
Abstract
We present the case of a healthy nulliparous woman who presented with persistent fever, proteinuria and elevated transaminases at 33 weeks’ gestation. Following initial treatment for suspected chorioamnionitis and potential pre-eclampsia, she had a caesarean section delivering a healthy male infant. However, on her third post-operative day, she developed neurological symptoms and accompanying severe sepsis, necessitating inotropic support and transfer to a higher level of care. A comprehensive work-up revealed herpes simplex Virus-2 (HSV-2) in serum and cerebrospinal fluid. Abdominal imaging was suggestive of accompanying hepatitis with micro-abscesses. This lady recovered well following intravenous acyclovir for 14 days. Her infant was not affected and was discharged home with his mother. Herpes simplex encephalitis and hepatitis associated with HSV-2 have been described three times previously in pregnancy. We delineate the diagnostic challenges that rare conditions such as this pose and emphasise the importance of multi-disciplinary care in managing complicated medical conditions in pregnancy.
Introduction
Herpes encephalitis and hepatitis are uncommon conditions in non-pregnant individuals, with fewer than 20 cases reported in the literature. We describe the case of a woman at 33 weeks’ gestation who was diagnosed with herpes encephalitis and hepatitis following presentation with a pyrexia and proteinuria at a routine antenatal check. We delineate the natural history of this woman’s condition and the diagnostic and therapeutic steps that were required to successfully treat this woman.
Case report
A 29-year-old lady booked in her first pregnancy at 13 weeks’ gestation with a normal body mass index, and no significant past medical history. Her antenatal course was uneventful, until review at 33 weeks and 5 days of gestation when she presented with a 3-day history of headache and right upper quadrant (RUQ) pain. Blood pressure was normal, but she had significant proteinuria (3+). She also complained of vaginal discharge but ultrasound, speculum and a non-invasive immunoassay test was negative. At planned review and admission the following day, she additionally complained of malaise, rigors and night sweats, with a pyrexia at home. Her blood results at this point are shown in Table 1, with a protein creatinine ratio of 50 mg/mmol. She was pyrexial and broad spectrum antimicrobial cover (benzylpenicillin/gentamicin/clindamycin as per local hospital protocol) was commenced as there was no focus evident. The pyrexia continued and an extended respiratory virology PCR test was sent with escalation of benzylpenicillin to meropenem. A liver ultrasound was non-contributory. At this point (day 4 of admission), the woman noted new onset lower abdominal pain and vaginal discharge. Haematological and biochemical parameters were deteriorating (Table 1). Amniotic membrane rupture was diagnosed, and given ongoing maternal pyrexia and tachycardia in the setting of preterm prelabour rupture of membranes, a caesarean section was performed, delivering a male infant in good condition.
Blood results from 28 weeks’ gestation until 20 days post-operative.
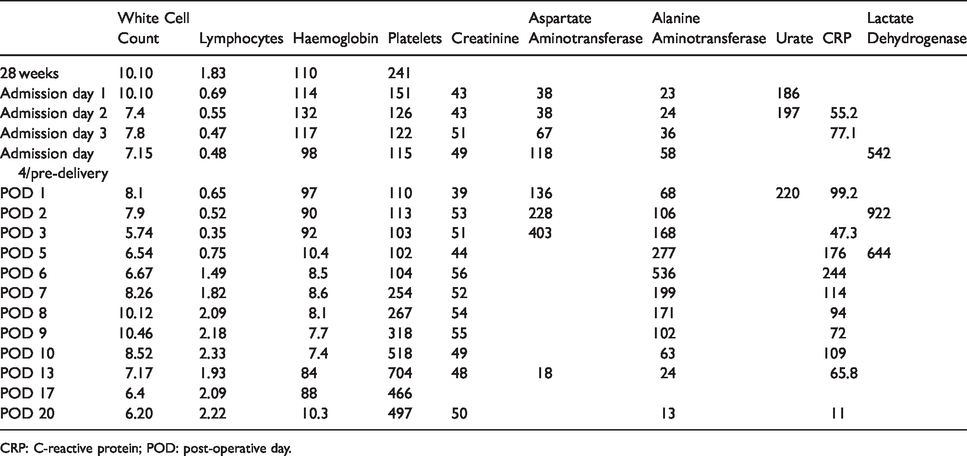
CRP: C-reactive protein; POD: post-operative day.
Her postnatal recovery was initially uneventful, with de-escalation of antibiotics after 48 hours owing to sterile blood cultures. However, on day 3 post caesarean, she reported new onset confusion, accompanied by a further pyrexia. Examination revealed only submandibular lymphadenopathy and lower abdominal tenderness. Repeat blood work was processed, to include a detailed viral and autoimmune screen (Table 1). Over an 8 hour period, she deteriorated and developed septic shock with hypotension and tachycardia refractory to treatment. This required inotropic support and she was transferred to a general hospital under hepatology for critical care support and management of sepsis.
On review at this juncture, severe RUQ pain persisted, with intermittent confusion and pyrexia. The woman had a transaminitis, with thrombocytopenia and an elevated C-reactive protein (CRP). She was hypoalbuminaemic (21 g/L), with a normal white cell count and bilirubin with normal coagulation parameters. A computed tomography (CT) scan of the abdomen and pelvis revealed no abdomino-pelvic collection, but the liver was diffusely abnormal with marked periportal oedema and minute hypodensities (Figure 1). These findings suggested an acute hepatitis, and pending results, we continued broad-spectrum antimicrobials.

Computed tomography cross section demonstrating hepatic changes.
Subsequently, serum herpes simplex virus 2 (HSV-2) PCR sent prior to transfer returned positive. A lumbar puncture was performed, detecting HSV-2 in cerebrospinal fluid. There was no previous history of HSV-2, and no active muco-cutaneous lesions on examination. Primary infection was diagnosed by assessing serology from 13 weeks’ gestation, as this was negative for HSV-2 IgG. Intravenous acyclovir was initiated. Over the coming days, she remained afebrile and there was an improvement in her symptomatology, biochemical and inflammatory parameters. Inotropic support was weaned and care was de-escalated to a ward.
A repeat CT abdomen/pelvis was performed for recurrent severe RUQ pain, demonstrating stable extensive periportal oedema. The number of hypodensities had increased significantly and was consistent with micro-abscesses secondary to HSV-2 viraemia; this illustrates the severity of the infection. With timely diagnosis and early initiation of anti-viral treatment, improvement was seen.
Intravenous acyclovir was continued for two weeks. She made a full recovery and was discharged home on the same day as her son.
Discussion
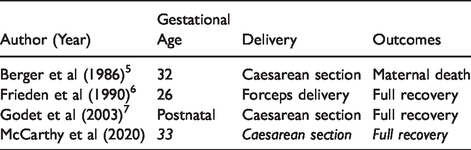
HSV-2 is associated with 10% of herpes encephalitis cases, and is most common in neonates, the immunocompromised and the elderly. 1 In the non-pregnant women mortality rates can escalate to more than 70% in the absence of prompt treatment. 2 It is most commonly associated with genital herpes, typically presenting with mucocutaneous vesicular lesions; however, these can be absent in up to 50% of cases. 3 Herpes encephalitis in pregnancy is most likely to present in the second or third trimester, presumed due to immunological changes in pregnancy. 4 HSV-2 encephalitis in the pregnant woman has only been described in three previous case reports (see Table 2). 4
Summary of herpes simplex virus-2 (HSV-2) cases in pregnancy.
Similarly, herpes hepatitis causes less than 5% of all acute hepatitis presentations, and pregnancy is associated with significant morbidity. 8 It can rapidly progress to fulminant liver failure, with mortality rates up to 90%. The mortality and morbidity of these conditions have been greatly improved by the utilisation of acyclovir (a nucleoside analogue), which is recommended for 14 days to decrease the risk of relapse. 9
Diagnostic challenges can present frequently in pregnancy, and it is important to consider both obstetric and non-obstetric diseases in the differential diagnosis, as well as to consider concomitant medical conditions. There should be a low threshold for the involvement of the multi-disciplinary team and expansion of the diagnostic test panel to encompass rarer entities. In cases such as this, the prompt recognition of the deteriorating women is essential to ensure timely treatment in order to minimise long-term neurological impairment. In this case, the identification of micro-abscesses was an important diagnostic clue.
We describe the case of a healthy woman who presented with a viral sepsis in the peripartum period, and a subsequent diagnosis of HSV-2 hepatitis and encephalitis. A high index of suspicion for rare non-obstetric conditions is essential to ensure prompt and effective treatment for women to optimise outcomes. The formation of a dedicated multi-disciplinary team is essential in the management of these cases.
Footnotes
Acknowledgements
We would like to thank the wider multi-disciplinary team for their care and management of this woman.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not required for this paper.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Guarantor
Prof M. Geary is the guarantor for this paper.
Contributorship
CMC, MK and MG are responsible for the conception of this article. CMC and CC researched the literature and wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.