
Abstract
Background
The Shock Index is a clinical tool to evaluate the hemodynamic status during hemorrhage. The impact of labor and pre-existing anaemia is unknown. The objective was to describe and discuss its clinical utility in this context.
Methods
This was a prospective cross-sectional study. The Shock Index (ratio between heart rate and systolic blood pressure) was measured in pregnant women at term, before or during labor. They were stratified according to the presence of anemia.
Results
The median Shock Index was significantly lower in women in labor than in those not in labor (0.72 (IQR: 0.64–0.83) vs. 0.85 (IQR: 0.80–0.94); p < 0.001). In women in labor, the Shock Index was not significantly different if anemia was present (0.72 (0.63–0.83) vs. 0.73 (0.65–0.82); p = 0.67).
Conclusions
Values of the Shock Index are affected by labor, which may hinder its utility in identifying hemorrhage during this period. However, the values were not altered by maternal anaemia. Therefore, an abnormal postpartum Shock Index should not be attributed to an abnormal antepartum Shock Index due to mild/moderate anemia.
Introduction
Postpartum hemorrhage (PPH) is recognized as the leading cause of maternal morbidity and mortality worldwide. 1 Although maternal mortality rates from this have declined in developed countries, approximately 50% of maternal deaths in low and middle-income countries (LMICs) are due to hemorrhage, particularly postpartum.1,2 PPH is also one of the leading causes of severe maternal morbidity, increasing the risk of admission to the intensive care unit and surgical interventions such as postpartum hysterectomy. 3 Despite the impact of PPH, a useful clinical tool to identify women early has remained elusive. 2
Visual estimation of blood loss—the most common method used for the diagnosis of PPH—has shown to be inaccurate and may contribute to a delay in the diagnosis and treatment of PPH.4–6 In addition, none of the quantitative or semi-quantitative methods proposed for estimating vaginal blood loss (e.g. collection of blood into plastic bags and weighing (gravimetric) or measurement of blood pigments using a spectrophotometer (photometric)) have been adopted in clinical practice due to their complexity or their high cost.7,8 Therefore, it has been suggested that early recognition of signs and symptoms of hypovolemia should guide diagnosis and treatment of PPH.9–13 However, due to the physiological changes of pregnancy particularly during the peripartum period, a drop of blood pressure (BP) or abnormalities in heart rate (HR) may be only evident when there is advanced hemodynamic compromise.14
The Shock Index (SI)—defined as the ratio between HR and systolic blood pressure (SBP) 15 —has been validated and applied in various scenarios in non-obstetric populations including trauma.16,17
It has been proposed as a useful and reliable tool to detect and/or predict hypovolemia and early hemodynamic compromise in obstetric populations at risk,18,19 even when other vital signs are within normal values. 20 In the non-pregnant population without any haemodynamic compromise, the SI range is 0.5–0.7. 15 Recent studies in obstetric patients proposed a normal SI range for pregnant women between 0.5 and 0.9, concluding that a SI <0.9 provides reassurance.18–21 A recent study from UK analyzed the normal range of SI in postpartum women and the influence of uterotonics and epidural analgesia. 18 However, those studies were conducted in women in developed countries and the potential influence of confounders in developing countries such as the presence of mild/moderate anemia has not been considered. 21 Anemia is more prevalent in pregnant women in LMICs. 22 Thus, in order to support and recommend the use of SI for the evaluation of pregnant patients in developing countries, the effect of mild/moderate maternal anemia in the interpretation of the SI should be described. The aim of our study was to describe the normal values of SI in pregnancy both before and after the onset of labor, and in the contexts of mild/moderate anemia and a normal hemoglobin level.
Materials and methods
A cross-sectional study was designed including women admitted to the Rafael Calvo Maternity Hospital (“Clínica de Maternidad Rafael Calvo”, CMRC) in Cartagena de Indias, Colombia, the largest maternal public health care institution on the North-East coast of Colombia. All women provided written informed consent and the Institutional Review Board of CMRC and Cartagena University approved the use of clinical data for research purposes.
From March 2013 to May 2013, consecutive women with singleton term pregnancies (>37 gestational weeks) determined by last menstrual period and confirmed by ultrasound, and admitted during the day-shift were included. Two groups were studied: group 1 consisted of women attending antenatal care and not in labor (n = 53); and group 2, women at term in labor (n = 47). Patients in labor were included if they met the following criteria: (1) regular uterine contractions; (2) ≥4 cm dilatation and/or ≥80% of cervical effacement with intact membranes.
Women from both the labor and no-labor group were excluded if: (1) gestational age was <37 or ≥42 weeks; (2) body mass index (BMI) was <18 or >30 kg/m2; (3) multiple pregnancy; (4) pre-existing medical conditions; (5) use of medications known to affect the cardiovascular system; or (6) patients developed hypertensive disorders in the index pregnancy. We also excluded women with severe anemia according to the World Health Organization (WHO) definition (hemoglobin <7 g/dl). BMI was calculated using weight and height recorded at the time of entry into the study for the no-labor group, and last entry in their prenatal record card in the labor group. We excluded under and overweight women given the low number expected and the possible bias induced by these BMI. Hemoglobin values were recorded from a complete blood count performed at admission for patients who were in labor or using the most recent measurement made in the last two months before the expected date of delivery for patients who were not in labor.
Measurements were carried out in the semirecumbent position to prevent supine hypotension syndrome. BP and HR were obtained using a digital sphygmomanometer (OMRON HEM-7220—Healthcare). This device has a bracelet “Comfit” that adapts to the contours of the arm, has a capacity to measure BP and HR and obtain the average value of three measurements made at different moments. Health care personnel were trained to perform adequate measurement of BP. The SI was calculated from the average of three measurements of BP and pulse with a time difference between each test of 5 min for women without labor or between contractions for those patients included in labor. None of the patients received obstetric analgesia or anesthesia during labor.
Statistical analysis
The Kolmogorov–Smirnov test and visual plot inspection were used to assess the normality of continuous data distributions. Student’s t-test or the Mann–Whitney U-test and Pearson Chi-square test were used to make univariate comparisons of quantitative and qualitative variables, respectively, between groups. A value of p <0.05 was considered significant. All analyses were performed using STATA (STATA for Windows, StataCorp, TX, USA).
Results
A total of 113 women met the inclusion criteria. Fifty-four women were included in the not in labor group and 59 with term pregnancies in labor. One woman was excluded from the no-labor group because of the onset of contractions. In women in labor, 20.3% (12/59) were excluded, eight with clinical diagnosis of obstructed labor and delivered by caesarean section and four women that did not have complete data. Table 1 shows the demographic and clinical characteristics of the women included in the study. Maternal age and BMI were similar between the groups. The gestational age at recruitment and parity were significantly higher in women included in labor than in those without labor. Otherwise, there were no significant differences in demographic characteristics between the two groups (Table 1).
Demographics and clinical characteristics of obstetric patients at term during and not in labor.
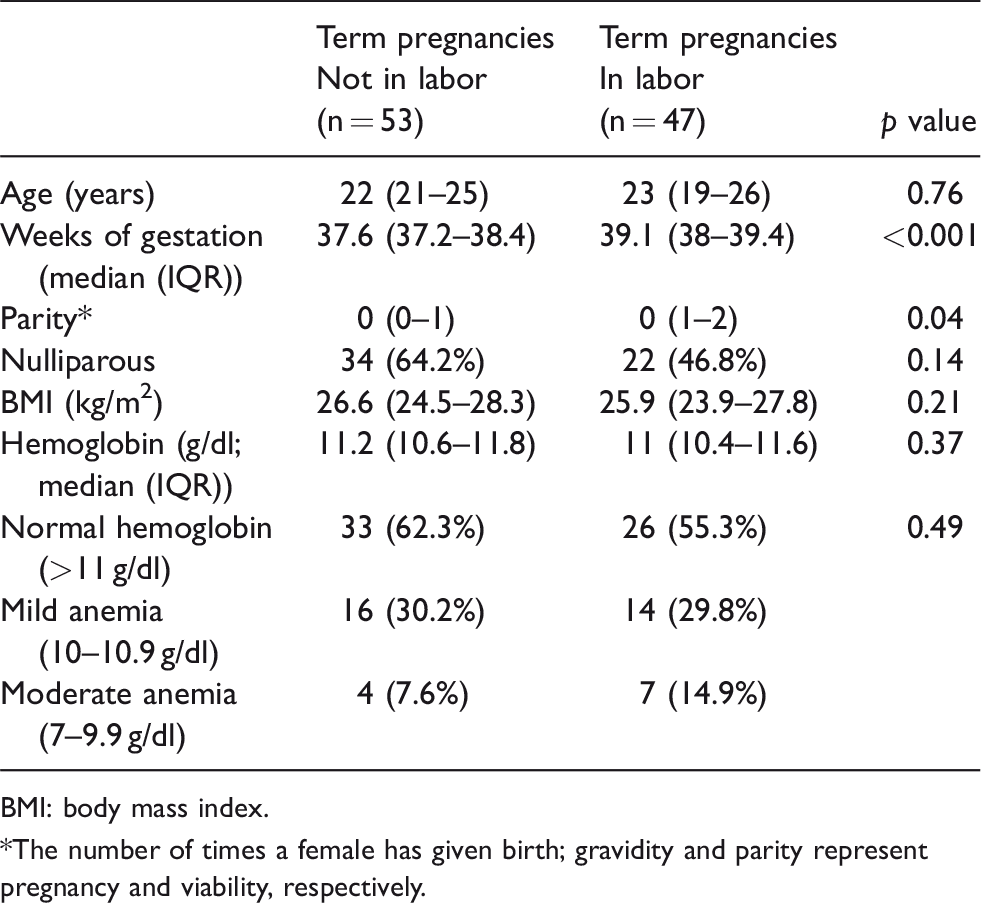
BMI: body mass index.
*The number of times a female has given birth; gravidity and parity represent pregnancy and viability, respectively.
In term pregnancies without labor, 62.2% (n = 33) of the women had normal hemoglobin values (≥11 g/dl) and 37.7% (n = 20) showed mild to moderate anemia, with a small number of cases with moderate anemia (mild 10–10.9 g/dl: 30.1%, n = 16; moderate 7–9.9 g/dl: 7.5%, n = 4; Table 1). Values of the SI in the study groups are presented in Table 2. We compared the values of the SI between the two groups, stratified by labor and no labor. The median (interquartile range (IQR)) SI in patients in labor 0.72 (0.64–0.83) was significantly lower than in those without labor 0.85 (0.80–0.94; p < 0.001). The median (IQR) SI in women with anemia was 0.82 (0.77–1.00) and 0.85 (0.81–0.93) for women without anemia (p > 0.05). Furthermore, differences of SI between the three different levels of hemoglobin (mild, moderate and no anemia) were not statistically significant (p value >0.05; Figure 1).
BP, heart rate, and Shock Index values in pregnant women at term according to whether they were in labor or not.
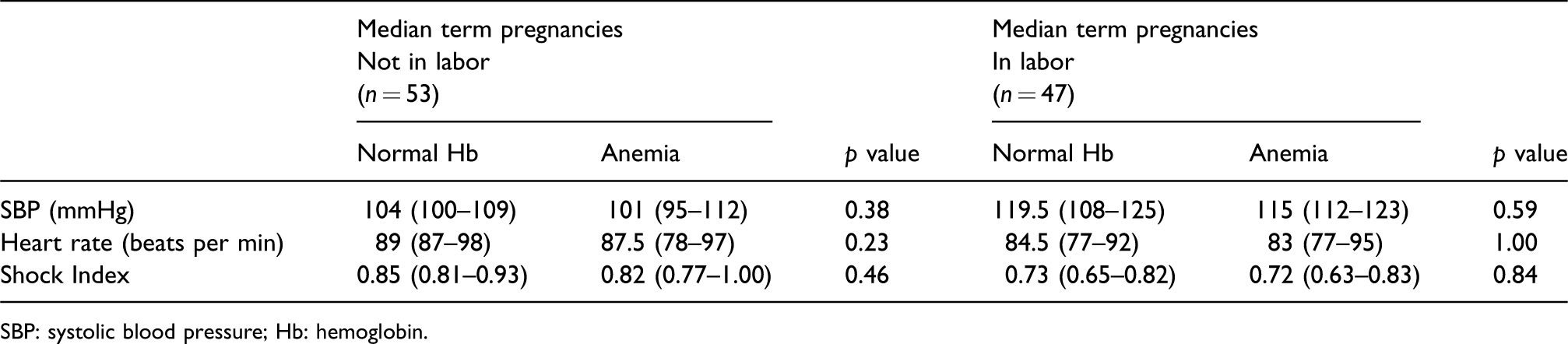
SBP: systolic blood pressure; Hb: hemoglobin.
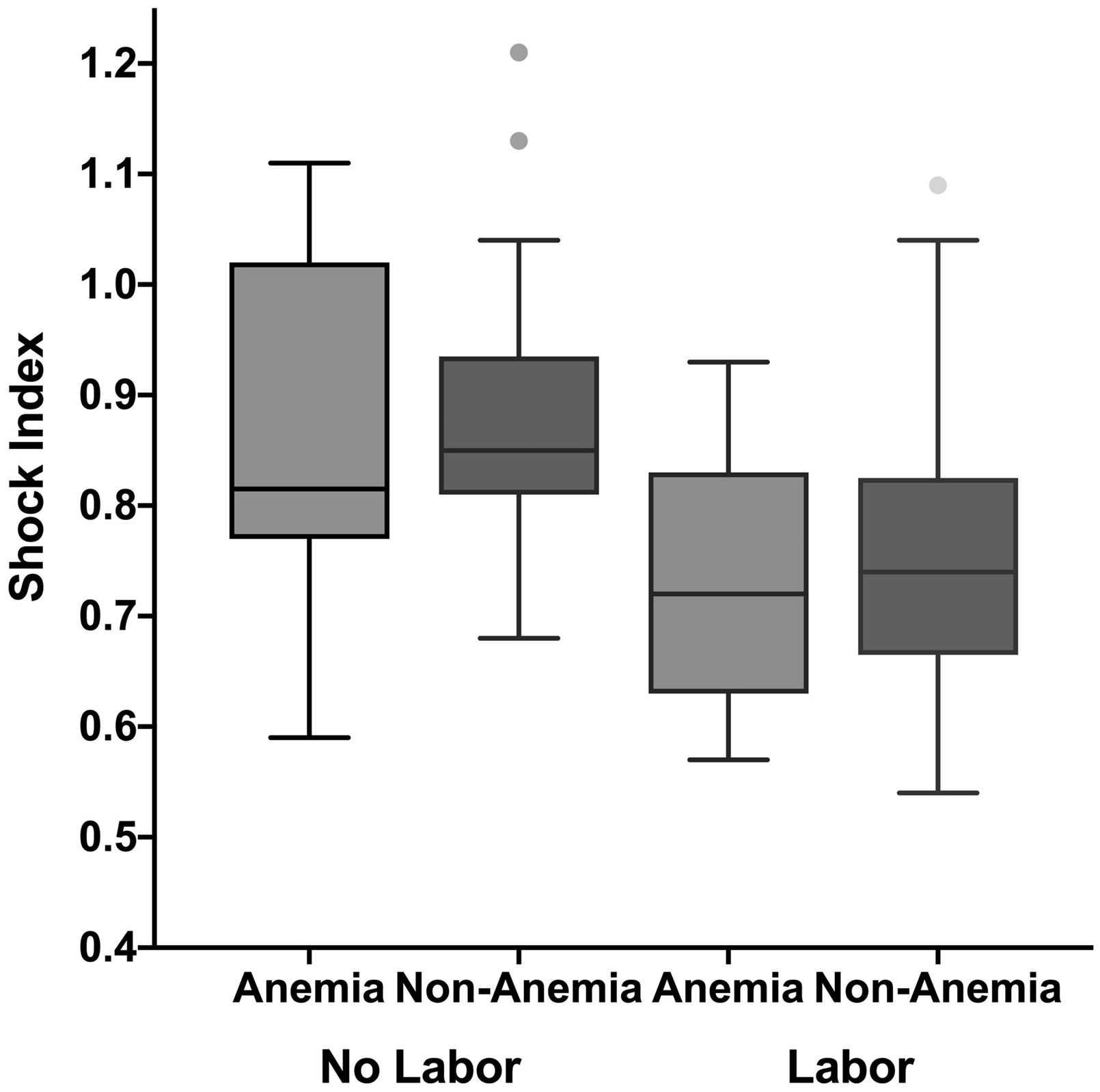
Comparison of Shock Index values in obstetric patients during and without labor, adjusted by the presence of anemia.
In the group of women in which the SI was measured in labor, 55.3% (n = 26) had normal hemoglobin, 29.7% (14/47) presented with mild anemia, and 14.8% (7/47) with moderate anemia (Table 1). Mean dilatation in these patients in labor was 7 cm (±SD 1.46), effacement was 80% (±SD 6.41). The median (IQR) SI was 0.72 (0.63–0.83) in women in labor with anemia, and 0.73 (0.65–0.82) for women in labor without anemia. There were no significant differences in the SI when women with different degrees of anemia were compared (p = 0.67).
Discussion
The main findings of this study are that the presence of labor in the mother may affect the values of the SI in this population, and that mild/moderate anemia did not change the values of SI. However, numbers were too small to show significance. Based on these data, an SI >0.9 should not be falsely reasoned to be due to the mild anemia. The change in SI during labor is driven by the physiological increase in BP, and the SI still falls within what is deemed a “normal SI” in pregnancy. Therefore, an SI > 0.9 should alert a practitioner to a problem, even in labor, and not be put down to normal physiological changes.
Evidence in the non-obstetric population shows that the SI can be a potentially valuable tool in various clinical settings for mortality prediction and risk assessment14,23 and has recently generated interest as a tool for the early detection of hypovolemia and hemodynamic compromise in obstetrics. 21 ,24–26 The SI has been used for the prediction of hypovolemia and severe maternal outcomes in women with ectopic pregnancy and in PPH.25–27 However, the majority of studies have evaluated the postpartum period and there was no data describing whether the values of the SI were affected by the presence of labor and/or maternal anemia, two situations potentially complicating vital sign measurements during hemorrhage in pregnancy. Labor and mild to moderate anemia do not seem to affect the SI to a degree to deem it useless in the immediate antepartum and intrapartum period, and an SI >0.9 should raise the question of concealed antepartum hemorrhage or uterine rupture.
During labor, in women who do not receive analgesia or anesthesia, pain and the resulting anxiety can induce activation of the sympathetic nervous system, leading to an increase in HR. As labor progresses, contractions lead to an increase in cardiac output by a mean value of 34–50%. 28 This rise is due to increases in both HR (15%) and stroke volume (15%) as result of the passage of about 300 to 500 ml of blood from the uterus to the systemic circulation during each contraction, resulting in an increase in SBP of 35 mmHg. 28 This may explain the significant decrease of the SI in women in labor, bearing in mind that any elevation in SBP results in a decrease of the SI. It is noteworthy that even in developed countries, it has been reported that the use of obstetric analgesia is less extensive among immigrants or women from minority ethnic groups, 29 making our data valuable for further study of the SI in those settings.
Our finding suggests that the presence of mild to moderate maternal anemia during pregnancy does not modify the results of the SI. In our study, the prevalence of mild to moderate maternal anemia was 41% (41/100), which is in concordance with the prevalence among other developing countries (38% (CI 33–43%)). 22 Ongoing studies from our group are exploring whether the values of the SI antepartum at term and in the immediate postpartum period in patients with and without PPH is modified by the presence of severe anemia, extreme values of BMI or preeclampsia.
This study has several limitations. This is a single center study at sea level; we are not proposing these normal values for all pregnant women under all or even most scenarios, although the values found are comparable with those reported by previous studies from developed countries using large sample sizes. 18 , 21 Also, the postpartum period was not included in our study of women during labor. The small sample size may limit analysis and conclusions of the stratified analysis, particularly for the moderate anemia group. Thus, our results may not be applicable to the general population, but to the group who are relatively normal or with mild/moderate anemia. Values of the SI may be affected by the technique of measurement and calibration of the equipment and during labor due to maternal position or stress. Strengths of our study are the prospective evaluation that was done and data collection of clinical information by use of three measurements of HR and BP with calibrated equipment and by trained personnel, through a standardized prospective process.
This study provides important information on normal values of SI described for the first time in pregnancy at term and in labor in a population from a developing country without access to anesthesia or analgesia and a high prevalence of mild to moderate anemia. We believe that the SI should be recommended by international organizations as a tool for early evaluation and monitoring of women with PPH. Inadequate early diagnosis and delayed treatment of women with PPH may lead to hypoperfusion and lactic acidosis, resulting in multiorgan dysfunction, and coagulopathy
Characterization of the SI in this population as we have described it, will allow further research of its predictive value to identify hemodynamic instability. This finding could aid practitioners, midwives and physicians alike, in rural settings and in facilities, to initiate early treatment and/or initiate early referral to reduce maternal morbidity or mortality.
Footnotes
Acknowledgments
We are grateful to the equipment of the labor and delivery room of the Clínica de Maternidad Rafael Calvo in Cartagena de Indias, Colombia, whose support was fundamental for the acquisition of the data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional Review Board of CMRC and Cartagena University approved the use of clinical data for research purposes.
Informed consent
All patients provided written informed consent.
Guarantor
JRS
Contributorship
JRS, APC, and JM made substantial contributions to the concept and design of the work, analysis, and interpretation of data. JET, LGP, FP, AM, and NG drafted the article and revised it critically. All authors approved the version to be published.