
Abstract
Idiopathic intracranial hypertension is more common among women of reproductive age and is often encountered in pregnancy, either pre-existing and exacerbated by pregnancy-associated weight gain and hormonal changes or arising de novo. We report the case of a 33-year-old woman with progressive visual loss and intractable headache from 20 weeks’ gestation requiring ventriculoperitoneal shunting during pregnancy. The risk of permanent maternal vision loss raises complex management dilemmas, when this must be balanced with the fetal and neonatal risks of treatment and possible premature delivery.
Keywords
Introduction
Idiopathic intracranial hypertension (IIH), also known as primary pseudotumour cerebri syndrome, is characterised by elevated intracranial pressure without evidence of an underlying structural or vascular lesion and with normal cerebrospinal fluid (CSF) composition (Table 1). 1 It typically occurs in obese females of reproductive age and is distinguished from secondary intracranial hypertension which is induced by venous thrombosis, medications or endocrine disorders. 1 Clinical manifestations include headache, transient visual obscurations, pulsatile tinnitus and horizontal diplopia, with papilloedema being the hallmark on fundal examination. The incidence of IIH is approximately 15 per 100,000 per year among overweight reproductive-aged females. 2 Pregnant women are over-represented among those seeking treatment, either due to de novo presentation in up to 10% of cases, or due to pre-existing disease exacerbated by pregnancy-associated weight gain and hormonal changes.3,4
Diagnostic criteria for idiopathic intracranial hypertension (adapted from Friedman et al. 1 ).
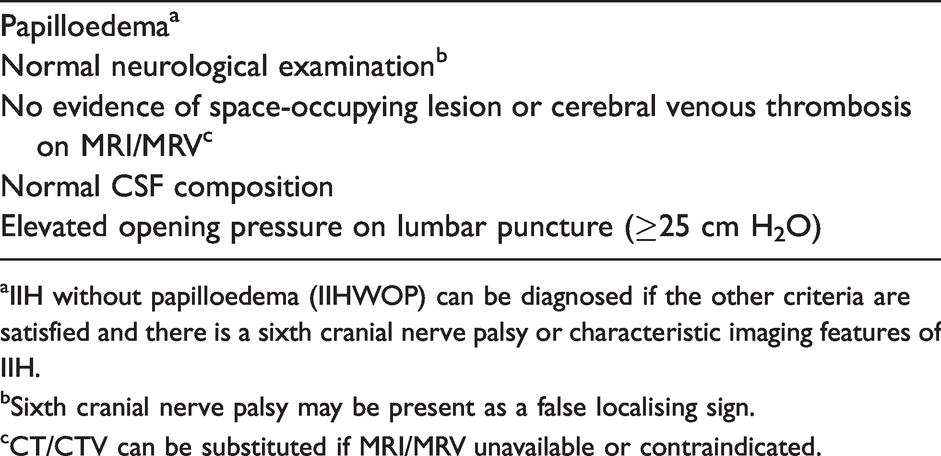
aIIH without papilloedema (IIHWOP) can be diagnosed if the other criteria are satisfied and there is a sixth cranial nerve palsy or characteristic imaging features of IIH.
bSixth cranial nerve palsy may be present as a false localising sign.
cCT/CTV can be substituted if MRI/MRV unavailable or contraindicated.
Vision loss in IIH and other causes of papilloedema is believed to result from axoplasmic stasis at the optic nerve head, often with an enlarged blind spot due to elevation of peripapillary retina. Papilloedema and visual loss can be asymmetrical or even unilateral. 5 This may be due to anatomical variation in the optic nerve sheath and lamina cribrosa, or a subarachnoid meshwork in the optic canal that modulates of intracranial pressure (ICP) to the optic nerve transmission of intracranial pressure (ICP). 6 Central vision is occasionally affected early in the disease course due to macular oedema, exudate, haemorrhage or chorioretinal folds. 7 IIH can result in permanent visual loss, and while rates of visual impairment are thought to be similar between pregnant and nonpregnant individuals, occasional fulminant cases require surgical intervention during pregnancy. 4 This raises complex management dilemmas when preservation of maternal vision must be balanced with the theoretical risks of medical and surgical treatment and the possibility of premature delivery with associated fetal implications.
Case
A 33-year-old woman presented to the ophthalmology clinic at 20 weeks’ gestation with a six-month history of blurred vision and headache. IIH had been diagnosed 12 years prior but resolved following significant weight loss. Her medical history included polycystic ovarian syndrome, anaemia and gastric bypass surgery. On examination, the woman’s weight was 128 kg with a body mass index (BMI) of 47 kg/m2, best corrected visual acuity was 6/6 (right) and 6/15 (left), and fundoscopy showed Frisén grade IV papilloedema bilaterally. Computerised perimetry showed bilateral visual field loss with mean deviations of −12.72 dB on the left and −3.98 dB on the right. Lumbar puncture under fluoroscopic guidance revealed an opening pressure of 29 cm H2O, with normal protein, glucose and cell count, and MRI/MRV without contrast demonstrated a narrowed left transverse sinus with no other abnormalities.
Acetazolamide 250 mg twice daily was commenced at 22 weeks’ gestation but was not tolerated due to nausea and worsening headache. Computerised perimetry showed significant field loss worse on the left than the right (Figure 1(a)). Operative intervention was considered, but further temporising measures were pursued given a short cervical length of 22 mm and concerns that surgery and anaesthesia might induce preterm labour. By 25 weeks’ gestation, there had been 4 kg of gestational weight gain. Therapeutic lumbar punctures were performed at 25 and 26 weeks’ gestation draining 27 mL of CSF. Both were performed in the seated position due to difficulty locating anatomical landmarks, precluding accurate measurement of opening pressure. There was temporary improvement in headache which returned approximately 12 h following each.
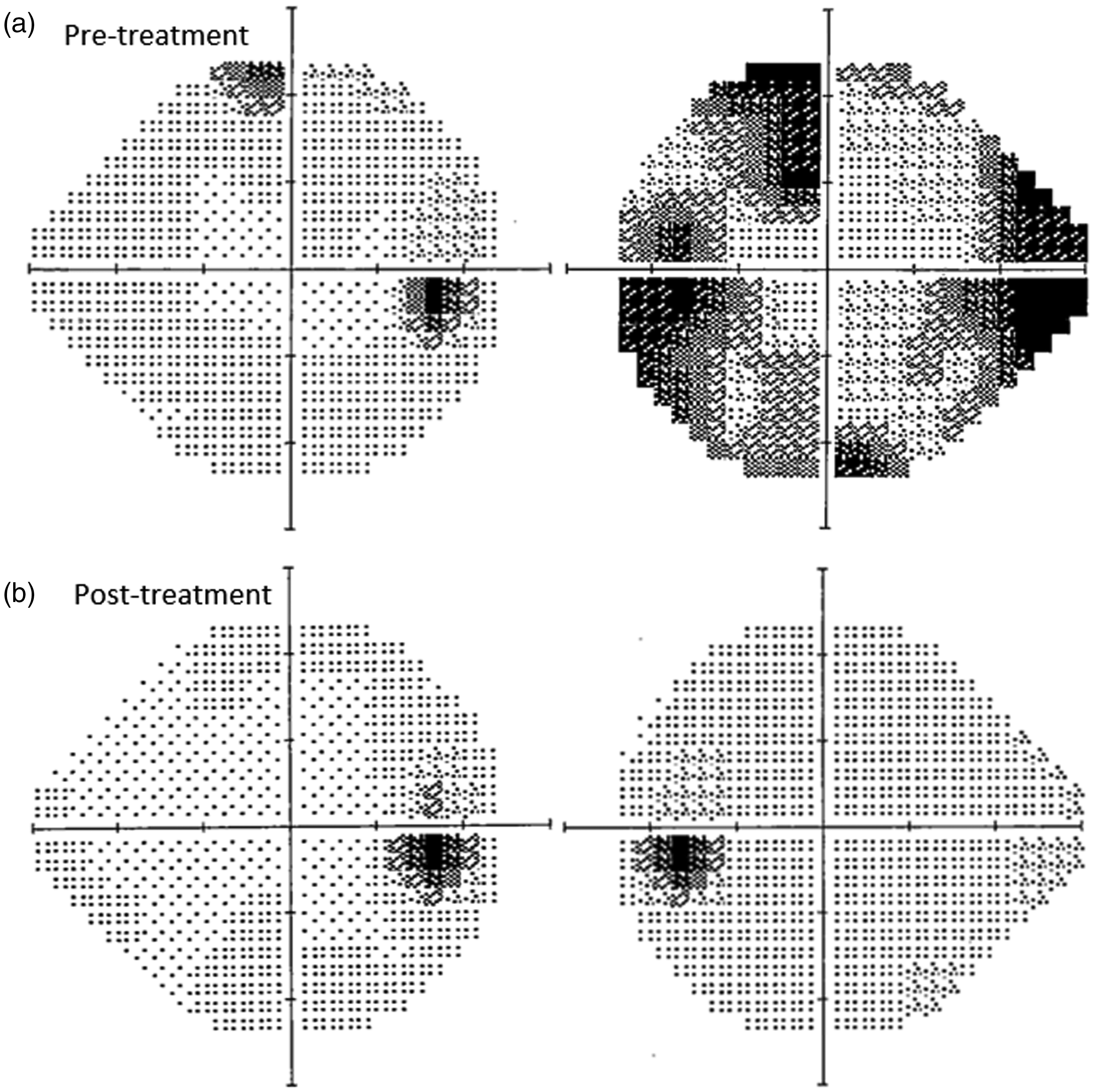
(a) Visual field analysis at 22 weeks’ gestation, prior to operative treatment (SITA Faster central 24–2) – MD −3.37 dB (right) and −14.94 dB (left). (b) Visual field analysis at 25 weeks’ gestation, two days after ventriculoperitoneal shunting – MD −1.26 (right) and −4.36 dB (left). MD: mean deviation.
A ventriculoperitoneal shunt was inserted at 26 weeks’ gestation due to headache unresponsive to medical therapy and progressive visual field loss on perimetry. A right parietal ventricular catheter was connected to fixed pressure valve with opening pressure 7–8.5 cmH2O (Delta 1.5, Medtronic, USA) and tunnelled to the abdomen. Pneumoperitoneum was obtained by open cut down in the right upper quadrant and the peritoneal catheter was inserted under laparoscopic vision. Surgical intervention led to improvement of the woman’s headache and marked improvement in subjective vision. Formal perimetry two days following the procedure confirmed improvement in visual fields (Figure 1(b)). However, approximately two weeks postoperatively, headache and visual loss returned necessitating a shunt revision at 31 weeks’ gestation. A non-functional abdominal catheter was identified but correction of this failed to improve the woman’s symptoms. An induction of labour was performed at 34 weeks’ gestation for intractable headache which was followed by an uncomplicated vaginal delivery. At one week postpartum, headache had completely resolved.
Approach to management
The management of IIH in pregnancy requires a multidisciplinary involving obstetric physicians, obstetricians, neuro-ophthalmologists, neurosurgeons and obstetric anaesthetists (Table 2). Ophthalmic examination including dilated fundoscopy and computerised perimetry is essential to document the severity of papilloedema and the extent of visual field loss (Figure 2). Acute severe hypertension can cause headache and papilloedema and should be excluded. Confirmation of the diagnosis requires urgent magnetic resonance imaging of the brain and venography without contrast (MRI/MRV) to exclude a space-occupying lesion or cerebral venous thrombosis. Lumbar puncture is required to demonstrate elevated opening pressure with normal CSF constituents, although the procedure is often challenging due to difficulties locating anatomical landmarks and may require radiological guidance. 8 Computed tomography of the brain with venography using iodinated contrast (CT/CTV) has negligible fetal radiation exposure and is acceptable if MRI is unavailable or contraindicated. The use of gadolinium contrast for MRI is usually advised against in pregnancy due to concerns regarding accumulation in amniotic fluid and the potential for fetal neurotoxicity. 9 IIH can be diagnosed in the absence of papilloedema if there are characteristic findings on imaging including an empty sella and flattening of the posterior aspect of the globe. 1
Treatment of idiopathic intracranial hypertension in pregnancy.*
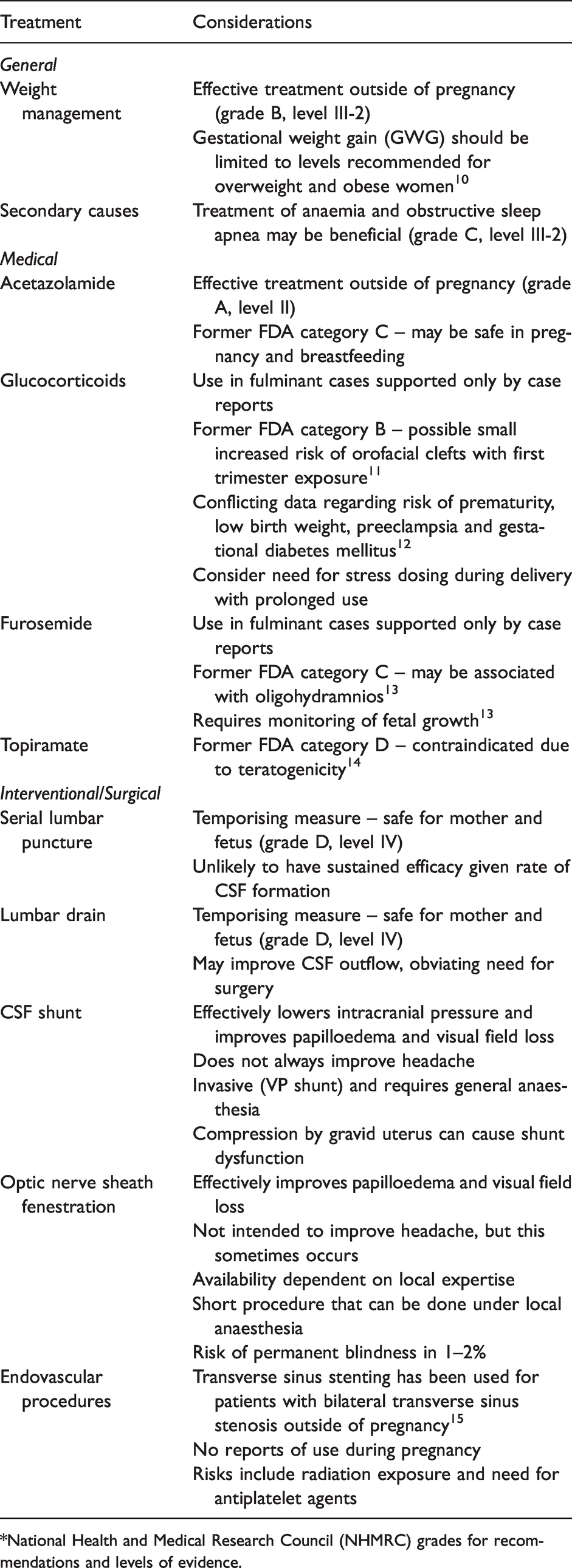
*National Health and Medical Research Council (NHMRC) grades for recommendations and levels of evidence.
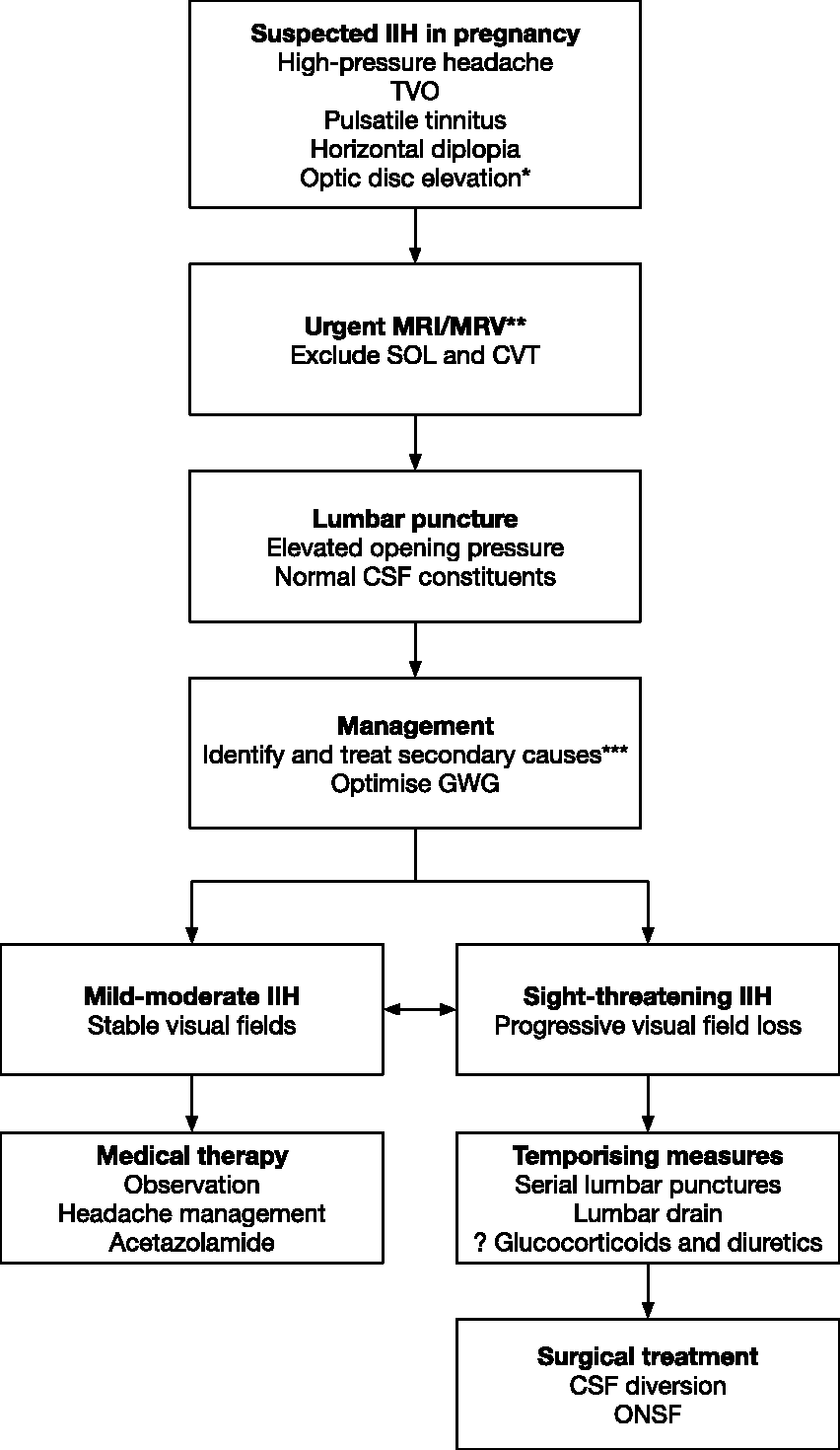
Management of idiopathic intracranial hypertension in pregnancy, adapted from Mollan et al. 8 *IIH can be diagnosed in the absence of papilloedema if characteristic imaging features are present. **CT/CTV can be substituted if MRI unavailable or contraindicated. ***Secondary causes to consider include iron deficiency anaemia and obstructive sleep apnoea. CSF: cerebrospinal fluid; CT/CTV: computed tomography with venography; CVT: cerebral venous thrombosis; GWG: gestational weight gain; IIH: idiopathic intracranial hypertension; MRI/MRV: magnetic resonance imaging with magnetic resonance venography; ONSF: optic nerve sheath fenestration; SOL: space-occupying lesion; TVO: transient visual obscurations.
Secondary causes
Secondary causes of raised intracranial pressure, including sleep-disordered breathing and anaemia, are prevalent in pregnancy. Obstructive sleep apnoea (OSA) raises intracranial pressure and may cause or exacerbate IIH. 16 A causal link between OSA and IIH has not been definitively established, and papilloedema is uncommon among nonpregnant individuals with OSA, but cases of IIH that resolve with continuous positive airway pressure (CPAP) treatment have been reported. 17 Obese pregnant women are likely to be at increased risk for pre-existing or gestational OSA, and treatment may be beneficial given the association with adverse pregnancy outcomes, including hypertensive disorders of pregnancy and perinatal mortality. 18 Similarly, anaemia has been associated with IIH in nonpregnant individuals with improvement in symptoms after correction of anaemia, although evidence is conflicting.19,20 Whether iron deficiency without anaemia contributes to IIH is not clear, but iron deficiency anaemia is a frequent and readily treatable finding in pregnancy and should be addressed in women with IIH.
Management of headache
While avoiding permanent visual loss is the principal clinical concern in IIH, headache is often the more problematic symptom to women and requires specific management. Classically, the headache of IIH is associated with elevated intracranial pressure and resolves with pressure lowering, although this sometimes does not occur and some women with other causes of headache also experience improvement after lumbar puncture. 21 Indeed, headache severity does not correlate with opening pressure in women with mild IIH, and many women continue to have headache after intracranial pressure normalises. 22 Up to two-thirds of women with IIH have a headache phenotype overlapping with migraine, and one-quarter with tension-type headache. Hence, particularly in known migraineurs, abortive and preventive therapies for migraine should be considered alongside appropriate management of intracranial pressure, and medication overuse should be identified and addressed. 23
Weight loss
Obesity is the principal risk factor for IIH, with a clear dose-dependent relationship between body mass index (BMI) and vision loss. 24 Hence, weight loss remains the only true disease-modifying therapy for IIH. 25 Sinclair et al. showed that weight loss induced by a low-energy diet reduced intracranial pressure, papilloedema and symptoms of intracranial hypertension and stabilised visual field loss among overweight nonpregnant women. 26 Bariatric surgery may be more effective than lifestyle modification and medical therapy for obesity in improving headache and papilloedema, although this is mainly driven by a greater decrease in BMI. 27 However, the association between weight and opening pressure on lumbar puncture is weak, suggesting that an alternative mechanism may be at play. 28 Obesity is linked with increased activity of 11β-hydroxysteroid dehydrogenase 1 in adipose tissue which converts inactive cortisone to active cortisol, and this may affect intracranial pressure given the role of glucocorticoid receptor activity in the regulation of choroid plexus fluid secretion. 29 Increased cortisol production during pregnancy may be responsible for some cases of de novo or worsening IIH in pregnancy.
Recommendations for gestational weight gain (GWG) depend on pre-pregnancy body mass index, ranging from 6.8–11.4 kg in overweight women to 5–9.1 kg in the obese, and specific recommendations for women with IIH are not available.30,31 Women with IIH and elevated BMI should be referred to a dietician in pregnancy to ensure GWG is appropriate. 24 In this case, symptoms progressed during pregnancy despite GWG not being excessive. Weight loss is not advised for pregnant women with IIH considering the potential for adverse fetal outcome, specifically low birth weight and premature delivery. 32
Medical treatment
Acetazolamide
Acetazolamide is a carbonic anhydrase inhibitor that reduces CSF production by altering ion fluxes across the ependymal cells of the choroid plexus. 25 The IIH Treatment Trial (IIHTT) randomised nonpregnant adults with newly diagnosed IIH to dietary intervention plus either acetazolamide or placebo, starting at a dose of 250 mg twice daily and increasing to a total daily dose of 4 g. 33 The primary outcome was perimetric mean deviation, a measure of visual field loss, with significantly greater improvement in the acetazolamide group at six months compared with placebo. 34 Persistent headaches were common in both treatment groups and were not significantly improved at six months with acetazolamide compared with placebo. 35 Common adverse effects include paraesthesia, nausea and vomiting, and altered taste sensation, although the maximum dose was tolerated in 44% of women. 36
The use of acetazolamide during pregnancy has been controversial, particularly in the first trimester, as reflected in recent international consensus guidelines. 8 Acetazolamide was classified as FDA category C due to evidence of teratogenicity in animal studies, albeit at doses as high as 1000 mg/kg which are significantly greater than routinely used in humans. 37 Successful use of acetazolamide in pregnancy, including in the first trimester, has been reported without adverse effects.38,39 There have been isolated reports of limb malformations after in utero exposure, but the Collaborative Perinatal Project did not detect an increased rate of congenital anomalies in the offspring of over 1000 pregnant women treated with acetazolamide. 40 Neonatal metabolic acidosis can occur following exposure in the third trimester. 41 Acetazolamide is considered safe at doses up to 1 g daily in breastfeeding mothers: the drug transfers to breastmilk in small quantities with neonatal exposure being less than 1% of the maternal dose per kilogram.42,43
Other agents
There is no evidence to support a role for other diuretics, such as furosemide, and glucocorticoids in the management of IIH. 8 Intravenous methylprednisolone, acetazolamide and furosemide have been used empirically in fulminant cases of IIH outside of pregnancy. 44 Topiramate may be an effective treatment for IIH outside of pregnancy, both through appetite suppression and weak carbonic anhydrase inhibition, but is teratogenic.45,46
Interventional and surgical treatment
Serial lumbar puncture and lumbar drains
Serial lumbar puncture has been used as a temporising measure in pregnant women with IIH as a bridge to definitive surgical therapy or delivery. 47 Although uncomfortable and inconvenient for the woman, it could delay the perceived maternal and fetal risks associated with major neurosurgical intervention in women with severe or rapidly progressive visual loss. The physiological basis for this treatment has been questioned given that the total CSF volume of 90–150 mL is replaced 3–5 times per day, presumably requiring multiple large-volume lumbar punctures per day to lead to a sustained reduction in intracranial pressure. 48 However, there is evidence that transverse sinus stenosis in IIH is a secondary phenomenon that results from elevated intracranial pressure and contributes to its persistence. 49 Hence, temporary reduction of intracranial pressure by lumbar puncture, aided by ongoing leakage of CSF following the procedure, may relieve the stenosis and interrupt this feedback loop leading to sustained clinical improvement in some cases. Indeed, both large-volume lumbar puncture and CSF diversion procedures have been shown to result in improvement of transverse sinus stenosis on serial MRV imaging.49,50 Lumbar puncture may lead to an improvement in headache in some women but can worsen headache in up to two-thirds of women with IIH. 51
Lumbar drain insertion is an alternative procedure that allows continuous drainage of CSF over a period of several days at a rate greater than its rate of formation. Consensus guidelines suggest the use of lumbar drains in fulminant IIH when surgery is likely to be delayed by more than 24 h. 8 However, there have been reports of disease resolution following lumbar drainage without further surgery, suggesting that sustained reduction in intracranial pressure may relieve compression of the transverse sinuses and alter the natural history of the condition.44,52 Further studies are needed to determine whether this strategy can obviate the need for surgical intervention in pregnant women with fulminant IIH.
CSF shunting
Diversion of CSF effectively reduces intracranial pressure and can be achieved by lumboperitoneal (LP), ventriculoperitoneal (VP), ventriculoatrial or ventriculojugular shunts. LP and VP shunts are similarly effective, with slightly higher failure rates for VP shunts and revision rates for LP shunts. 53 VP shunts may have better long-term patency rates, but LP shunts have the benefit of being less invasive as the cranium is not entered, although they do carry a risk of acquired Chiari malformation.53,54 Effective CSF diversion by either means improves papilloedema and visual acuity and can reverse progressive visual decline, although headache commonly persists postoperatively. 55 Both LP and VP shunts have been successfully inserted in pregnancy in women with progressive visual loss. 56 Shunt malfunction can occur during pregnancy, including due to increased intra-abdominal pressure interfering with valve function, but can often be managed conservatively. 57
Optic nerve sheath fenestration
Optic nerve sheath fenestration (ONSF) refers to the surgical creation of a slit or window in the optic nerve sheath to treat papilloedema and visual field loss. This can be performed by medial, lateral, combined or endoscopic approaches and likely acts by creating a new pathway for CSF egress from the optic nerve sheath. Papilloedema improves in the majority of women but up to 70% eventually deteriorate and require further procedures. 58 There is a 1–2% risk of blindness that results from optic neuropathy secondary to vascular compromise or retrobulbar haemorrhage. 59
ONSF has been performed for fulminant IIH during pregnancy, and is sometimes considered with severe papilloedema and worsening visual loss but minimal headache. 60 The choice between ONSF and CSF shunting often depends on the local expertise and experience with either procedure. 61 Women with very high opening pressures (greater than 50 cm H2O) may be at increased risk of ONSF failure and might benefit from CSF shunting as the primary procedure. 62 Potential benefits of ONSF in pregnancy include the ability to perform the procedure under local anaesthesia, shorter operation duration and avoidance of entry into the peritoneal cavity. This is of interest when surgery must be performed after the limit of viability, although the association between general anaesthesia for non-obstetric surgery and preterm delivery is controversial and the risk of preterm labor after laparoscopy or laparotomy is low.63–65
Other procedures
Endovascular placement of a stent to correct transverse sinus stenosis is increasingly advocated as an effective treatment for IIH, but the radiation doses and antiplatelet agents required likely preclude this as a treatment during pregnancy. 15 This could be considered when symptoms persist after pregnancy. Historically, subtemporal decompression has been performed for IIH leading to good visual outcomes, albeit often requiring CSF diversion to address persistent headache. This procedure has not been reported in pregnancy. 66
Natural history and prognosis
Limited data from case series and case-control studies suggest that IIH most frequently arises in the first trimester, with rates of visual loss similar to nonpregnant women.4,67 Recurrence of IIH during pregnancy is thought to be uncommon, occurring in approximately 5% of cases, and it is not certain whether pregnancy is a risk factor for recurrence of IIH independent of weight gain.68,69 Monitoring of women with IIH during pregnancy includes dilated fundal examination and computerised perimetry, the frequency of which depends on papilloedema severity and the degree of field loss. International consensus guidelines recommend that women with mild or moderate papilloedema and minimal field loss be seen every one to three months, while women with severe papilloedema and stable fields should be seen at least every four weeks, increasing to weekly when fields are unstable. 8
Preconception care
There is little evidence to guide preconception counselling for women with IIH. The determinants of disease recurrence or deterioration in pregnancy are not known with certainty, although disease activity prior to pregnancy may be a reasonable guide. Appropriate GWG is likely to be important for asymptomatic women with quiescent disease to avoid recurrence in pregnancy. Weight loss, including by lifestyle modification and bariatric surgery, can be pursued prior to pregnancy in women with mild-to-moderate IIH successfully controlled on medical therapy. This may allow the cessation of acetazolamide prior to conception. Sustained weight loss is associated with successful cessation of systemic treatment, with one study showing 8.9 kg of weight loss in those able to stop treatment compared with 6.6 kg in those remaining on therapy, although this can take 24 months or longer to achieve. 70 Among women with progressive or sight-threatening disease, conception is ideally delayed until surgical intervention is complete and remission achieved.
Labor and delivery
IIH is not a contraindication to vaginal delivery and epidural or spinal analgesia, nor is the presence of a CSF shunt.71,72 Combined spinal-epidural analgesia has been described, allowing for removal of CSF as needed for relief of headache. 73 Intrathecal catheters have also been used to permit CSF removal during delivery if symptomatic deterioration occurs. 74 Pain contributes to the rise in ICP that occurs during vaginal delivery, and effective neuraxial analgesia may mitigate this. 75
Conclusion
Management of IIH in pregnancy is complex, with mostly low-quality evidence available to guide the choice of intervention in cases that demonstrate progressive visual field loss. Surgery, either CSF shunting or ONSF, is effective and generally well tolerated and the choice of procedure may depend on local expertise and experience. Predictors of benefit from one procedure over the other are yet to be fully elucidated but may include high opening pressures favouring shunting and predominant visual loss without headache favouring ONSF. Emerging data on the potential for lumbar puncture or temporary lumbar drainage to alter the course of IIH raise the prospect of avoiding neurosurgery during pregnancy, although these procedures are often inconvenient and uncomfortable for the woman. There is a lack of robust epidemiological information on IIH in pregnancy, particularly regarding the determinants of recurrence and deterioration. Preconception counselling is essential to allow for weight loss to occur prior to pregnancy, changing the natural history of the disease.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Written informed consent was obtained from the patient for their anonymised information to be published in this article.
Guarantor
LAB is the guarantor of the present work.
Contributorship
LAB wrote the first draft of the article. All authors reviewed and substantially edited the manuscript, and approved the final version.