
Abstract
Background
The first-line treatment for gestational diabetes mellitus remains insulin, but oral hypoglycemic agents are easier and cheaper to use. The aim of the current study was to compare the efficacy and safety of oral glibenclamide and subcutaneous insulin on the serum glucose control and perinatal outcome of patients with gestational diabetes mellitus.
Materials and methods
This randomized clinical trial was conducted during a 2-year period from 2017 to 2019 in two tertiary healthcare centers in Shiraz, Iran. We included 84 singleton pregnancies between 24 and 34 weeks of gestation diagnosed with gestational diabetes mellitus. Patients were randomly assigned to oral glibenclamide (n = 44) or subcutaneous insulin (n = 40) according to a standard protocol and followed until delivery. The primary endpoint was to compare the glycemic level of patients, and the secondary outcomes included pregnancy adverse events and neonatal complications such as preeclampsia, preterm and premature rupture of membranes, preterm labor, placental abruption, maternal hypoglycemia, birth weight, neonatal hypoglycemia, hyperbilirubinemia, respiratory distress syndrome, and neonatal intensive care unit admission.
Results
The two study groups had comparable baseline characteristics. After treatment, the two study groups were comparable regarding fasting blood glucose (p = 0.398) and 2 h postprandial glucose (p = 0.085). There was no significant difference between the two groups regarding the rate of preeclampsia (p = 0.250), preterm rupture of membranes (p = 0.998), preterm labor (p = 0.495), hypoglycemia (p = 0.476), and abruption (p = 0.815). There was no significant difference between the two study groups in birth weight (p = 0.863) and the Apgar score at 1 (p = 0.190) and 5 min (p = 0.055). The rates of neonatal adverse events including hypoglycemia (p = 0.999), hyperbilirubinemia (p = 0.160), neonatal intensive care unit admission (p = 0.852), and respiratory distress syndrome (p = 0.665) were comparable between the two groups.
Conclusion
The results of the current study demonstrate that oral glibenclamide is as effective and safe as subcutaneous insulin in glycemic control and maternal and neonatal outcomes in women with gestational diabetes mellitus. Thus, it could be used as first-line treatment of gestational diabetes mellitus.
Introduction
Gestational diabetes mellitus (GDM) is a common complication of pregnancy that is associated with adverse pregnancy outcomes.1,2 The rate of the GDM is increasing worldwide and several lines of evidence have demonstrated that improving glycemic control during pregnancy is associated with improved neonatal outcomes as well as decreased maternal mortality and morbidity.3–5 Uncontrolled blood glucose during pregnancy has been associated with increased rates of macrosomia, neonatal death, and delivery complications, and increased risk of diabetes mellitus in the neonate. 6 Thus, blood glucose control is recommended during pregnancy, especially during the third trimester.7,8
Insulin remains the first line of treatment in patients with GDM in many countries according to the American College of Obstetricians and Gynecologists and has been approved by the Food and Drug Administration (FDA). 9 However, insulin administration is associated with several disadvantages including high price, route of administration (several subcutaneous injections), and risk of hypoglycemic events due to inappropriate dosing. Thus, oral hypoglycemic agents come into consideration including metformin and glibenclamide. 10 Research during the past decade has been performed on the subject with inconclusive results.11,12 Glibenclamide (glyburide) has been demonstrated to be more effective than metformin, while the adverse events are comparable. 12 However, there is controversy regarding the efficacy of glibenclamide compared to insulin injection despite several randomized clinical trials (RCTs) and meta-analyses.13–18 While some recent studies have demonstrated equal results of glucose control with glibenclamide and insulin,13,17 some others believe that insulin remains the treatment of choice.11,16,18 In addition, most of the previously conducted studies have focused on the serum glucose level control, and few of them have addressed adverse events and neonatal outcomes. The results of a recent RCT 17 demonstrated that the use of glibenclamide compared with subcutaneous insulin did not result in a greater frequency of perinatal complications. However, the results were inconclusive and there is a need for complementary fRCTs. Therefore, we designed this randomized, controlled clinical trial to compare the pregnancy outcome of patients with GDM who were being treated with oral glibenclamide and subcutaneous insulin.
Materials and methods
Study population
This randomized controlled clinical trial was conducted during a 2-year period from January 2017 to January 2019 in two tertiary maternal and fetal healthcare centers affiliated with Shiraz University of Medical Sciences. We included women aged 20 to 45 years, pregnant with a singleton pregnancy, with a gestational age of 24 to 34 weeks who were diagnosed with GDM. The GDM was confirmed according to the results of the 75-g glucose tolerance test (GTT). Briefly, the diagnosis was confirmed if a 75-g GTT resulted in one or more abnormal blood glucose values for fasting, 1-h postprandial, or 2-h postprandial blood glucose concentrations: greater than 92 mg/dL (5.1 mmol/L), greater than 180 mg/dL (10 mmol/L), or greater than 153 mg/dL (8.5 mmol/L), respectively. 19 We excluded the patients with renal diseases, liver diseases, overt DM (FBS ≥ 126 mg/dL), preeclampsia, chronic hypertension, and multiple pregnancies. We also excluded those who were screened for GDM before 24 weeks of gestation. All the included patients were given an individual nutritional education and exercise program and were asked to follow the instructions rigorously for 2 weeks. Only those who did not reach the glycemic control during this period were found eligible to be randomized. The study protocol was approved by the institutional review board (IRB) and medical ethics committee of Shiraz University of Medical Sciences (Reference No. CT-P-92-6115). The study was also registered by the Iranian registry for clinical trials (www.irct.ir; IRCT2016041317827N1).
Randomization and intervention
All the included patients received a registration number based on the order of registration in the study. All the eligible patients were randomly assigned to two study arms using a computer-based random digit analyzer. Only statisticians had access to the full list of the patients and groups. However, blinding could not be performed for patients and clinicians due to different routes of administration. Those assigned to the glibenclamide (glibenclamide 5 mg tablets, Kimia Daru Gharb Co., Tehran, Iran) group received the drug according to the following protocol. The drug was started with the lowest required dose, 2.5 mg daily, and was increased by 1.25–2.5 mg weekly, and finally reached 15 mg/day. If the blood glucose was not controlled by the dose of 15 mg/day of glibenclamide, they were started on insulin and excluded from the study. Blood glucose monitoring was done by patients themselves at home or in hospital, 4 times per day (overnight, fasting, and 2 h postprandial diet). Those who were assigned to the insulin group received it in rapid (regular insulin 100 IU, Exir Pharmaceutical Company, Tehran, Iran) and basal (NPH insulin 100 IU, Exir Pharmaceutical Company, Tehran, Iran) forms. The starting dosage for rapid analogs was 4 IU given subcutaneously before meals, 1 to 3 times per day as necessary, and increased by 2 IU every 2 days according to the postprandial blood glucose value. If necessary, the starting dosage for basal insulin was 4 IU to 8 IU given subcutaneously at bedtime and increased by 2 IU every 2 days according to the morning fasting blood glucose value. Women were taught to self-adjust their insulin doses in an effort to reach and maintain glycemic goals throughout their pregnancy.
Study protocol
All patients with the diagnosis of GDM were referred to a diet and nutrition clinic. Daily calorie quota was measured based on body mass index (BMI). These patients were instructed to have three meals and three snacks per day. Their diet was designed to provide 25 kcal/kg for obese patients and 35 kcal/kg for the non-obese ones, with 40–45% of total calories from carbohydrates. Patients were taught how to measure blood glucose with a glucometer. The aim was to maintain FBS ≤ 95 mg/dL and 2-h postprandial ≤ 120 mg/dL, according to the American Diabetes Association (ADA) guidelines. The FBS and 2-h postprandial blood glucose were measured once a week by obstetricians and twice weekly by the patients at home using a glucometer. The normal values were given to the patients and if there was an abnormal value or the patients had symptoms of hyperglycemia, they were asked to call the obstetrician. The glucometer values correlated with plasma blood glucose.
Outcome measures
At the initial visit, a detailed history was obtained that included demographic data, ethnic background, and a summary of past social medical, and obstetrical history. All mothers with GDM were scheduled for routine prenatal care visits. Laboratory and radiologic assessments were done according to the routine standard protocols. The primary outcome was the achievement of the goals of treatment or the best result in controlling the blood glucose. Other outcome measures included glycemic control during pregnancy, maternal weight gain, route of delivery, pregnancy, and neonatal complications including preeclampsia, dystocia, preterm and premature rupture of membranes (PPROM), placenta abruption, birth weight, prenatal mortality, neonatal hypoglycemia (neonatal blood glucose level ≤40 mg/dL); hyperbilirubinemia (total bilirubin ≥ 12 mg/dL in first 7 days of life); polycythemia (hematocrit ≥ 60%); hypocalcemia (ionized calcium < 8 mg/dL in first 3 days of life); pH of an umbilical artery; and 5-min Apgar Score. We have also recorded Neonatal Intensive Care Unit (NICU) admission, need for oxygen therapy for more than 1 h after birth, or need to assisted ventilation and intubation. Neonatal respiratory outcomes included the presence or absence of hyaline membrane disease and transient tachypnea (defined as respiratory distress in infants born near term that lasted for about three days). To evaluate the neonate hypoglycemia, the blood sugar was measured every 6 h for 2 days from birth.
Statistical analysis
According to the rate of pregnancy adverse events in women with GDM based on previously published data, 7 with 80% power to detect at least 5% difference between the two study groups regarding the primary endpoint and pregnancy adverse events with an α equal to 0.01, at least 39 patients were required in each study group. In order to compensate for non-evaluable patients, we included 44 patients in each study group. All the data are presented as mean ± SD and proportions as appropriate. Data were checked for normality using the Kolmogorov-Smirnov test. The proportions were compared between the two study groups using the chi-square test. Parametric variables with normal distribution were compared using an independent t-test, while those without normal distribution were compared using Mann-Whitney U-test. For comparing the parametric variables within the groups, paired t-test and repeated measures were used. A 2-sided p-value less than 0.05 was considered statistically significant.
Results
Overall, 96 singleton pregnancies were assessed for eligibility. Ten patients were excluded, and 86 patients were randomly assigned to two study groups (46 in the glibenclamide group and 40 in the insulin group). In the glibenclamide group, two patients had uncontrolled serum glucose which required insulin therapy. Thus, the final number of patients included in the final analysis was 84 patients (Figure 1). The baseline characteristics of the 84 patients are summarized in Table 1. As demonstrated, the baseline characteristics were comparable between the two study groups.
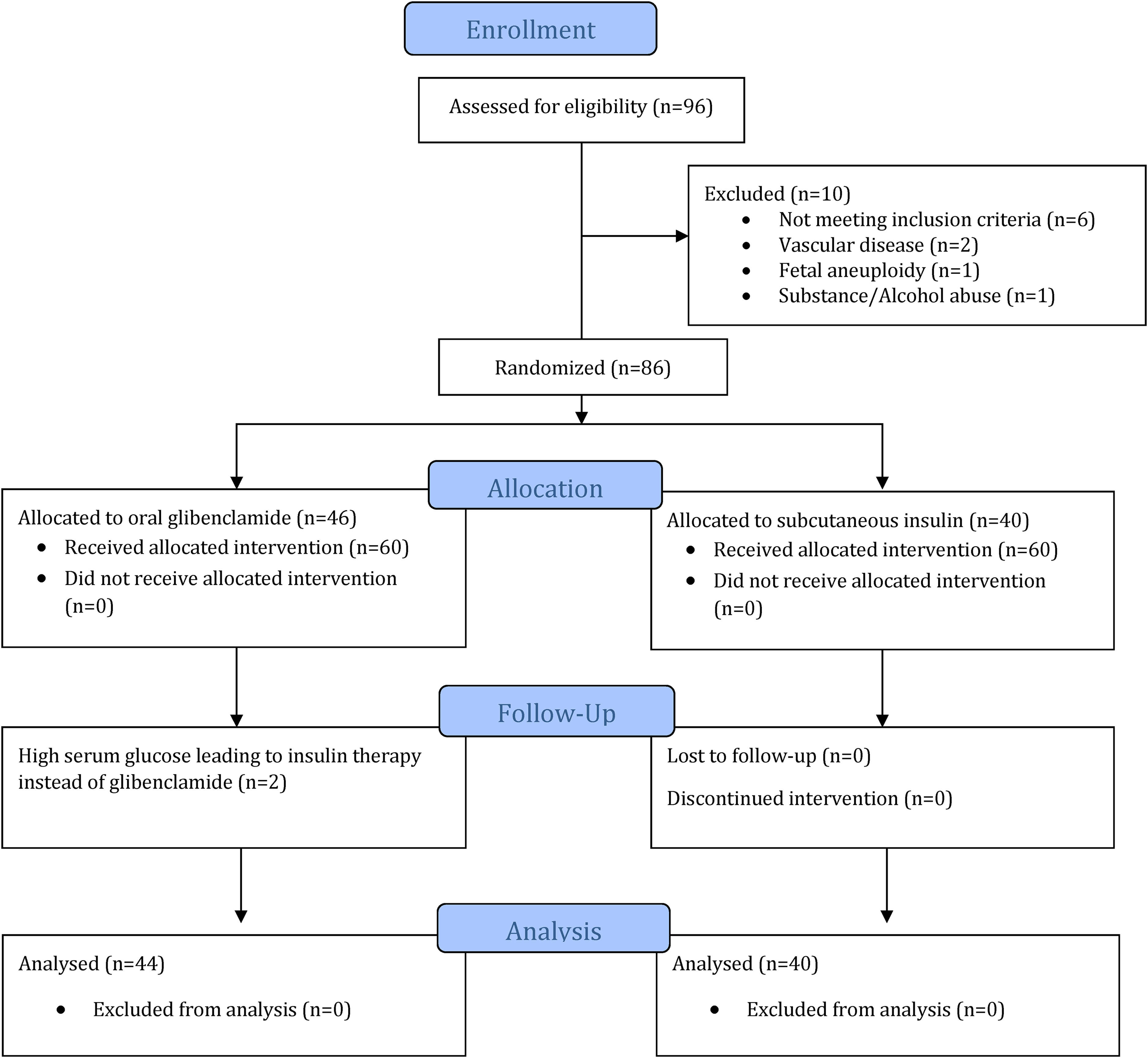
CONSORT flow diagram of the study.
Baseline characteristics of 84 singleton pregnancies with gestational diabetes mellitus in the two study groups.

BMI: body mass index; DM: diabetes mellitus; FBS: fasting blood glucose; GA: gestational age; GCT: glucose challenge test; GDM: gestational diabetes mellitus; GTT: glucose tolerance test.
After treatment with either glibenclamide or insulin, the FBS was comparable between the two study groups (p = 0.398). In the same way, the 2 h postprandial (2hpp) test results were comparable between the two study groups after the treatment (p = 0.085). Most of the patients underwent cesarean section in both study groups, and the most common reason for cesarean delivery was a previous caesarean delivery. However, both study groups were comparable regarding the route of delivery (p = 0.261). The maternal complications of pregnancy were also evaluated in both study groups. There was no significant difference between the two study groups regarding the rate of preeclampsia (p = 0.250), PROM (p = 0.998), preterm labor (p = 0.495), hypoglycemia (p = 0.476), and abruption (p = 0.815). The results of the maternal outcome of the two study groups are summarized in Table 2.
Maternal serum glucose level and the pregnancy outcome of 84 singleton pregnancies with gestational diabetes mellitus in the two study groups.
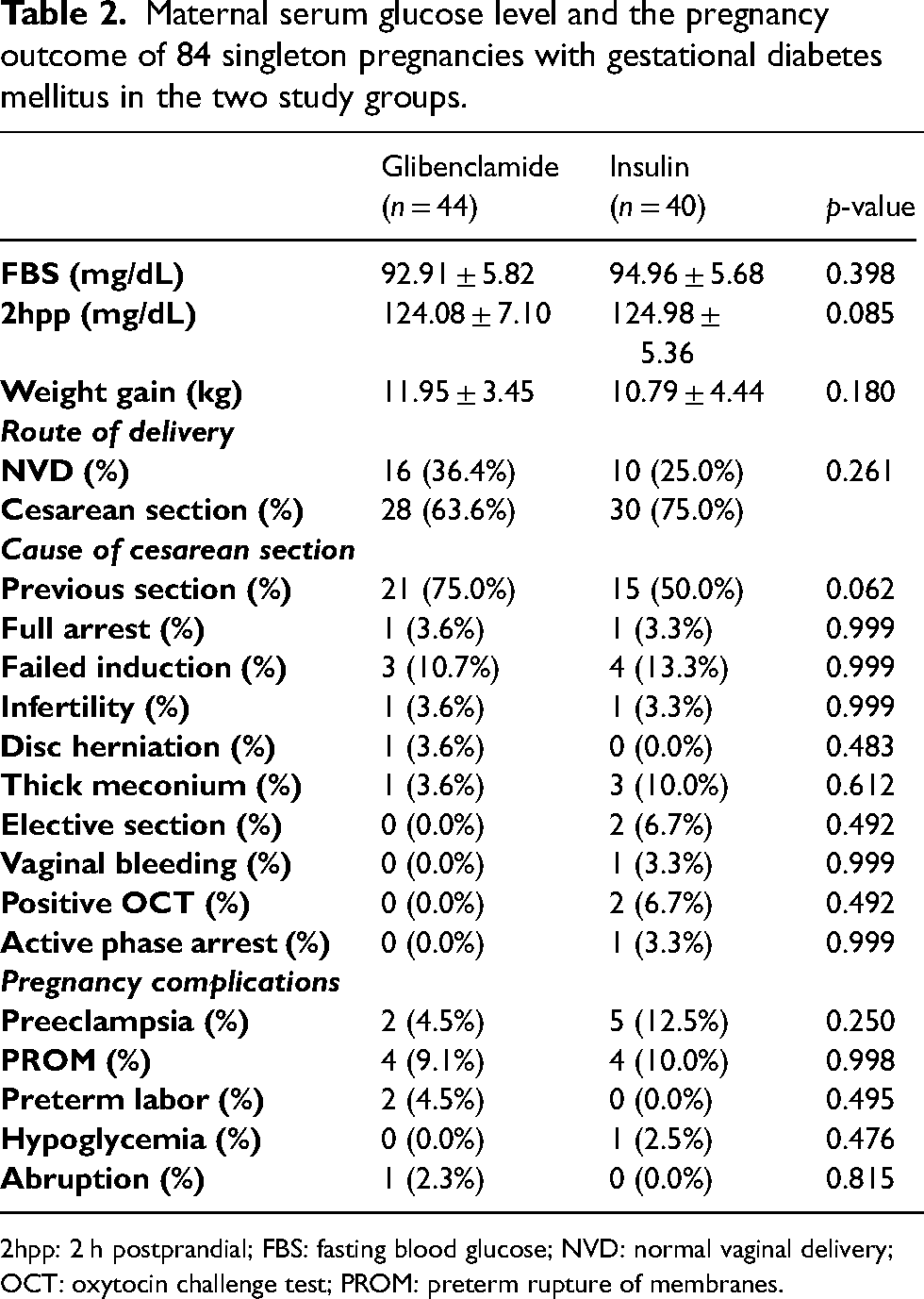
2hpp: 2 h postprandial; FBS: fasting blood glucose; NVD: normal vaginal delivery; OCT: oxytocin challenge test; PROM: preterm rupture of membranes.
There was no significant difference between the two study groups regarding the birth weight (p = 0.863) and Apgar score at 1 min (p = 0.190) and 5 min (p = 0.055). The rate of neonatal adverse events including hypoglycemia (p = 0.999), hyperbilirubinemia (p = 0.160), NICU admission (p = 0.852), and respiratory distress syndrome (p = 0.665) was comparable between the two study groups. Similarly, ultrasonography findings were not statistically different between the two study groups (Table 3). We ran a multivariate logistic regression analysis in order to compensate for confounders such as the maternal age, gestational age, and family history. We found that there was no statistically significant difference between the two study groups regarding the serum glucose control, maternal complication, and the neonatal outcome, even after compensating for the confounding factors.
Neonatal outcome of 84 singleton pregnancies with gestational diabetes mellitus in the two study groups.
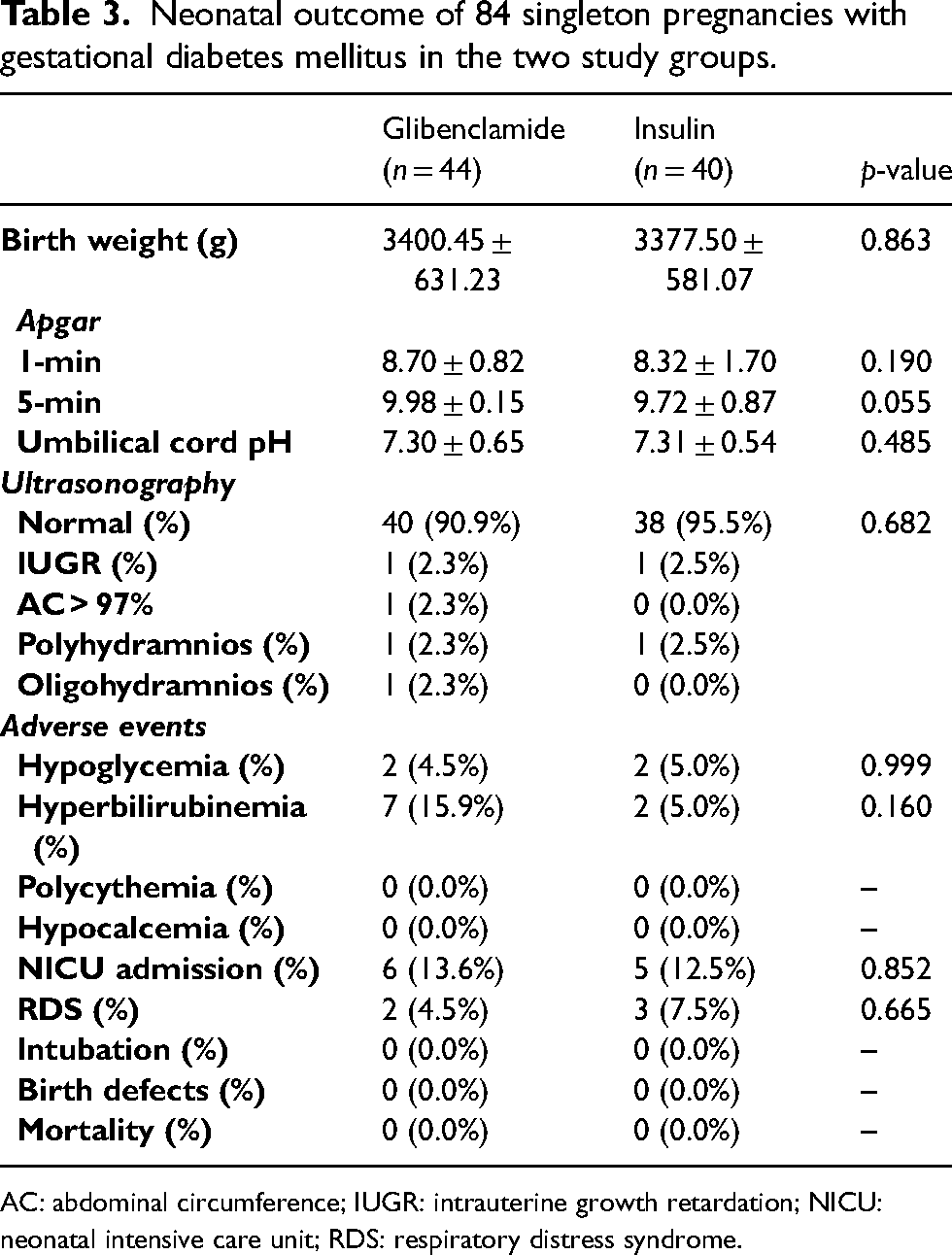
AC: abdominal circumference; IUGR: intrauterine growth retardation; NICU: neonatal intensive care unit; RDS: respiratory distress syndrome.
Discussion
The first-line treatment of GDM remains controversial, although commonly subcutaneous insulin, this is expensive and multiple injections are not easy or comfortable. 10 Oral hypoglycemic agents such as glibenclamide have been tested extensively but their results remain inconclusive.13,17 In the current clinical trial, we compared oral glibenclamide and subcutaneous insulin with regards to pregnancy and neonatal outcomes. We clearly demonstrated that the two therapies were comparable regarding glycemic control, as well as pregnancy and neonatal outcomes. Glibenclamide was as effective and safe as subcutaneous insulin. According to the results of the current RCT, we can recommend glibenclamide as the first-line treatment of GDM.
Several RCTs and meta-analyses have recently addressed the issues in detail. Recently, Helal et al. 20 performed a meta-analysis of 24 studies comparing the efficacy of glibenclamide to insulin in singleton pregnancies with GDM. Their pooled analysis revealed that glyburide was an effective and well-tolerated drug compared to insulin in the management of women with GDM, provided that the neonates were monitored for hypoglycemia and Apgar score. In addition, glyburide was associated with a lower rate of cesarean section, which may add to the potential clinical benefits of glyburide compared to insulin. 20 In a pharmacodynamic study, Shuster et al. 18 determined the insulin sensitivity (IS), β-cell responsivity, and disposition index in women with GDM utilizing a mixed-meal tolerance test (MMTT) before and during treatment with glyburide monotherapy, metformin monotherapy, or glyburide and metformin combination therapy. Glyburide significantly decreased the dynamic β-cell responsivity. Metformin and combination therapy significantly increased insulin sensitivity. Metformin (metformin and combination therapy) demonstrated a larger decrease in MMTT peak glucose concentrations than subjects taking only glyburide. Taking all these together, they showed that glibenclamide was as effective as metformin in improving insulin sensitivity and better in glycemic control in pregnant women with GDM. 18 Contrary to these results, Balsells et al. 13 conducted a meta-analysis that included randomized clinical trials comparing glyburide and insulin in GDM. They demonstrated that in short term, in women with GDM requiring drug treatment, glibenclamide was clearly inferior to both insulin and metformin, while metformin (plus insulin when required) performed slightly better than insulin. 13
In the current study, equal results were observed in the use of glibenclamide and insulin; this indicates that glibenclamide may be an effective and safe method for the treatment of GDM. However, Sénat et al. 17 compared glyburide with subcutaneous insulin in the prevention of perinatal complications in newborns of women with gestational diabetes. They demonstrated that the use of glibenclamide was associated with an increased rate of adverse neonatal outcomes; thus, they could not recommend glibenclamide for the treatment of GDM. 17 Another meta-analysis by Guo et al. 21 found that metformin could be a safe and effective treatment for GDM. Compared with insulin, glyburide had a higher increase in neonatal hypoglycemia. The use of glyburide in pregnancy for GDM women appeared to be unclear. 21
In our study, the rate of neonatal complications was comparable between the two study groups, and there was no significant difference between them regarding neonatal adverse events. However, Sénat et al. 17 demonstrated that glibenclamide administration was associated with increased adverse pregnancy outcomes (27.6% vs. 23.4%). The rate of neonatal hypoglycemia in the glyburide group was 12.2%; this is the same magnitude as the 9% reported by Langer et al. 22 in their insulin group, but much lower than the 33% reported by Bertini et al. 23 and the 25% reported by Silva et al. 24 in their glyburide groups. A prospective cohort study revealed that the neonates were considered to be at risk of hypoglycemia, including 40% of neonates born to a mother with diabetes. It was shown that with an on-treatment blood glucose level threshold of 47 mg/dL (2.6 mmol/L), neonatal hypoglycemia was not associated with adverse neurodevelopmental outcomes at 2 years compared with neonates with normal glucose levels. 25
We had some limitations in the current study. First, we included a limited number of patients in two study groups. Thus, the study might have been underpowered for subgroup analysis and cox regression analysis. However, in the power calculation, it was shown that the study had 80% power in primary and secondary endpoints. Complementary larger RCTs are required to add to the value of the current research. Second, we only recorded the main outcome measures and the neonatal and glycemic control. There are many variables that could be measured to help understand the pathophysiology including insulin resistance, serum levels of different hormones such as insulin, and growth hormones as well as other biometric variables. Further studies including all these variables could shed light on the mechanism of action in GDM and different treatment options. The last limitation was the lack of information on drug adverse events. We asked the patients to record all the adverse events related to glibenclamide and insulin therapy, but the patients did not do so appropriately. In addition, we did not record the price and expenses of each study arm. Thus, we could not comment on the expenses of each treatment option.
In conclusion, the results of the current randomized clinical trial demonstrated that in short term, in women with gestational diabetes mellitus requiring drug treatment, despite having a 5% failure rate of glibenclamide (indicating that it may not be as effective as insulin) and despite the probability of maternal hypoglycemia induced by glibenclamide, glibenclamide was associated with appropriate serum glucose control and comparable pregnancy and neonatal outcome. However, we have no long-term follow-up of offspring exposed to glibenclamide, so more RCTs are suggested to complement the results of the current study.
Footnotes
Acknowledgements
We would like to thank all the patients and their families for participating in the current study. The study is extracted from the thesis project by Dr Lida Tahamtani as partial fulfillment of the requirements for the degree of specialty in obstetrics and gynecology (no. 6115). The authors would like to thank Shiraz University of Medical Sciences, Shiraz, Iran, and also the Center for Development of Clinical Research of Nemazee Hospital, and Dr Nasrin Shokrpour for editorial assistance. We would also like to acknowledge the editorial assistance of Diba Negar Research Institute leading to improvements in the language and style of the manuscript.
Authors’ contribution
Azam Faraji: Project development, Data Collection, Data analysis. Lida Tahamtani: Data Collection, Data analysis. Najmeh Maharlouei: Data analysis. Nasrin Asadi: Project development, Data collection, Data analysis, Manuscript writing/editing. All authors read the manuscript and approved it.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.