
Abstract
Neurological and neurosurgical conditions complicating pregnancy may precipitate considerable concern regarding the risk of complications, and uncertainty regarding the preferred mode of delivery and anaesthesia. Caesarean section is known to be associated with significantly increased risk of adverse maternal outcomes compared with vaginal delivery in healthy pregnancy. Nevertheless, a common perception exists among the general population and some health professionals that caesarean section is safer for the mother and baby in high-risk pregnancies. This manuscript examines the literature regarding the risks and outcomes related to mode of delivery in pregnancy complicated by disorders of the central nervous system. With the exception of women with raised intracranial pressure, and some women with Von Hippel-Lindau syndrome, the available evidence suggests that the mode of delivery should be based upon obstetric indications.
Introduction
It is not uncommon for women with high-risk pregnancies to be advised by health professionals to have delivery by caesarean section (CS) rather than vaginal delivery (VD) because of the perception that the former is “safer” for mother and baby. No randomised trials have been performed assessing the risks and benefits of VD or CS for women with no conventional medical indication for CS. 1 A retrospective cohort study which compared planned CS in 47,000 women with planned VD in 2,292,000 women found that CS was associated with a significantly increased risk of puerperal infection (OR 3.0), venous thromboembolism (OR 2.2), anaesthetic complications (OR 2.3), hysterectomy (OR 3.2), postpartum haemorrhage and wound haematoma (OR 5.1), and maternal death from cardiac arrest. 2 A prospective multicentre study assessing the outcome of 97,095 deliveries found that compared with VD, elective CS was associated with increased risk of major maternal morbidity (OR 2.3) and maternal death (OR 3.38). 3 Serious maternal morbidity progressively increases with the number of previous CS.4,5 Neurological conditions may result in additional considerations with respect to mode of delivery and anaesthetic techniques in these women. This review examines the available evidence regarding mode of delivery in pregnancies complicated by neurological and neurosurgical disorders affecting the central nervous system (CNS).
Methods
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 6 A MEDLINE search utilising PubMed, EMBASE and Google Scholar between 1960 and 1 December 2019 was conducted using the terms “pregnancy” and individual conditions affecting the central nervous system. Abstracts were used to filter results. Manuscripts were included that compared the outcome with VD or CS in the setting of CNS disorders. The lists of references from review articles, case series and case reports obtained were manually reviewed to identify additional studies. Eligible studies were peer reviewed and published in English. This is a qualitative analysis, thus no statistical analysis was undertaken. This was primarily due to the studies being retrospective in nature, and the small number of studies related to each condition.
Results
The search strategy resulted in 3403 articles for screening, from which 296 full text articles from 1961 to 2019 were assessed for eligibility (Figure 1). One hundred and ninety-three full text articles were excluded as they did not address outcomes with mode of delivery. One hundred and three manuscripts were eligible for qualitative synthesis, consisting of 63 retrospective case studies, 22 review articles, 14 case reports, three consensus statements and one prospective study.

Flowchart of study search and selection.
Cerebral arteriovenous malformation
Cerebral arteriovenous malformations (cAVM) occur in approximately 0.01% of the population. 7 Studies examining as to whether pregnancy is associated with increased risk of cAVM rupture have yielded conflicting results. Six studies totalling 1175 pregnancies found an increased risk of AVM rupture during pregnancy compared with control women, with odds ratios varying from 1.9–8.18. 8 Conversely three studies totalling 1040 pregnancies found no increase in rate of cAVM rupture as a result of pregnancy.9–11 Overall the risk of rupture during pregnancy varied between 1.6% and 11.1%. The majority of episodes of cAVM rupture during pregnancy occur in the second and third trimester. Several studies have indicated that labour and delivery are not associated with increased risk of AVM rupture.12–14 In a study of 64 pregnancies where cAVM was diagnosed during or after pregnancy, VD (83% of pregnancies) did not increase haemorrhage risk compared with CS. 9 Several authors recommend it is reasonable to perform VD in cAVM without previous rupture. 12,15
Hereditary haemorrhagic telangiectasia (HHT) accounts for approximately 2% of cases of cAVM. Multiplicity of cAVMs, recurrent nosebleeds, iron deficiency anaemia, mucocutaneous telangiectasia, pulmonary or hepatic AVMs or an affected relative should prompt genetic testing for HHT. Major complications have been reported in 5–13% of pregnancies in women with HHT, predominantly in women not examined for pulmonary or cAVMs prior to pregnancy.16–18 A review of 185 live births in women with HHT reported VD in 129 deliveries (70%). 17 Peripartum complications occurred in 10 VD (5%), the most common of which was postpartum haemorrhage. No comparison of adverse outcome between VD and CS delivery was performed. Spinal AVMs occur in approximately 1% of individuals with HHT. 19 Neuraxial anaesthesia was performed in 92 of 185 deliveries in women with HHT without neurological complications without prior screening for a spinal AVM. 17
Cerebral cavernous malformations (cavernomas/cavernous angiomas)
Cerebral cavernous malformations (CCM) have been reported as an incidental finding in 0.4–0.6% of the general population on autopsy and magnetic resonance imaging (MRI) studies. Approximately 20% of cases are estimated to be familial associated with loss of function mutations, and are typically associated with multiple CCMs. The risk of haemorrhage is higher with familial CCM, a previous history of haemorrhage, brainstem malformations, and diameter of CCM greater than 10 mm. Two large studies have assessed pregnancy outcomes. Kalani et al. described 168 pregnancies in 64 women with CCM (28 sporadic, 36 familial). 20 The risk of haemorrhage during pregnancy was 1.8% in the sporadic CCM group, and 3.6% in the familial patients, which is not increased compared with non-pregnant individuals. Vaginal delivery occurred in 149 pregnancies (88%) without complication. A retrospective review of 186 women of child-bearing age found a haemorrhage rate for pregnant women of 1.15% per person-year and 1.01% per person-year for non-pregnant women. 21 Of the 283 live births, 237 (84%) were VD, with no episodes of haemorrhage in the peripartum or postpartum period. The authors concluded that the risk of haemorrhage with CCM is not increased during pregnancy, delivery or postpartum. The synopsis of guidelines for the clinical management of cerebral cavernous malformations states VD is appropriate for most patients unless there is a recent haemorrhage or neurological deficit that precludes VD. 22
Cerebral aneurysm
The reported incidence of subarachnoid haemorrhage (SAH) ranges from 2.8 to 11 per 100,000 pregnancies.23,24 Recent studies have not found an increased risk of aneurysmal SAH (aSAH) rupture during pregnancy or delivery.23,25 Analysis of the Nationwide Inpatient Sample database concluded the risk of rupture of cerebral aneurysm during pregnancy to be 1.4%, and 0.05% during delivery, similar to the risk of rupture in the general population. 23 Similarly a case crossover study estimated the relative risk of aSAH rupture related to pregnancy to be 0.4 compared with the risk of aSAH rupture in the general population. 25 While 70% of deliveries in women with cerebral aneurysm were by CS, there is no evidence that the risk of intracerebral haemorrhage is higher with VD, and the mode of delivery with unruptured aneurysm should be based on obstetric indications.15,23,25,26 Where aneurysmal haemorrhage occurs in early pregnancy, VD may occur after clipping or embolisation has been performed. 27
Cerebellar hemangioblastoma
Cerebellar hemangioblastoma may occur sporadically (75%) or as part of von Hippel-Lindau (VHL) syndrome. It is unclear whether pregnancy is associated with accelerated hemangioblastoma progression.28–30 In a recent series, 10 of 19 (52.6%) deliveries to women with central nervous system hemangioblastoma were by VD, all without morbidity. 31 The authors’ practice was a preference for CS if any signs of raised intracranial pressure were present. MRI of the spine should be performed before neuraxial anaesthesia.
Historically it has been stated that VD is contraindicated with pheochromocytoma in pregnancy; however, this was based upon high mortality rates where women proceeded to labour with undiagnosed pheochromocytoma. Many case reports have described uncomplicated VD with phaeochromocytoma where alpha-adrenergic blockade was adequate. 32 No large study of VHL in pregnancy has reported the frequency of VD versus CS. 33 Adekola et al. suggested that the mode of delivery in women with VHL should be on a case-by-case basis depending on the presence/absence of intracranial tumours, raised intracranial pressure and pheochromocytoma. 34 Neuraxial anaesthesia (spinal and epidural) has been used in the delivery women with VHL without any reports of complications in the literature.34,35
Previous cervical artery dissection
Most cervical arterial dissections occur following trauma. 36 Approximately 1–5% occur in the setting of a heritable connective tissue disorder such as Marfan or Ehlers Danlos syndrome. In 13 pregnancies in women with a past history of cervical artery dissection (CAD) in the absence of a connective tissue disorder, there were no episodes of recurrent CAD or cerebrovascular events during subsequent pregnancy or the puerperia. 37 Six births were by VD and 7 by CS. All pregnancies were at least 12 months after the diagnosis of the primary CAD.
Previous reversible cerebral vasoconstriction syndrome
Only two completed pregnancies have been reported in women with a previous history of postpartum reversible cerebral vasoconstriction syndrome (RCVS). 38 Neither was complicated by recurrence of RCVS. Nine women with a history of RCVS unrelated to pregnancy subsequently completed pregnancies. One delivery was followed by postpartum RCVS. The mode of delivery was not stated.
Neurosurgical shunts
Liakos et al. described the outcome in 105 livebirths in women with cerebrospinal shunts for hydrocephalus. 39 Sixty-one (58%) were VD, and 44 deliveries (42%) were CS. One shunt infection occurred subsequent to CS. Epidural anaesthesia was employed in 24 VD (39%). Anaesthesia for CS was epidural in 19 births (43%), general in 17 births (39%) and spinal in six births (14%). The authors concluded that the presence of hydrocephalus is not a contraindication to vaginal delivery or the use of epidural anaesthesia, and that mode of delivery should be determined by the neurological status of the patient and obstetric indications. 39 Landwehr et al. reviewed 16 pregnancies in women with neurosurgical shunts. 40 Fourteen women (88%) had VD. None of the women delivered vaginally received prophylactic antibiotics, and none had peripartum complications, and the authors concluded that antibiotic prophylaxis is not essential with VD. 40 Two cases of delayed postpartum group B β haemolytic streptococcal (GBS) shunt infection have been described, symptoms onset 38 days and 6 months postpartum.41,42 The mode of delivery was by CS in one case, and not stated in the other. Kane et al. concluded that women colonised with GBS with ventriculoperitoneal shunts should receive perinatal antibiotic prophylaxis. 42 Shunt complications including infections and adhesion around the shunt tip are described more frequently after CS than VD. 43 VD with an early epidural and the option of shortening the second stage are favoured over CS in women with neurosurgical shunts.43,44
Chiari I malformations
A national database survey found that women with Chiari malformation were 2.2–942 times more likely than healthy women to develop severe medical complications during pregnancy including stroke, sepsis, seizures, acute respiratory distress syndrome, preeclampsia and eclampsia. 45 A retrospective case series of 23 pregnancies in women with Chiari malformation found 15 VD (65%) and eight deliveries by CS. 46 There were no adverse neurological outcomes, and seven women had neuraxial anaesthesia without complication. The authors concluded that offering VD with effective analgesia was safe. A multicentre retrospective cohort study of 185 deliveries in 148 patients with Chiari I malformation described 80 VD (43%), 105 deliveries by CS (57%) and neuraxial anaesthesia in 135 (73%) deliveries, all without neurological complications. 47 A review of 51 women with Chiari malformation who had VD, and 62 women who were managed with neuraxial anaesthesia found no complications that could be attributed to the Chiari malformation. 48 The authors concluded that women with Chiari I malformation who are asymptomatic or have headache as the only manifestation can be delivered based upon obstetric indications. 48
Cerebral tumours
The incidence of primary malignant brain tumours in pregnant women is 2.6–15 per 100,000. 49 Pregnancy may provoke tumour growth and clinical deterioration in women with gliomas and meningiomas.50,51 A 2013 literature review found that 59% of women with known gliomas delivered by VD, whereas 66% of women with newly diagnosed glioma during pregnancy delivered by CS. 52 A subsequent systematic review identified 202 women with newly diagnosed and 114 with known gliomas in pregnancy. 50 In women who have stable disease at term, there was no clinical benefit of CS over VD. 50 CS under general anaesthesia is recommended in women with signs of increased intracranial pressure (ICP). A review of 104 cases of intracranial meningioma diagnosed during pregnancy or in the immediate postpartum period found that 42 patients (40%) underwent craniotomy during pregnancy or at the time of delivery, and 62 women had tumour resection post-delivery. 51 Sixty-seven per cent of the pregnancies were delivered by CS, including all preterm births. Of the women who delivered at term, 71% delivered by VD. There were two maternal deaths – one following VD, and the other following CS. The authors noted a group of eight patients who had VD prior to the diagnosis of meningioma. In two cases the diagnosis was made on the first postpartum day, and symptoms may have been precipitated by increased ICP during the second stage of delivery. In the remaining six cases, the diagnosis was made at least seven days postpartum without any indication the mode of delivery contributed to symptoms. The authors concluded that the decision regarding mode of delivery at term should be made by a multidisciplinary team. 51
Epilepsy
Maternal seizures in labour may result in uterine hyperactivity and fetal hypoxia. 53 Seizure frequency before conception is the strongest predictor of seizures during pregnancy. In the EURAP epilepsy pregnancy registry, seizures occurred during delivery in 2.6% of pregnancies treated with carbamazepine or lamotrigine, 1.9% of those treated with phenobarbital, and 1.4% of those treated with sodium valproate. 54 A Norwegian study of 222 consecutive deliveries with a diagnosis of maternal epilepsy reported three women (1.5%) with seizures during childbirth, two of these during CS. 55 Seventy-five per cent were VD, and when corrected for prematurity the rate of CS was not significantly different in women with epilepsy compared with controls. No studies have compared the incidence of seizures during VD compared with CS. As seizures during delivery are uncommon, maternal epilepsy is not regarded as an indication for CS.
Idiopathic intracranial hypertension
No studies have directly compared outcomes with vaginal and caesarean deliveries in women with idiopathic intracranial hypertension (IIH). Two case series and one review of case reports of women with IHH reported VD in 45 of 54 pregnancies (83%), with no adverse neurological outcome.56–58 The increase in intracranial pressure during labour is transient and not harmful to the mother or baby. The mode of delivery with IHH should be based on obstetric indications.59,60 Neuraxial anaesthesia is safe in women with IHH, and preferred if CS is required, as general anaesthesia may be associated with increased cerebrospinal fluid pressure. 60
Moyamoya disease
Historically CS has been preferred in women with moyamoya disease (MMD) because of the hyperventilation and a possible rise in blood pressure occurring during VD. 61 Nationwide surveys of perinatal centres and adult females with MMD in Japan identified 337 deliveries. 62 CS accounted for 240 deliveries (71%). No significant difference in adverse neurological event rate between CS and VD was seen. A single institute reported 20 of 27 deliveries (74%) in women with MMD to be VD with epidural anaesthesia, without adverse event. 63 A review of reported data identified 390 pregnancies to women with MMD diagnosed prior to pregnancy, with no cases of stroke during delivery regardless of the mode of delivery. 64 The authors concluded that VD with epidural anaesthesia if favourable and feasible for women with MMD whose cerebral blood flow is stable. 64
Prior ischaemic stroke
The incidence of stroke in women of childbearing age is approximately 10.7 per 100,000 women. 65 A descriptive study of 35 pregnancies in 23 women with a history of previous stroke included nine pregnancies in four women whose stroke occurred during a previous pregnancy. 65 Eleven women received aspirin and/or heparin. There were no episodes of recurrent stroke. Twenty-nine pregnancies resulted in a livebirth, and there were five miscarriages and one fetal death. Twenty (69%) of the live born infants were by VD. A questionnaire and phone survey of the outcome of 187 pregnancies in 125 women with a history of prior ischaemic stroke found a recurrence rate in subsequent pregnancies of 1% (2/187 pregnancies). 66 Seventy-seven per cent of deliveries were VD. The authors of both papers concluded that the occurrence of an ischaemic stroke should not contraindicate a subsequent pregnancy. A prospective study of 569 pregnancies resulting in 425 births in women with a previous history of cerebrovascular events found that subsequent pregnancy was associated with increased risk of miscarriage, fetal death and hypertensive disorders of pregnancy though no episodes of recurrent vascular events. 67 The mode of delivery was not stated.
A nationwide population-based study in Taiwan demonstrated that compared with women delivered vaginally, CS delivery was associated with a 44.7% higher risk of stroke during the three-month post-delivery period, as well as increased risk in the 6- and 12-month post-delivery periods. 68 This was consistent with two other studies which found a significant correlation between CS delivery and postpartum stroke.69,70 A confounding factor in these studies may have been the hypertensive disorders of pregnancy leading to urgent or premature delivery by CS and their association with postpartum stroke.
Cerebral vein thrombosis
Previous studies describing the outcome of pregnancies in women with prior cerebral vein thrombosis (CVT) disclosed recurrence of CVT in 6/564 pregnancies (1.1%), and non-cerebral venous thrombosis in 11/533 pregnancies (2.1%).71–73 Anticoagulation was not used in 76/299 pregnancies (25%). Miscarriage occurred in 98/586 pregnancies (17%). 71 A systematic review of studies from July 2005 to October 2017 disclosed a crude risk of recurrent CVT in 1/197 (0.5%) during pregnancy with anticoagulation, and 1/73 pregnancies (1.4%) without heparin. The corresponding risks for non-cerebral venous thrombosis were 3/193 pregnancies (1.6%) with anticoagulation and 5/59 pregnancies (8.5%) without anticoagulation. 71 The mode of delivery was stated in only one study, in which 22 of 24 births (92%) were by VD. 72 The authors concluded that a prior history of CVT was associated with low risk of recurrent events in subsequent pregnancy.
Multiple sclerosis
Two studies totalling 419 deliveries in women with multiple sclerosis (MS) (239 VD – 57%), and with neuraxial anaesthesia in 74 women (18%) found no association between mode of delivery or method of analgesia/anaesthesia and the risk of postpartum relapse or disability progression.48,74 A 2019 UK consensus statement on pregnancy in MS concluded that MS should not influence the mode of delivery or analgesia/anaesthesia unless there was significant disability. 75 In women with severe spinal cord disease, autonomic dysreflexia should be considered in the differential diagnosis of preeclampsia.
Limitations
This review is limited by the absence of published randomised or prospective studies addressing mode of delivery in neurological or neurosurgical conditions. The review is based upon retrospective case series, case studies and review articles, with the inherent risks of bias in patient selection for a particular mode of delivery, as well as reporting and publication bias. Incomplete data recording and the tendency to report favourable outcomes may also limit applicability of the data reviewed. For many of the conditions, data were only available on the mode of delivery, without any information regarding the rate of complications of delivery, let alone a comparison between complications with vaginal delivery or caesarean section.
Conclusion
There is a paucity of literature regarding the preferred mode of delivery in women with underlying neurosurgical and neurological conditions. Recommendations regarding the mode of delivery based upon the available literature are summarised in Table 1. In women with evidence of raised intracranial pressure due to intracranial space occupying lesions with mass effect, or obstruction of CSF flow at or above the foramen magnum, neuraxial anaesthesia is associated with a significant risk of herniation, and delivery should be by CS using general anaesthesia. The preferred mode of delivery in women with VHL needs to be based on the assessment of each individual’s clinical features by a multidisciplinary team. In other chronic neurosurgical and neurological disorders, the available evidence suggests mode of delivery should be based upon obstetric indications. Large prospective studies assessing maternal and fetal outcomes are needed to establish guidelines regarding the preferred mode of delivery with neurosurgical and neurological conditions.
Summary of recommendations regarding mode of delivery.
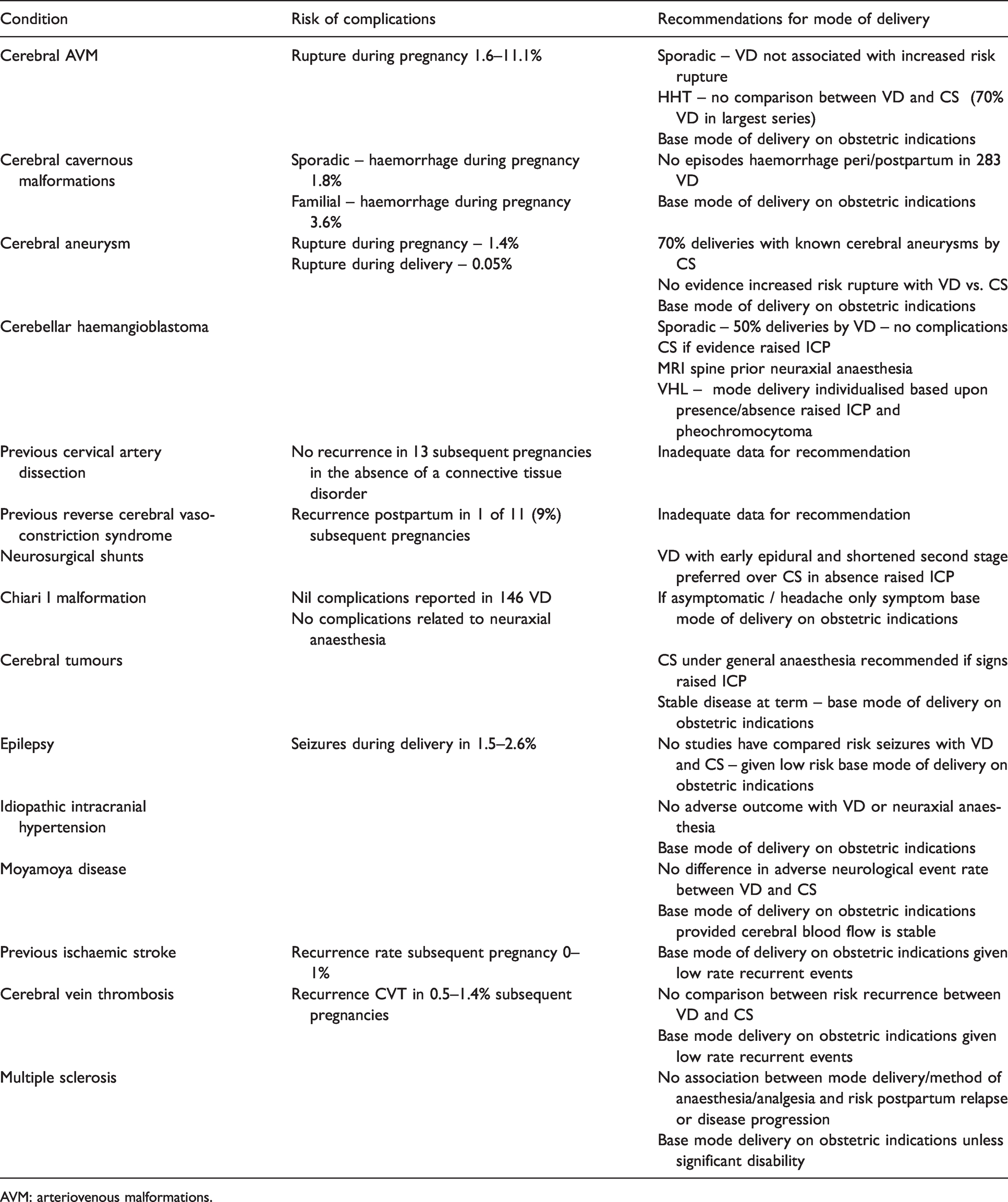
AVM: arteriovenous malformations.
Supplemental Material
sj-pdf-1-obm-10.1177_1753495X211000176 - Supplemental material for Pregnancy complicated by neurological and neurosurgical conditions – The evidence regarding mode of delivery
Supplemental material, sj-pdf-1-obm-10.1177_1753495X211000176 for Pregnancy complicated by neurological and neurosurgical conditions – The evidence regarding mode of delivery by Adam Morton in Obstetric Medicine
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval waived by Mater Health Human Research and Ethics Committee.
Informed consent
Not applicable.
Guarantor
AM is the guarantor of the present work.
Contributorship
AM researched and wrote the manuscipt.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.