
Abstract
Gastrointestinal cancer occurs in approximately 1 in 13,000 pregnancies, making up 4% of malignancies detected in pregnancy. It is a complex and challenging condition to diagnose and manage and is often only detected in its more advanced stages. This is partly due to symptoms of gastrointestinal cancer being incorrectly attributed to physiological symptoms of pregnancy, as well as concerns about the safety of diagnostic investigations in pregnancy, both of which may delay diagnosis and lead to disease progression. Challenges in management also arise from under-treatment in pregnancy due to concerns about the impact of surgery or chemotherapy on the pregnancy. We present here three cases of gastrointestinal cancer diagnosed in pregnancy in our centre and discuss the challenges and pitfalls one may encounter in the diagnosis and management of gastrointestinal malignancies in pregnancy.
Introduction
The incidence of cancer in pregnancy has doubled over the past four decades to reach approximately 1 in 1000 pregnancies at present, likely related to the rising age of the maternity population, as well as more frequent examinations in pregnancy that lead to increased detection rates.1–3 The overall pregnancy-related mortality rate from malignancies was 4.4 per 100,000 maternities in the most recent MBRRACE-UK 2018 report. 4 Gastrointestinal cancer occurs in approximately 1 in 13,000 pregnancies, making up 4% of malignancies detected in pregnancy. 5 It is often a devastating diagnosis for both mother and fetus due to it often being detected in advanced stages of the disease and having the highest association with neonatal intensive care unit admission compared to other malignancies in pregnancy. 5
We present three cases of gastrointestinal cancer diagnosed in pregnancy in our centre over 12 months and discuss the challenges and pitfalls one may encounter in the diagnosis and management of gastrointestinal malignancies in pregnancy.
Case 1
A 45-year-old nulliparous woman was admitted at 13 weeks’ gestation with intermittent left iliac fossa (LIF) pain, vomiting and constipation. She had had an episode of bleeding per rectum prior to conception but a planned flexi-sigmoidoscopy was deferred when she conceived. On admission, examination revealed LIF and suprapubic tenderness with rebound and hard stool per rectum. She was treated for constipation in pregnancy, and her abdominal pain resolved rapidly with analgesia. She was discharged from hospital the subsequent day. At 19 weeks’ gestation, she was readmitted with a five-day history of left flank and LIF pain associated with fever, constipation and vomiting. Examination revealed left flank tenderness with a raised CRP level of 65 mg/L. Initial conservative measures did not result in an improvement of her symptoms; hence an MRI of her abdomen and pelvis was performed. This showed a 6 cm focal mural thickening of the colon at the junction between the descending and sigmoid colon with an adjacent 2 cm abscess. Differential diagnoses included a diverticular abscess or colonic malignancy with perforation. Options presented to the patient were to proceed with a flexible sigmoidoscopy with the risk of exacerbating a perforation, delay the sigmoidoscopy for six weeks to await fetal viability, or repeat the MRI in two weeks for further evaluation. The woman opted for repeat interval imaging which remained unchanged and highly suspicious for a colonic malignancy. Flexible sigmoidoscopy and biopsy performed at 23 + 5 weeks’ gestation diagnosed an invasive adenocarcinoma. The woman was reviewed by the Medical Oncologist at 25 weeks of gestation to discuss therapy aimed at delaying cancer progression and was offered the following choices: (1) Neoadjuvant combination chemotherapy using oxaliplatin with bolus and infusional 5FU (FOLFOX). (2) Neoadjuvant bolus and infusional 5FU alone. (3) Observation alone. She was informed of the paucity of published chemotherapy outcomes in pregnant women with colon cancer. She declined chemotherapy treatment in pregnancy due to concerns about adverse effects on the pregnancy and underwent a planned caesarean section at 33 + 2 weeks’ gestation with concomitant definitive tumour resection. Final histology showed a stage T4b N0 M0 moderately differentiated sigmoid adenocarcinoma, with clear surgical margins. Post-operative adjuvant chemotherapy was declined by the woman, with subsequent early surveillance imaging demonstrating new hepatic lesions suggestive of metastatic deposits.
Case 2
A 37-year-old multiparous African woman with a history of latent tuberculosis treated in 2016 was admitted in 2018 to her local hospital at 23 weeks’ gestation for worsening lower back pain affecting mobility. Investigations revealed a mild neutrophilia, a negative infection screen, unremarkable chest radiograph, and normal renal and abdominal ultrasound. Whole spine MRI performed in view of unremitting pain revealed an L4 lesion with end plate destruction but no disc involvement. The working diagnosis was spinal tuberculosis in view of her history of latent tuberculosis. Consideration was given towards a diagnostic spinal biopsy but not performed due to concerns regarding CT radiation and general anaesthesia in pregnancy, as well as difficulties with accessing the lesion behind the gravid uterus. She was treated with an empirical course of anti-tuberculous therapy and steroids, but her symptoms worsened with development of neuropathic pain down her right leg two weeks later. She was transferred to our unit at 28 weeks’ gestation, and treatment for spinal tuberculous continued after a spinal multidisciplinary team discussion concluded this to still be the most likely diagnosis. Unfortunately, her symptoms deteriorated over the next five weeks. MRI spine repeated at 34 + 2 weeks’ gestation showed disease progression with a new lesion in the T8/L1 vertebra, prompting the decision for delivery. Vertebral body biopsy performed post-delivery revealed adenocarcinoma positive for CK7 and CK20, in keeping with metastatic disease from an upper gastrointestinal tract primary. Oesophagogastroduodenoscopy (OGD) did not detect an obvious gastric lesion, but PET-CT scan was suggestive of metastatic cancer. The woman deteriorated rapidly and passed away six weeks post-delivery. Final autopsy confirmed metastatic linitis plastica of the stomach.
Case 3
A 33-year-old primiparous woman with no significant medical history was admitted at 36 weeks’ gestation with generalised abdominal pain associated with vomiting. She had otherwise been well antenatally. Examination revealed the abdomen to be distended, and an epigastric mass was intermittently palpable behind the fundus of the uterus. Haemoglobin level was 105 g/L with normal mean corpuscular volume (MCV) of 86 FL on admission. MRI of the abdomen revealed a partially obstructive, locally advanced 6 cm transverse colon tumour. CEA level was normal at 1.5 µg/L. A multidisciplinary team discussion between the obstetricians, obstetric physicians, general surgeons and anaesthetists was held to decide on the optimal timing and mode of delivery. The woman underwent an uncomplicated elective caesarean section with a concomitant extended right hemicolectomy with end-to-end anastomosis at 37 weeks of gestation. She recovered well post-operatively without any complications and was discharged on post-operative day 4 together with her baby. Final histology revealed a moderately differentiated adenocarcinoma of the transverse colon with 3 out of 25 lymph nodes detected positive for malignancy. Immunohistochemistry of the tumour noted an isolated loss of PMS2. A staging CT chest was performed postnatally which did not show any evidence of metastatic disease, putting the stage of the tumour to be at pT3 N1b M0 or AJCC stage IIIB, and the woman was recommended for adjuvant chemotherapy.
Discussion
The incidence of gastrointestinal cancers is estimated at 1 in 13,000 pregnancies, with the majority being colorectal cancer, the third most common cancer in females in the UK with approximately 18,700 new cases diagnosed in 2015. 6 The incidence of young-onset cases of colorectal cancer in women between 20 to 49 years of age is increasing, now accounting for 11% of colon cancers and 18% of rectal cancers.7,8 Furthermore, the mortality rate of women with young-onset colorectal cancers increased by 13% from 2000 to 2014. 7 Given these statistics, gastrointestinal cancer in pregnancy is certainly a condition that clinicians may encounter at some point in their career, and they should therefore be aware of the principles of its diagnosis and management.
However, gastrointestinal cancer is a complex and challenging condition to manage in pregnancy for several reasons.
Firstly, symptoms of gastrointestinal cancer, such as abdominal pain or discomfort, constipation, rectal bleeding, bloating, loss of appetite, nausea or vomiting and fatigue, often overlap with those seen in pregnancy, and may therefore initially be incorrectly attributed to physiological symptoms of pregnancy, resulting in delays in investigation and treatment, thereby leading to potential disease progression. 9 This was seen in the patient in Case 1 where her symptoms of lower abdominal pain, vomiting and constipation in the first trimester were initially thought to be pregnancy related. Advanced metastatic disease may also sometimes present with symptoms that are also experienced in pregnancy, such as lower back pain, which was seen in Case 2. A systematic approach to history-taking is therefore vital, specifically looking out for red flag symptoms that would warrant an earlier and more in-depth investigation, for example, persistent or recurring symptoms, recurrent presentations for the same complaint or worsening severity of symptoms.
Secondly, another challenge faced in diagnosing gastrointestinal cancers in pregnancy is the concern surrounding imaging such as computed tomography (CT) scans and magnetic resonance imaging (MRI). Ionizing radiation in imaging modalities such as X-rays and CT scans carry with it the risks of fetal exposure causing teratogenicity, carcinogenesis and genetic mutations in germ cells. However, these risks are largely dependent on the gestational age at the time of exposure, the dose of radiation received and the anatomic location of interest.10,11 Table 1 illustrates the effects of gestational age and radiation dose on the fetus, 12 and Table 2 illustrates fetal radiation doses associated with common radiologic investigations. 13 The patient in Case 2 had a delayed diagnosis partly due to concerns about radiation from a CT-guided spinal biopsy, which might have contributed to the eventual poor outcome. When clinically indicated, imaging modalities utilizing ionizing radiation should thus not be deferred simply because of a perceived (and unsubstantiated) risk to the fetus. In the case of MRI, this is in itself considered a safe modality during pregnancy, although there has been some controversy surrounding the safely of the gadolinium-based contrast used to increase the specificity of this technique. In particular, gadolinium has been thought to potentially cause fetal connective tissue complications such as nephrogenic systemic fibrosis (NSF) or skin disease. A large retrospective study looking at the long-term safety after MRI exposure in pregnancy found that although there was no statistically significant difference in NSF-like outcomes between fetuses exposed to and not exposed to gadolinium, there was an increased risk of rheumatological, inflammatory or infiltrative skin conditions in those exposed during the first trimester. 14 However, limitations of this study made it difficult to conclusively prove the adverse effect of gadolinium on the fetus. Most guidelines thus advise for gadolinium use to be limited to cases where benefits clearly outweigh potential risks.15–17 All three women underwent antenatal MRI scans without gadolinium contrast, which proved instrumental in leading to the final diagnosis of cancer.
Effects of gestational age and radiation dose on fetus.
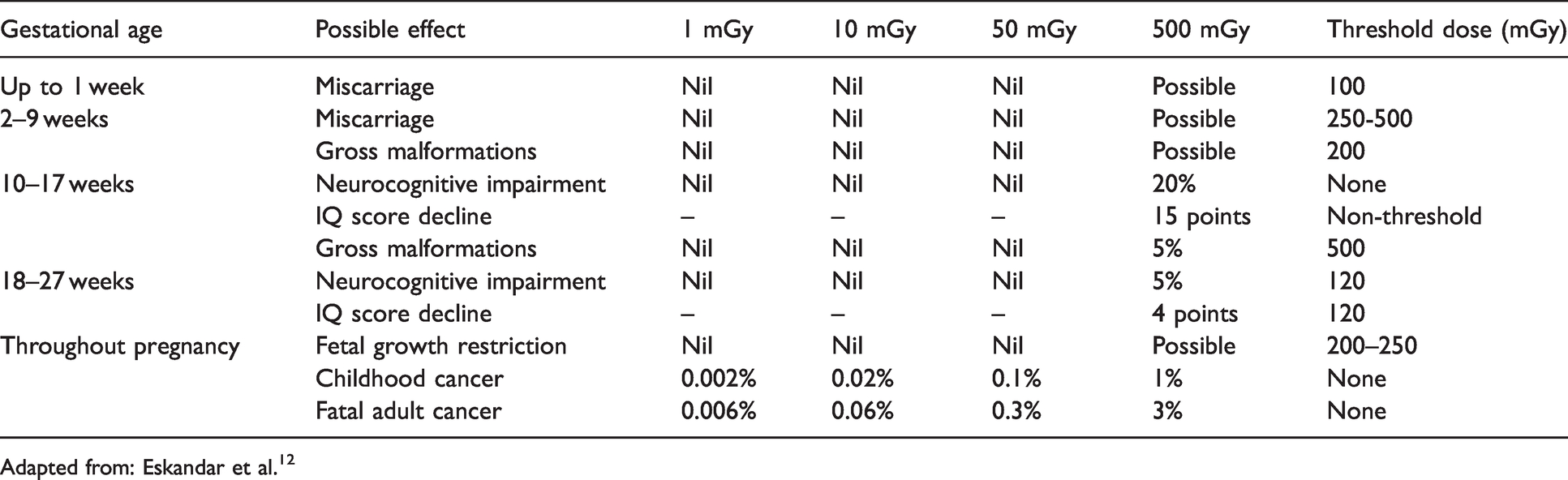
Adapted from: Eskandar et al. 12
Fetal radiation doses associated with common radiologic examinations used in the workup of gastrointestinal malignancies.

aFetal exposure varies with gestational age, maternal body habitus and exact acquisition parameters.
Adapted from: Tremblay et al. 13
Alongside radiological investigations, endoscopic procedures such as oesophagogastroduodenoscopy, sigmoidoscopy and colonoscopy are often integral in the diagnostic workup for gastrointestinal malignancies. Traditionally, the perceived risks of endoscopy in pregnancy include preterm labour, trauma, hypoxia and teratogenesis. However, studies have shown that both upper and lower GI endoscopy are safe in pregnancy albeit in the case of colonoscopy, greater colonic preparation, increased requirement for sedation and analgesia and longer procedure time have all been reported.18–32 Endoscopy should thus not be deferred in the presence of a strong indication such as suspected malignancy, particularly if presentation occurs after the first trimester. The patient in Case 1 had a strong indication for colonoscopy in view of the MRI findings of a suspicious lesion. However, due to her concerns about the risks of the procedure on the pregnancy, she opted to defer this, leading to delayed diagnosis and potential upstaging during the intervening period.
A definitive diagnosis of cancer cannot be achieved without histology. Unfortunately, there is often hesitancy to proceed with biopsies in pregnancy due to concerns regarding accessing internal structures in gravid women and risks of miscarriage or preterm birth. As an example, the vertebral body biopsy in Case 2 was delayed in part due to concerns regarding accessing the spinal lesion, which led to the diagnosis only being made 12 weeks later. If the suspicion of malignancy is sufficiently high, performing a biopsy is essential to allow prompt diagnosis, early specialist referral and multidisciplinary discussion, and ultimately consideration of earlier treatment of cancer.
Challenges in management
The management of gastrointestinal cancers in pregnancy should not differ greatly from that of non-pregnant individuals, although the challenge is in balancing oncological and pregnancy outcomes. As recommended in the 2015 MBRRACE-UK Report, treatment for all women with cancer in pregnancy should be the same as for cancer in non-pregnant women, unless there is specific evidence that to do this would cause harm. 33 The report also highlighted that the same targets for diagnosis and treatment times should apply in pregnant and postpartum women as for non-pregnant women. 33 The prognosis of gastrointestinal cancers is not inherently worsened by pregnancy itself, 34 although delayed diagnosis from reasons discussed above and hesitancy to start treatment in pregnancy may negatively affect outcomes. Difficult conversations regarding termination of pregnancy, iatrogenic prematurity or intentional delayed treatment of the malignancy with its inherent risks of progression of disease may have to be undertaken. The final decision depends largely on the patient’s wishes, type and stage of cancer, gestational age of the pregnancy and the estimated risk/benefit ratio of specific treatments for the cancer.
Surgical resection is the mainstay of curative-intent treatment for most gastrointestinal cancers and if required, should not be significantly delayed because of pregnancy. Surgery in the first trimester is avoided because of the increased risk of miscarriage,35–37 and abdominal surgery in the third trimester carries with it the risk of preterm labour and is also more technically difficult due to the significantly gravid uterus. The second trimester is thus the ideal period for surgery to be performed, preferably before 20 weeks’ gestation when the uterus is still relatively small, 38 and when miscarriage rates for pregnant women undergoing surgery are similar to that of the general population.34,38 If diagnosed later in pregnancy, the option of definitive oncological surgery at the time of a planned caesarean section can be considered, as demonstrated in Case 1 and Case 3. Alternatives for discussion include termination of pregnancy, depending on gestation, then proceeding on to definitive treatment, or chemotherapy prior to surgery as neoadjuvant treatment or as a holding measure for fetal maturity before definitive surgery.
In gastrointestinal cancers, chemotherapy is indicated either as neo-adjuvant therapy (prior to definitive treatment such as surgery), adjuvant therapy (post-surgery), or for palliation. In the pregnant woman, chemotherapy during the first trimester is not recommended due to the increased risk of miscarriage, teratogenicity and congenital malformations. 39 During the second and third trimester of pregnancy, women should be counselled that the published literature indicates that chemotherapy appears to be largely safe in terms of fetal and obstetric outcomes in a wide selection of cancers. However, the caveat is that the number of women involved in these case series and reports remains small, especially when broken down by tumour type. In addition, the number of cases involving specifically gastrointestinal cancers are too few to allow for assessment of efficacy. In international case series, breast cancer constitutes the majority of cases, and therefore it is in this patient cohort that most of the reassuring data exist on drug safety and efficacy, particularly for anthracyclines, cyclophosphamide and 5-fluorouracil.5,40–42 In addition, there are also important differences between breast and gastrointestinal cancers in the dosing of certain drugs that form part of key combination protocols, which require care when making across-tumour comparisons. As an example, in the case of 5-fluorouracil, this drug is given as an intravenous bolus at 600 mg/m2 every three weeks in breast cancer, whereas it is given as an intravenous bolus at 400 mg/2 followed by a 46 h infusion at 2400 mg/m2 every two weeks in colon cancer. For colon cancer cases, there is still paucity of safety and efficacy data for the use of infusional 5-fluorouracil during pregnancy, with the additional issues of altered pharmacokinetics during pregnancy. There is also the issue of a possible increased risk of small-for-gestational-age neonates in pregnant women with cancer, especially when chemotherapy is administered during pregnancy, 5 which may expose the infants to an increased risk of perinatal mortality and morbidity. It would therefore be prudent to have close obstetric biometric and Doppler surveillance especially during and after chemotherapy administration.
The patient in Case 1 was offered neo-adjuvant chemotherapy, but chose to delay treatment despite the risks of cancer upstaging, as she was worried about the effects of chemotherapy on her pregnancy. The issue of maternal and fetal safety should be considered in tandem with the issue of efficacy of chemotherapy treatment during pregnancy.
Another factor that is likely to play a big role in patient outcomes is that of clinicians’ knowledge and attitude toward management of cancers in pregnancy, which often vary from one clinician to another. A survey in 2012 looking at current clinical practice for the management of cancer in pregnancy found termination of pregnancy, delay of maternal treatment and iatrogenic preterm delivery to be frequently applied strategies in the management of pregnant cancer women, suggesting that the current treatment was not in line with evidence-based guidelines. 43 This was similarly observed in Case 1 where there was a general reluctance to pursue treatment antenatally until a much later stage in pregnancy, and in Case 2, a hesitancy to pursue investigations to achieve a definitive diagnosis. This highlights the importance of a multidisciplinary team of specialists from the various relevant areas who could advise on what the optimal treatment of cancer would be for a non-pregnant patient. By using this as a starting point for discussion, then bringing in other factors such as gestational age and the patient’s wishes for individualization of treatment plans, one would be able to better ensure provision of the best recommended care for the patient.
Lastly, one must not forget that cancer is a major risk factor for venous thromboembolism (VTE) in pregnancy because of its prothrombotic effect, not to mention the inherent hypercoagulable state of pregnancy. This may be further increased by any dehydration resulting from nausea and vomiting related to chemotherapy. Undertaking regular VTE risk assessments in pregnancy and considering thromboprophylaxis with low-molecular weight heparin is thus extremely important, particularly in higher risk individuals such as those who are obese or older (more than 35 years of age).
Conclusion
Gastrointestinal cancer in pregnancy, with its increasing prevalence, is an important condition of which all clinicians should have a good knowledge of its basic principles of management. It requires a high index of suspicion for diagnosis as many of its symptoms overlap with physiological symptoms experienced in pregnancy, thereby potentially delaying the diagnosis. Clinicians in a multidisciplinary setting need to recognise the common pitfalls one may encounter in the diagnosis and management of gastrointestinal cancers in pregnancy, avoid delays in investigations if suspicion for malignancy is high, and use evidence-based information to counsel women appropriately on their recommended treatment plan, so as to achieve the best possible outcome for them.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Written informed consent was obtained from either the patient or a legally authorized representative for their anonymized information to be published in this article.
Guarantor
CNP.
Contributorship
CNP conceived the study. ST and JM researched literature and wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.