
Abstract
Peripartum cardiomyopathy is a syndrome of maternal heart failure with decreased left ventricular ejection fraction affecting maternal and fetal well-being. We analysed clinical profiles and outcomes in women with peripartum cardiomyopathy enrolled retrospectively from a tertiary care centre in southern India (1 January 2008–31 December 2014). The incidence of peripartum cardiomyopathy was one case per 1541 live births. Fifty-four women with a mean age of 25.5 years and mean gestational age of 35.4 weeks were recruited; 35 were primigravidae. Maternal and fetal deaths occurred in 9.3% and 24.1% of subjects, respectively. Mild-to-moderate maternal anaemia (80–110 g/L) was associated with fetal mortality (p = 0.02). Reduced left ventricular ejection fraction (<30%, p = 0.04) and cardiogenic shock (p = 0.01) were significantly associated with adverse maternal outcomes. Forty per cent of women were followed up after 24.2 ± 17.7 months, and in these women a significant increase in left ventricular ejection fraction was seen (mean 16.4%, p < 0.01); all were asymptomatic. Peripartum cardiomyopathy with poor left ventricular ejection fraction and shock is associated with adverse maternal outcomes, while non-severe maternal anaemia predisposes to adverse fetal outcomes. Significant left ventricular ejection fraction recovery occurred on follow-up.
Introduction
Of the pregnancy-associated cardiovascular diseases, peripartum cardiomyopathy (PPCM) represents a potentially fatal syndrome of heart failure (HF) with reduced left ventricular ejection fraction (LVEF) in previously healthy women. 1 Despite the knowledge of morbidity and mortality associated with this condition, the aetiology remains unknown and is subject to much speculation. PPCM resembles dilated cardiomyopathy (DCM) with regard to its phenotypic characteristics, but is considered to be a distinct entity, separate from other cardiomyopathies. 2 The Working Group on PPCM of the Heart Failure Association of the European Society of Cardiology (ESC) defines PPCM as a non-familial form of peripartum HF characterized by left ventricular (LV) systolic dysfunction presenting towards the end of pregnancy or in the months post-delivery, where no other cause of HF is found. 1 Hence, the diagnosis depends on the temporal relation of the symptoms with pregnancy as well as the exclusion of other cardiomyopathies. Despite an increasing awareness of PPCM over the years, there is much left to clarify in the areas of epidemiology, risk factors, pathophysiology and management.
Epidemiology
Data on PPCM are relatively sparse and are dominated by numbers contributed by epidemiological studies from Africa, Haiti, European nations and the United States of America (USA).3–6 The incidence of PPCM shows a significant variation with the ethnic and regional background of women; Africans and African-Americans have been shown to have a greater propensity for developing PPCM, with an estimated incidence of 1:100 in Nigeria and 1:299 in Haiti.7,8 In Caucasian populations, incidences range from 1:1000 in Germany to 1:10,149 in Denmark.6,9 According to a cross-sectional study of 14,323,731 hospitalisations for pregnancy in the USA from 2004 to 2006, the hospitalization rate for cardiomyopathy in the postpartum period was 0.46 per 1000 deliveries (0.18 for apparent PPCM, 0.28 for other cardiomyopathies). 10 A large difference in the incidence of PPCM between ethnic groups in the USA was demonstrated in another study: 1 per 1421 in African-American women, 1 per 2675 in Asian women, 1 per 4075 in white women and 1 per 9861 in Hispanic women. 4
Scarce data are available regarding the incidence of PPCM in Asian populations with the incidence in Japanese and South Korean populations estimated at 1:20,000 and 1:1741, respectively.11,12 A single centre study from Pakistan reported an LV recovery rate of 71% with no mortality. 13 In stark contrast, poor outcomes have been reported from geographic areas such as Turkey (mortality rate of 24%, LV recovery in 30%) and Africa (mortality rate of 13–17%, LV recovery in 21%).14,15 Risk factors predisposing to PPCM include advanced age, black race, preeclampsia, multiple gestation, hypertension, anaemia and prolonged tocolysis. 16 However, the disease process is heterogeneous as demonstrated by the fact that most women with preeclampsia do not manifest as PPCM and a large proportion of women with PPCM are young primiparous women. 17 Recent studies from Germany and Japan describing outcomes in PPCM reported a mortality rate of 2–4% with LV recovery rates of 60% at 3–6 months.6,11 The vast difference in incidence among different populations and ethnicities may also be due to variations in the methodology of estimation.
Studies with regard to mortality in PPCM reported a rising trend with maternal age, in women with live birth order of at least four, and in black women, who were 6.4 times more likely to die compared with white women. 18 A significant proportion of deaths have been noted within the first week and between 80 and 90% within six months of diagnosis, attributed to either progressive HF or sudden cardiac death. 18 Mortality is higher in women with a baseline LVEF of 25% or less. 19 A delay in the diagnosis of PPCM has also been noted to contribute to mortality. 19
Among Indian studies on PPCM, Mandal et al. described associations and outcomes of 36 women diagnosed with PPCM. 20 Five cases (14%) developed persistent LV dysfunction after six months of presentation with maternal mortality being 14%. A study from a South Indian tertiary care centre showed an incidence of 1:1374 live births but was limited by a low number of women. 21 The relative scarcity of literature from India has impeded strategy formulation for the diagnosis, management and follow-up of women. Therefore, we aimed to analyse the incidence of PPCM from a tertiary care centre in southern India and determine clinically significant associations with maternal and fetal outcomes, which are specific to this geographic region.
Materials and methods
This retrospective, observational study was conducted among women admitted with a clinical diagnosis of PPCM between 1 January 2008 and 31 December 2014 under the Departments of Medicine, Unit-3 (Obstetric Medicine) or Obstetrics of the Christian Medical College and Hospital, Vellore, Tamil Nadu (India), which is a 3000 bed tertiary care centre. 2 There were 83,203 deliveries during the study period. Women were included if there were features of HF in the last six weeks of pregnancy or five months postpartum, with an absence of other identifiable causes of HF including valvular lesions, absence of features of HF prior to last month of pregnancy, LV systolic dysfunction on echocardiography defined as one of LVEF less than 45%, fractional shortening less than 30%, or both, and possible additive LV end diastolic dimension greater than 2.7 cm/m2 body surface area. Those with incomplete patient details at baseline, pre-existing HF, chronic obstructive pulmonary disease, valvular heart disease, blood pressure of 170/100 mmHg or greater or severe anaemia as per World Health Organization guidelines (haemoglobin < 80g/l) were excluded. The schematic depiction of recruitment of women into the study is as shown in Figure 1.

Flow chart depicting recruitment into the study and follow-up.
The primary outcomes of interest assessed included the risk factors, disease characteristics and predictors of poor maternal and fetal outcomes as described in the medical literature.12,16,21 Data were extracted from patient records by a trained physician. Accuracy of the data was checked by the principal investigator. Data were analysed by an independent clinician who was unaware of the outcomes. Categorical variables are presented as frequencies and percentages, while continuous variables as mean and standard deviation after assessments for normality using the Shapiro–Wilk test. The chi-square test or Fisher’s exact test have been used for comparison of nominal variables, and the two-sample t-test or the Mann–Whitney U test were used to compare continuous variables. A p-value less than 0.05 was considered statistically significant. All components of the statistical analysis were performed using IBM SPSS Statistics Version 23 (IBM, Armonk, NY, USA).
Results
Fifty-four women with PPCM were included in the analysis after strict enforcement of the inclusion and exclusion criteria, of which the majority were primigravidae (35(64.8%)); the incidence of PPCM was noted to be one case per 1541 live births. A total of 83,203 live births occurred over the study period. The mean age at presentation was 25.5 years with a mean gestational age of 35.4 weeks. Seven women had multiple pregnancies, all of which were twin gestations. Maternal and fetal deaths were noted to occur in 9.3% (5/54) and 24.1% (13/54) of the study population, respectively. Patient characteristics were tabulated with a comparison of maternal and fetal outcomes across groups (survivors vs. non-survivors) as seen in Tables 1 and 2. A total of 150 cases of maternal mortality were noted due to non-PPCM causes during the study period. Prior studies have highlighted the various causes of maternal and fetal mortality at our centre. 22 Haemorrhage, puerperal sepsis and hypertension together have caused 37.1% of maternal deaths in our hospital over the last decade. The mean age of the cohort of women sampled during our study period was 31.1 years; we also calculated proportions of women suffering from various comorbidities such as diabetes mellitus (15.1%), anaemia (21.7%), hypertensive disorders (3.2%) and hypothyroidism (3.1%).
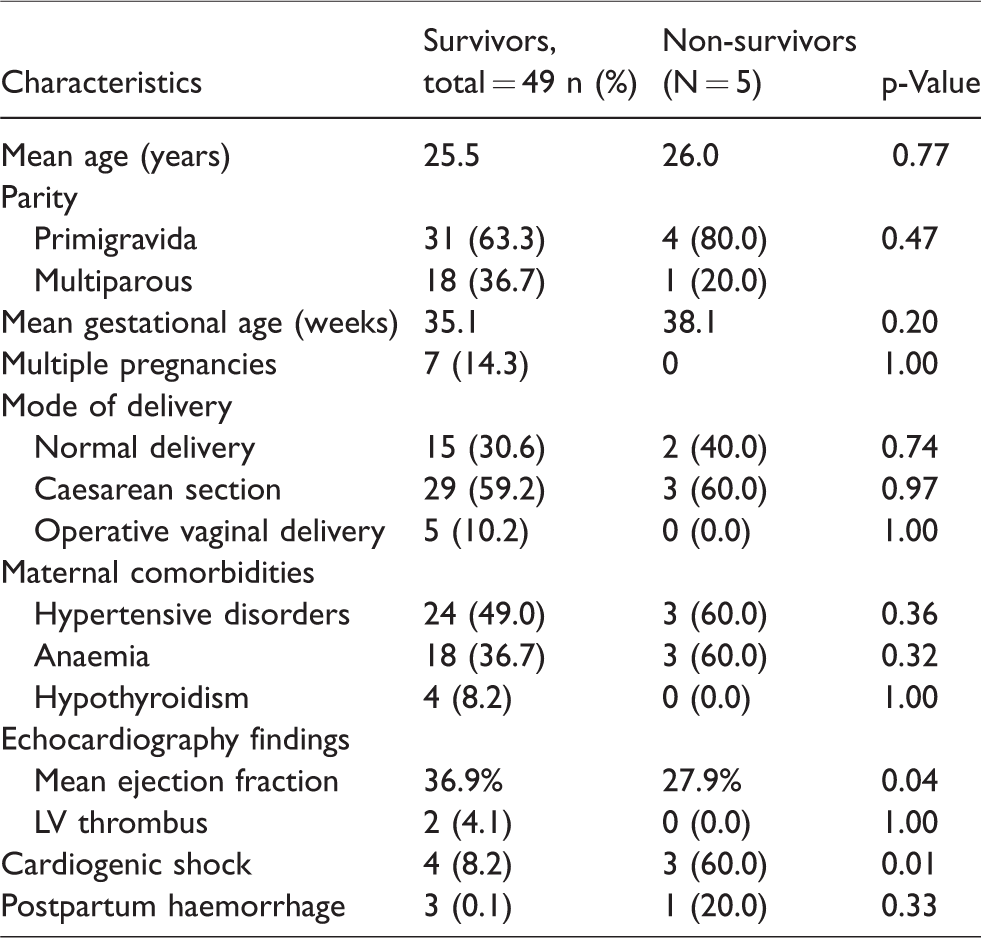
Patient characteristics and maternal outcomes.
Patient characteristics and fetal outcomes.

The predominant symptom at presentation was exertional dyspnoea with 29 (53.7%) women having New York Heart Association (NYHA) class III symptoms and 14 (25.9%) women having NYHA class IV symptoms. Thirty-nine (72.2%) women had pulmonary oedema on clinical examination and 7 (13%) women had cardiogenic shock as manifested by hypotension with cold, clammy extremities associated with poor cardiac contractility. None reported syncope. Only two (3.7%) women had documented episodes of thromboembolism. ECG findings of sinus tachycardia were noted in 100% of the women with a mean heart rate of 104.4 beats per minute; ischaemic changes such as ST-T changes and poor R wave progression were noted in 10 (18.5%) women. The mean ejection fraction on the baseline echocardiogram was 36.1%. Long-term follow-up data were available for 20 women with review echocardiography. The mean duration of follow-up was 24.2 months. The mean EF on repeat echocardiography was noted to be 53.7 ± 4.5% as seen in Figure 2. The mean change in EF was noted to be 16.4 ± 5.5% (p < 0.01). All women were asymptomatic at review.
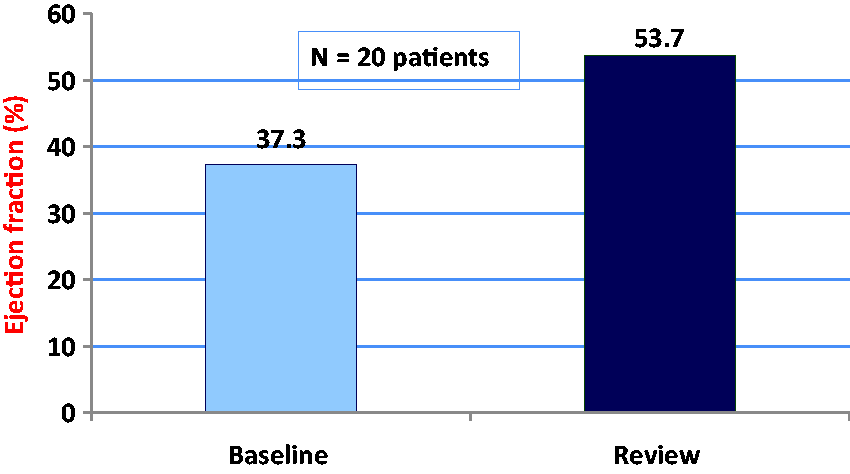
Comparison of ejection fraction at baseline and on follow-up (mean duration of follow-up = 24.2 months).
Thirty-two (59.3%) women underwent a lower segment caesarean section (LSCS), while 5 (9.3%) women underwent operative vaginal deliveries (suction cup or forceps). On evaluation of maternal mortality as the primary outcome (Table 1), mean EF was found to be significantly lower among the poor maternal outcome group (mean EF 27.9%) when compared with the group that had a good maternal outcome (mean EF 36.9%, p = 0.04). The odds of a poor maternal outcome was noted to be significantly higher in those with cardiogenic shock (odds ratio = 16.9, p < 0.05). Other comorbid illnesses such as gestational hypertension, hypothyroidism and anaemia did not influence the maternal outcomes. Five (9.3%) women had gestational diabetes mellitus but there was no significant association with maternal mortality (p = 0.4). Factors associated with poor fetal outcomes were non-severe anaemia with haemoglobin (Hb) between 80 g/l and 110 g/l (69.2% vs. 31.7%) with a p-value of 0.02. The mean Hb was 103 g/l among those with poor fetal outcomes.
Mild-to-moderate anaemia was noted to be a predictor of poor fetal outcomes (p = 0.02). In the group with adverse maternal outcomes, LVEF was significantly reduced (p = 0.04) (Table 1) with a greater proportion of cardiogenic shock (p = 0.01) as compared to the group with good maternal outcomes.
Discussion
PPCM is a rare illness of uncertain aetiology occurring in late pregnancy or early puerperium. The incidence is variable based on geographic location and race. The incidence in our study was one case per 1541 live births. A similar incidence of one case per 1374 live births was noted in a study by Pandit et al. 21 The aetiology of PPCM is not well elucidated and many hypotheses have been proposed. 23 However, it is acknowledged to be distinct from idiopathic DCM. Several unconfirmed aetiologies such as infective viral triggers, a pregnancy-mediated abnormal hemodynamic response, myocarditis, autoimmune factors, inflammatory mediators, prolonged tocolysis and selenium deficiency have been postulated.2,17,24 PPCM has also been speculated to be mediated by a 16 kDa fragment of prolactin. 25
Risk factors for PPCM which have been previously studied include multiparity, advanced maternal age, multiple gestation, African descent, gestational hypertension, preeclampsia, family history, smoking and maternal cocaine abuse.1,26 Elkayam et al. had previously demonstrated that PPCM can occur at any age but a higher incidence was noted in women aged 30 years or more. 27 Our cohort was relatively younger with the mean age at presentation being 25.5 years. In relation to traditional risk factors, no significant association was determined with regard to gestational hypertension or diabetes mellitus and hypothyroidism. Anaemia was found to have an association with fetal mortality.
PPCM is known to have a variable clinical course and remains a diagnostic and therapeutic challenge. 28 Clinical features are similar to those observed in any other form of DCM and include exertional dyspnoea, fatigue, syncope and oedema. 16 The mainstay of diagnosing and prognosticating PPCM is echocardiographic analysis with demonstration of LV systolic dysfunction after excluding other causes of HF, like valvular heart disease, restrictive and hypertrophic cardiomyopathy. 29 Electrocardiography mostly shows non-specific features such as sinus tachycardia, non-specific ST-T changes and evidence of left atrial or ventricular enlargement, but is useful for detecting and correcting aggravating factors such as arrhythmias. 30 ECG features in our cohort included sinus tachycardia (mean rate = 104.4 beats per minute) and ischaemic changes in 10 (18.5%) women. Endomyocardial biopsy may occasionally be used to confirm or rule out other cardiomyopathies. 3
The management of PPCM is similar to that of other forms of HF and depends on the functional class, with NYHA class III and IV cases preferably managed in a hospital. 30 Euvolemic status is maintained by dietary sodium and fluid restriction with optimisation of diuretics. 28 Angiotensin converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs), the mainstay of HF management in non-pregnant individuals due to their effects on preload and afterload, are contraindicated in pregnancy, since their use in the latter half of pregnancy is known to cause oligohydramnios, intrauterine growth retardation, neonatal renal failure, hypotension and death.16,28 ACEIs and ARBs may be used postpartum after counselling women regarding potential risks in future pregnancies. Hydralazine and nitrates are the preferred vasodilators in pregnancy. 31 Beta-blockers and calcium channel blockers have also been shown to prolong longevity in women with HF.1,17 Digoxin improves symptoms, quality of life and exercise tolerance by attenuation of the neurohormonal system and increasing myocardial contractility, and has been used safely in pregnancy. 32 Ivabradine is a sinus node inhibitor which is known to improve outcomes in women with reduced EF and tachycardia 33 but is not currently used in pregnancy.
Anticoagulation needs to be considered in atrial fibrillation, a history of thromboembolism or LVEF of under 35%. 32 None of the women in our cohort were found to have atrial fibrillation but a reduced LVEF and cardiogenic shock were associated with poor maternal outcomes. Implantable cardioverter defibrillators may be used when indicated to prevent sudden cardiac death in women. 34 Other possible therapeutic modalities include immunosuppressive therapy, such as azathioprine and prednisolone, intravenous immunoglobulin or cardiac transplantation.35–37 Bromocriptine has a theoretical role in view of its role in stimulating hypothalamic dopaminergic receptors and thereby inhibiting prolactin secretion.38,39 Other drugs which are being evaluated in the management of PPCM include pentoxyfylline and levosimendan.40,41
With regard to obstetric management, vaginal delivery is preferred in women with compensated HF, while LSCS is reserved for women who are decompensated or in cases of fetal distress. It is advisable to shorten the second stage of labour with the use of forceps or suction devices to reduce cardiac work. 37 While 59.3% of our women underwent an LSCS, 9.3% underwent operative vaginal deliveries.
Prior studies have reported recovery of LV function, mostly within the first six months, in 45%–78% of women. 42 Review echocardiograms were available for 20 women in our study with a mean follow-up of 24.2 months. The mean EF on review echocardiography was 53.7 ± 4.5%.
Women should be advised on the risk of recurrence of PPCM in subsequent pregnancy, and on the safest and most effective contraceptive method, by both their cardiologists and obstetricians. Rest and stress echocardiography should be advised in women planning for subsequent pregnancies. 1 Baseline LVEF prior to the subsequent pregnancy must be determined three months after the discontinuation of ACEIs or ARBs, which are contraindicated in pregnancy. Early termination of an unintentional pregnancy should be considered to prevent worsening of LV function and potential maternal mortality, in women with persistent LV dysfunction.
Conclusion
In this study conducted on women diagnosed with PPCM from southern India, adverse maternal outcomes were noted to be associated with lower LVEF and cardiogenic shock. There were no significant associations seen with traditional risk factors for PPCM such as hypertension, maternal age or multiple pregnancies. Mild-to-moderate anaemia (Hb 80–110 g/l) was found to be associated with adverse fetal outcomes. Nearly 40% of women had follow-up echocardiographic data, with most of them showing a significant recovery of LVEF. Women need to be counselled against further pregnancies in view of chances of recurrence of PPCM. To the best of our knowledge, this is the largest series of women with PPCM studied in India. Further multi-centre, prospective studies are encouraged to assess newer modalities of diagnosis, therapeutic response and novel management strategies.
Limitations
This study was limited by its retrospective and observational nature, and unavailability of follow-up data in a significant proportion of women.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Permissions obtained from heads of units. IRB not required.
Informed consent
Written consent was obtained from the patients for their anonymised information to be published in this article.
Guarantor
AJB.
Contributorship
AJB conceptualized, designed the study, and did the literature review, data collection, analysis and manuscript preparation, editing and manuscript review. SS, SJR, AR, MB, SR and VST were involved in conceptualization and design of the study and in the manuscript editing and review process.