation, IVIg may offer a safe and effective therapeutic option.
Footnotes
Acknowledgments
We thank the patient for letting us share her case.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Written consent was obtained from the patient for publication of case report and associated images.
Guarantor
MLeB is the guarantor of the present work.
Contributorship
AD and MLeB took the lead in writing the manuscript. All authors provided critical feedback and helped shape the research, analysis and manuscript.