
Abstract
Tachycardia-induced cardiomyopathy is rare during pregnancy and is reversible when the underlying arrhythmia is effectively treated. Management can be complex due to the risks of antiarrhythmic medications and cardiac interventions on the developing fetus. The care requires a well-coordinated multidisciplinary team of cardiologists, electrophysiologists, and maternal-fetal specialists. In this report, we describe a case of recurrent atrial tachycardia-induced cardiomyopathy in pregnancy.
Case
A 30-year-old woman, with no personal or family history of heart disease, attended her first antenatal visit at 11 weeks of gestation. At this time, she was found to have an asymptomatic atrial tachycardia (AT) with 1:1 conduction and a heart rate varying between 140 and 180 beats per min. On examination, it was found that her blood pressure was 120/60 mmHg, body mass index was 35.8 kg/m2, oxygen saturation was 99% on room air, heart sounds were normal, and lung fields were clear. A transthoracic echocardiogram showed severe left ventricular (LV) dysfunction with a left ventricular ejection fraction (LVEF) less than 20%, a mildly dilated LV, an LV apical thrombus, and normal right ventricular systolic function with no signs of pulmonary hypertension. She was started on intravenous low molecular weight heparin (LMWH) along with metoprolol and digoxin for rate control. The high-risk nature of pregnancy was discussed with the woman, and her preference was to continue the pregnancy despite the risks. Initial treatment with metoprolol and digoxin failed to control her heart rate. After the LV thrombus had resolved with heparin therapy, overdrive pacing was attempted but was unsuccessful. The option of ablation was considered, but due to the potential radiation exposure to the fetus, the woman declined, and amiodarone was started. She was discharged after treatment with metoprolol, amiodarone, and LMWH subcutaneously every 12 h. At her discharge, her LVEF had improved (LVEF 30%), and no LV thrombus was visualized. Follow-up with a multidisciplinary team involving cardiologists, electrophysiologists, and maternal-fetal specialists was arranged. The woman remained stable until 30 weeks of gestation when she presented again with recurrent AT and an LVEF of 25%. An attempt at cardioversion was unsuccessful. Due to her poorly controlled AT (Figure 1) and declining LVEF, she underwent an elective caesarean delivery under regional anesthesia at 34 weeks of gestation. A healthy 2480 g baby was delivered. Postpartum, she was closely monitored on a coronary care unit, and her course was uneventful. She underwent an electrophysiology study five days after delivery, and a focal AT arising from the right atrial appendage was identified and ablated. She was followed regularly in the outpatient clinic. Amiodarone was discontinued, and metoprolol and coumadin were continued. At six weeks postpartum recurrent, persistent AT with variable AV conduction was identified, a second ablation was performed successfully. A cardiac magnetic resonance imaging (MRI) with late gadolinium enhancement at six months postpartum showed full recovery of LVEF, with no evidence of myocardial fibrosis. There was no evidence for any other etiology of cardiomyopathy. She was counseled about contraception options given that in the setting of LV systolic dysfunction and LV thrombus, estrogen-containing contraceptives, which can increase the risk of thrombosis, are not recommended and an intrauterine device (IUD) would be the preferred option. At one year and seven months postpartum, she presented with palpitations and was found to be in AT with an average heart rate of 111 bpm. Her echocardiogram showed a significant decline in LVEF to 38%. A positive pregnancy test prompted an ultrasound scan, which confirmed an intrauterine pregnancy at six weeks’ gestation. After a long discussion with the multidisciplinary team, the woman elected to have a termination of pregnancy. One month after termination, she was in sinus rhythm, and an echocardiogram showed normal LV size with mildly decreased LVEF (43%). She was maintained on metoprolol at the same dose. A year later, she presented again with AT (HR 100 bpm) and pregnancy at eight weeks of gestation. She elected to terminate the pregnancy. One week after the termination, her AT converted to sinus rhythm. Contraception was prescribed, she has been followed closely for five years and had no recurrence of AT, and her LV systolic function has remained normal. The three episodes of AT-induced LV dysfunction occurred only in the context of pregnancy.
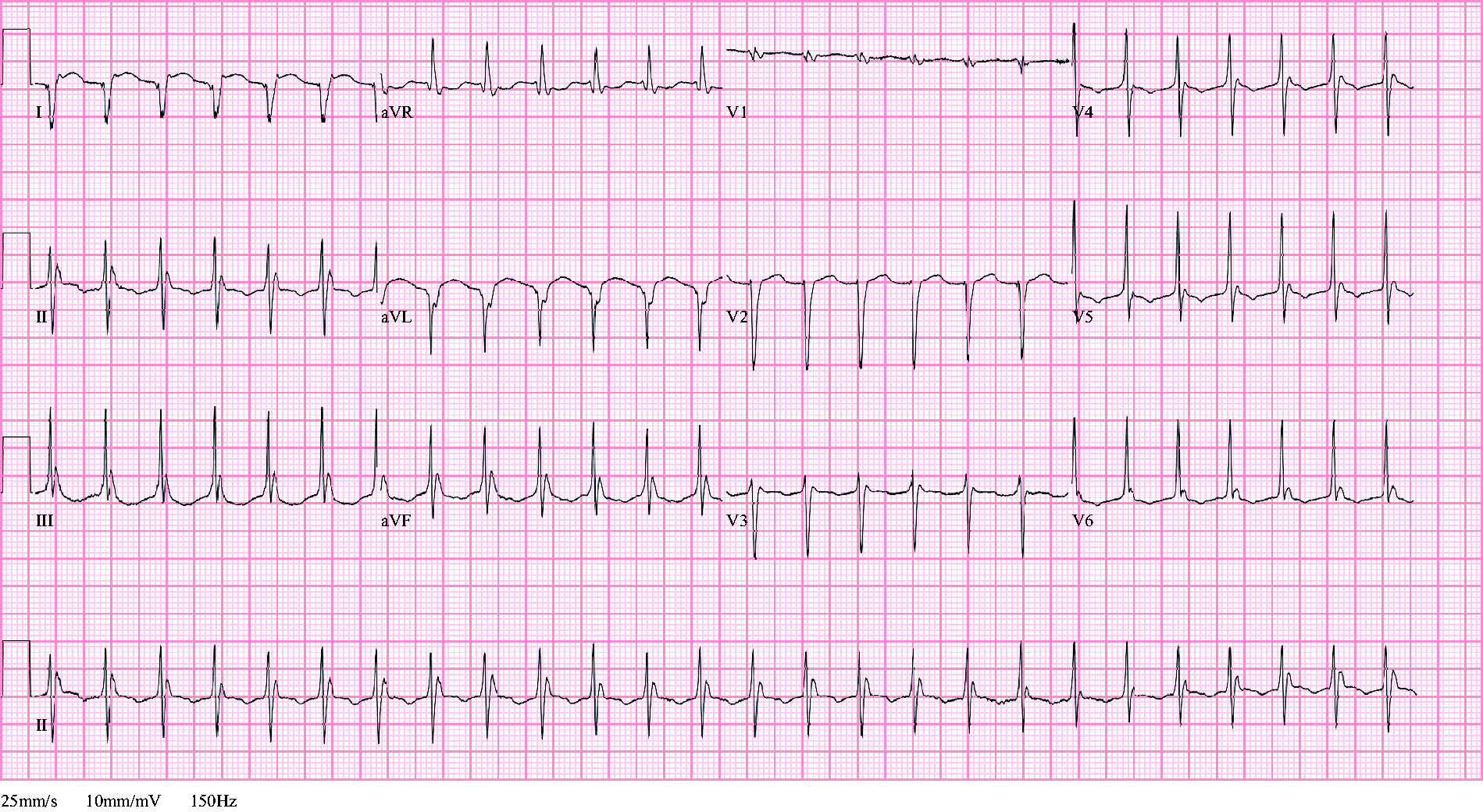
Maternal electrocardiogram at 12 weeks of gestation showing an atrial tachycardia with a ventricular rate of 155.
Discussion
Persistent tachycardia can lead to ventricular dysfunction and heart failure. The diagnosis of tachycardia-induced cardiomyopathy is confirmed if the individual presents with a persistent tachycardia, if other causes of LV dysfunction are excluded, and if ventricular function normalizes after reinstitution of normal heart rate. 1 Although arrhythmias are one of the most common cardiac complications in pregnant women, 2 tachycardia-induced cardiomyopathy is very rare and can be life-threatening for the mother. During pregnancy, increases in atrial and ventricular stretch, maternal heart rate, and changes in adrenergic receptor sensitivity, likely all contribute to an increased propensity to arrhythmias. 3 Incessant AT is defined as AT present for more than 90% of the time and may develop during pregnancy because of the sensitivity of the ectopic focus to autonomic modulation. 4 The challenge of discerning right atrial tachycardia from sinus tachycardia is important. The management of inappropriate sinus tachycardia is purely supportive, whereas AT requires treatment. Controlling AT can be difficult, not only because these arrhythmias are often not responsive to antiarrhythmic therapy, but also because ablations are technically challenging. Pregnancy further impacts treatment as the use of antiarrhythmics needs to be weighed against the potential effects of the medication on the fetus. Metoprolol, digoxin, verapamil, and flecainide are potential medication options during pregnancy because they are not teratogenic and have been used in pregnancy to treat other supraventricular arrhythmias. However, verapamil and flecainide are not typically used in the setting of significant LV systolic dysfunction. Higher doses of metoprolol or digoxin may be needed during pregnancy. Beta-blocker exposure during pregnancy has been associated with low birth weight babies, fetal bradycardia, and neonatal hypoglycemia. Amiodarone is used to treat AT outside of pregnancy but is typically not used during pregnancy because it can lead to fetal thyroid dysfunction. 5 However, when women present with refractory arrhythmias, especially in those with ventricular dysfunction, the benefits of amiodarone may outweigh the fetal risks. Decisions about Amiodarone use in pregnancy must be made in conjunction with the mother. For drug-refractory AT, consideration of minimal or no fluoroscopy-guided ablation procedures can be considered5,6; however, at the time this woman first presented to hospital, fluoroless catheter ablation was not available at our center. Although experience is limited during pregnancy, successful cases of ablation of AT with and without fluoroscopy during pregnancy have been described in the literature.7–9 This rare form of cardiomyopathy is reversible when the underlying arrhythmia is effectively treated. The care for pregnant women with tachycardia-induced cardiomyopathy is a complex task, which requires a well-coordinated multidisciplinary team of cardiologists, electrophysiologists, and maternal-fetal specialists.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Rohan D’Souza, MD has received speaking honoraria and grant funding from Ferring Canada Inc for projects on labour induction, which are unrelated to this publication.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Mount Sinai Hospital does not require ethical approval for reporting individual cases.
Informed consent
Written informed consent was obtained from the patient for the anonymized information to be published in this article.
Guarantor
BP is the guarantor of the present work.
Contributorship
BP wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.