
Abstract
Background
Hemophagocytic lymphohistiocytosis is a rare disorder, especially in pregnancy, characterized by excessive immune activation leading to hemophagocytic activity.
Case Report
A 34-year-old woman presented at 31 weeks’ gestation with fever, cytopenias, hyperferritinemia and fulminant hepatitis. Bone marrow biopsy was non-contributory, and no trigger was identified. Liver biopsy confirmed the diagnosis of hemophagocytic lymphohistiocytosis, and she received dexamethasone and etoposide, which was changed to anakinra to allow breastfeeding. Prompt diagnosis and treatment of hemophagocytic lymphohistiocytosis is crucial to the survival of pregnant women, but no consensus exists regarding the most appropriate therapy during pregnancy.
Conclusion
Hemophagocytic lymphohistiocytosis is life-threatening and associated with significant morbidity and mortality. Important treatment considerations in pregnancy include maternal health, fetal prematurity and treatment toxicity. Anakinra has been successfully used in pregnancy and provides a promising alternative.
Background
Hemophagocytic lymphohistiocytosis (HLH) is a rare, life-threatening inflammatory disorder characterized by pathological immune system activation leading to phagocytosis of normal hematopoietic cells. 1 The hyperinflammatory response and massive cytokine release lead to the clinical manifestations of the syndrome including persistent fever, hepatosplenomegaly and end-organ damage. The differential diagnosis of the clinical and biochemical manifestations of HLH is broad and includes malignancies (leukemia, lymphoma), infections (bacterial, viral or parasitic) and autoimmune disorders (systemic lupus erythematosus, Still’s disease). 2
The disease is divided into primary or familial HLH (FHL) and secondary HLH. FHL patients have a genetic predisposition and multiple affected genes leading to a deficiency of immunomodulatory mechanism have been identified. 3 It is a fatal disease with a median survival of less than two months after diagnosis if untreated. Despite its name, family history is often negative as it is an autosoal recessive disease. 2 Although some sporadic mutations can be identified, secondary HLH usually refers to an acquired condition related to autoimmune syndromes, rheumatological diseases, immunodeficiencies and infections. 4 It is the most common cause of HLH in the adult population.
HLH in the peripartum period is an excessively rare entity and although a few cases are reported in the literature,5,6 there is no established consensus with regard to management of this entity during pregnancy. Here, we report a case of pregnancy-related HLH leading to fulminant hepatitis, as well as the successful use of Anakinra, an IL-1 inhibitor, as a central part of therapy. We highlight important features and clinical insight into the diagnosis and management of this potentially fatal disease during this cornerstone period in a woman’s life.
Case
A 34-year-old woman, in her second pregnancy, presented to a community hospital at 31 weeks’ gestation with epigastric pain. Observations on arrival revealed a blood pressure of 116/80 mm Hg, heart rate of 112 beats per minute, temperature of 38.3°C and oxygen saturation of 99% on air. Initial investigations revealed anemia, thrombocytopenia and hepatocellular liver injury (Table 1). She was transferred to our quaternary care center for suspicion of HELLP syndrome (hemolysis, elevated liver enzymes and low platelets) after receiving magnesium sulfate and betamethasone. The woman was originally from Algeria but living in Canada for over 10 years and was previously healthy with no medical history or pertinent family history. She was persistently febrile with epigastric abdominal discomfort. She denied recent travel or infectious contacts.
Laboratory investigations.
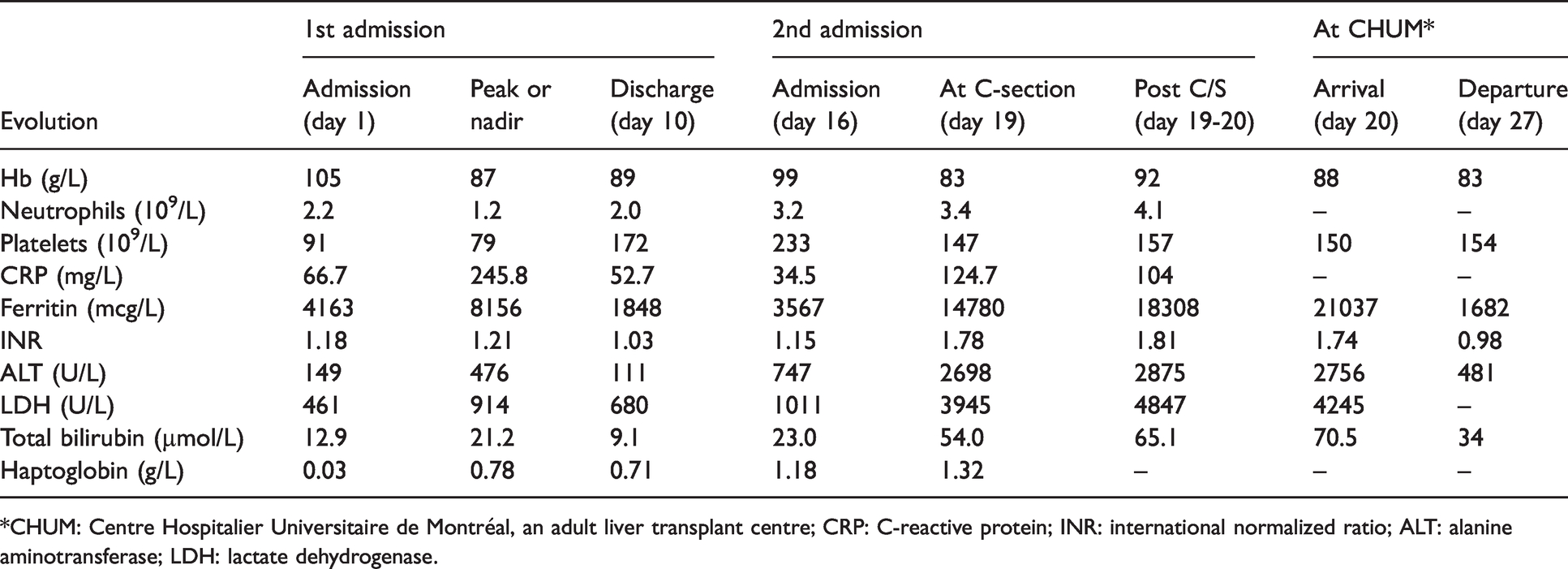
*CHUM: Centre Hospitalier Universitaire de Montréal, an adult liver transplant centre; CRP: C-reactive protein; INR: international normalized ratio; ALT: alanine aminotransferase; LDH: lactate dehydrogenase.
Investigations revealed worsening pancytopenia, elevated lactate dehydrogenase (LDH) with worsening liver injury (Table 1). Abdominal ultrasound revealed splenomegaly at 16.8 cm. The woman was started on cefotaxime for presumed sepsis, but an extensive infectious and auto-immune work-up was either negative or pending, including but not limited to blood cultures, serology and polymerase chain reaction (PCR) for all viral hepatitidies, autoimmune hepatitis, and some zoonoses as well as other causes of fever of unknown origin.
Over the next few days, she deteriorated both clinically and biochemically. She remained febrile with associated tachycardia, with worsening hepatocellular liver enzymes. Intravenous acyclovir was started empirically for the possibility of a herpetic hepatitis. The ferritin was found to be elevated and rising rapidly. A bone marrow biopsy was performed and was remarkable only for mild hypocellularity. Shortly after, the woman developed a diffuse maculopapular rash and further deteriorated hemodynamically and biochemically. She was started empirically on high dose methylprednisolone for a suspected inflammatory disorder. Eighteen days after first consultation for this illness, she underwent an urgent caesarean section at 33 weeks’ gestation for fetal distress and delivered a male infant with APGAR scores of 3,5 and 5 at 1, 5 and 10 minutes respectively and a birth weight of 2450 g. He was transferred to the neonatal intensive care unit and had a favorable clinical evolution.
Immediately following her delivery, the woman’s status progressed to fulminant liver failure with evidence of synthetic liver dysfunction and a ferritin above 18,000 ng/mL. She was transferred to the Centre Hospitalier Universitaire de Montréal (CHUM), an adult liver transplant center where a liver biopsy was performed and confirmed the diagnosis of HLH. She improved significantly with dexamethasone and etoposide and expressed the desire to breastfeed. Etoposide was thereafter changed to anakinra, an IL-1 inhibitor, to allow for breastfeeding. The woman continued to improve and was discharged home. Many weeks later, she was clinically well, with liver enzymes and ferritin that had normalized. Both mother and child are currently healthy, with no evidence of residual disease.
Discussion
Pregnancy-associated HLH is a rare entity, but it has been described increasingly in the literature. In the adult population, the main causes of secondary HLH include malignancies, especially hematological, as well as rheumatological disorders. The young pregnant population is different in that the most common causes of secondary HLH include infections7–11 and autoimmune disorders,12–15 especially systemic lupus erythematosus. It has been hypothesized that cases with unknown etiologies may be pregnancy-derived, with fetomaternal trafficking playing a role in the inflammatory response.16,17
We describe a case of HLH in pregnancy with a favorable clinical outcome in a woman without an identified trigger or underlying cause. Reported cases of women without an identifiable cause for HLH during pregnancy have had positive outcomes,16,18–20 which raises the possibility of a self-limited viral infection and inflammatory disorder which would respond to high doses of steroids. It has also been hypothesized that pregnancy causes an immune adaptation to the genetically foreign fetus which decreases cell-mediated immunity and leads to macrophage overactivation as the first immune response to infection. 21
Our patient developed fulminant liver failure and was evaluated for urgent liver transplantation. Giard et al. describe a case of HLH in pregnancy that progressed to liver failure in a woman diagnosed with Kikuchi-Fujimoto lymphadenitis who ultimately died despite corticosteroid therapy, etoposide and termination of pregnancy. 22 Liver failure with HLH has been evaluated in the non-pregnant population and the mechanism of HLH-mediated liver injury remains unknown. 23 While liver injury can result from underlying diseases, infiltration of activated histiocytes and cytokine production in HLH can lead to multiorgan failure, including severe liver injury. 23
While diagnostic criteria for HLH were established in 2004, 2 the diagnosis remains challenging in pregnancy as most of the cardinal clinical manifestations can mimic more common entities including sepsis and HELLP, and it can take time for some diagnostic criteria results to become available. The presence of hemophagocytosis is not required nor sufficient to establish the diagnosis of HLH. Our patient’s bone marrow biopsy did not reveal hemophagocytosis, but she met the HLH diagnostic criteria and was treated accordingly. The presence of persistent fever and cytopenias without a localizing infectious source should prompt clinicians, in the appropriate setting, to pursue the possibility of HLH and include ferritin, triglycerides and, when possible, soluble CD25 levels to their investigations.
While the prompt diagnosis and treatment of HLH is crucial to the survival of pregnant women, no consensus exists regarding the most appropriate therapy for HLH during pregnancy. Due to the high mortality rate of this disorder, timely recognition and treatment initiation is fundamental. The need for delivery relies on a balance between maternal instability and fetal prematurity, as well as treatment toxicity. Delivery as a specific treatment for HLH in pregnancy, especially if no other etiology is found, remains controversial. Patients with an identified underlying disorder should be treated according to their respective etiology, e.g. human immunodeficiency virus, 7 herpes simplex virus10,24 or tuberculosis. Most described cases in HLH in pregnancy were treated with corticosteroids.3,5,6,25 Etoposide is an antimitotic chemotherapeutic agent used in the treatment of multiple malignancies. Its use is limited in pregnancy due to the possible fetal toxicity and severe myelosuppression.
Yip et al. 20 previously described the use of Anakinra, an IL-1 receptor antagonist, as an alternative to etoposide. anakinra is used in rheumatoid arthritis and has been used in children with secondary HLH. 26 Although safety data in pregnancy are limited, it has been used to treat other conditions without serious complications to the mother or the fetus.27,28 An international multicenter study of mothers exposed to interleukin-1 receptor antagonists, identified 14 babies who were breastfed by mothers receiving anakinra without evidence of infections or developmental abnormalities. 29 Our patient was able to breastfeed while continuing anakinra as well as a steroid taper and showed no evidence of relapsing disease.
Conclusion
HLH is a life-threatening condition associated with significant morbidity and mortality. Timely recognition and management are essential, and identification of a possible underlying trigger can help clarify the treatment plan. Important treatment considerations in pregnancy include maternal health, fetal prematurity and treatment toxicity. Although safety data are lacking, anakinra has been successfully used in pregnancy to treat various conditions and provides a promising alternative to the current mainstay of therapy.
Footnotes
Authors’ note
Camille Simard (CS) is first author for this manuscript. Marie-Lou Tardif (MLT) is last and supervising author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought for this review article because it consists of a review of the literature.
Informed consent
A signed paper consent has been obtained from the woman described in the case report.
Guarantor
CS.
Contributorship
CS and MLT participated in the review of the existing literature. CS wrote the first draft of the manuscript. Both authors reviewed and edited the manuscript and approved the final version of the manuscript.
Acknowledgements
None.