
Abstract
Background
Pregnancy in women with cystic fibrosis (CF) is becoming more common. Long-term metabolic issues such as diabetes are also becoming more common and have potentially important impacts on pregnancy outcomes. This study aimed to assess the impact of diabetes on pregnancy outcomes for women with CF.
Methods
We undertook a retrospective chart audit of pregnancies to women with CF at the two tertiary obstetric hospitals in Southeast Queensland associated with CF and transplant management clinics between 2006 and 2016.
Results
A total of 38 pregnancies among 26 women were identified. Four women (five pregnancies) had cystic fibrosis-related diabetes (CFRD) diagnosed prior to pregnancy, and 12 women (15 pregnancies) developed gestational diabetes (GDM) complicating pregnancy. CFRD and GDM were associated with higher rates of delivery complications, prematurity, and the need for neonatal intensive care unit admission.
Conclusion
Diabetes is common during pregnancy in women with CF and impacts pregnancy outcomes.
Introduction
Cystic fibrosis (CF) is an inherited disorder caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene. People with CF are living longer with a median survival of Australians estimated to be 53 years in 2019, 1 and recent analyses suggest further reductions in morbidity and mortality with the novel CFTR modulator therapies.2,3 Of the 3445 people with CF in Australia in 2019, 882 were adult females, and this proportion continues to rise. 1 Therefore, it is not surprising that pregnancy in women with CF is becoming more common. In the United States, the number of pregnancies among women with CF has consistently increased from 139 in 1999 to 310 pregnancies in 2019. 4 Historically, pregnant women with CF had an increased risk of worsening pulmonary function and death as well as increased rates of prematurity and low birthweight in neonates. 5 However, multiple studies in recent years have shown that outcomes in pregnant women with CF are improving, even in those with reduced pulmonary function prior to pregnancy.6–9
Another consequence of the increased life expectancy of people with CF is an increase in diabetes given the positive correlation between the prevalence of CF-related diabetes (CFRD) and age.10,11 However, there is very little data regarding outcomes and optimal management in women with CFRD and women with CF who develop gestational diabetes (GDM) during pregnancy. One single-site cohort study with 36 women with CF found higher rates of preterm premature rupture of membranes, earlier gestational age of delivery, and lower birthweight in women with CFRD compared to women with CF without diabetes in the United States, 12 while a French multisite cohort study with 232 women only found an increase in the rates of caesarean delivery. 13 More data from larger cohorts is required to further elucidate pregnancy outcomes associated with CFRD and GDM.
Only two studies from the same adult CF center in Sydney have reported pregnancy outcomes in women with CF in Australia in 1998 and 2011.7,14 Therefore, the aim of this study was to identify pregnancy outcomes for women with CF in Southeast Queensland at the two tertiary obstetric hospitals associated with CF multidisciplinary clinics. In addition, we aimed to compare outcomes between the women with CFRD, those who developed GDM during pregnancy, and those who did not have diabetes during pregnancy.
Methods
This retrospective cohort study was conducted at two tertiary obstetric hospitals and their associated CF and lung transplant clinics, either co-located or in nearby institutions. This study was granted ethical clearance by the Human Research Ethics Committee (HREC/17/QRBW/239) and did not require individual patient consent.
Women with a pregnancy managed at either an obstetric hospital from June 2006 to July 2016 or who had a diagnosis of CF were included in the study. Participants were identified from each hospital's local obstetric database, and medical records were retrieved for detailed chart review. Where applicable, data were cross-referenced between obstetric and CF clinical databases and records for respiratory and other CF-related outcomes. Data were collected regarding baseline health status, including age, baseline body mass index (BMI), underlying mutation, baseline lung function, and the presence of any CF complications including transplant status and CFRD. Information regarding the pregnancy course was collected including measures of forced expiratory volume in one second (FEV1), pregnancy complications such as GDM, and data regarding CF and non-CF-related hospitalizations. GDM was diagnosed in accordance with the local clinical guidelines at the time of diagnosis. Specifically, this was the 1991 Australasian Diabetes in Pregnancy Society criteria prior to 2015 and the International Association of the Diabetes and Pregnancy Study Groups after 2015. Pregnancy outcomes were collected as well including gestational age, birthweight, and any maternal or fetal complications.
Data analysis was conducted using SPSS 26.0 (IBM, Armonk, NY). Descriptive statistics were used to report outcomes from the study. Data are presented as means ± standard deviations and frequencies and percentages where appropriate. Given the small sample size, we have not undertaken a formal statistical comparison of groups.
Results
In total, there were 38 pregnancies among 26 women identified in the study period. One woman had four pregnancies, one woman had three pregnancies, seven women had two pregnancies, and 17 women had one pregnancy. There was one twin pregnancy, so 39 infants were included in the study. Four women had children born prior to the study period, 10 women had prior miscarriages, and one woman had a prior intrauterine fetal demise. Two women had prior lung transplants, and these transplants were 10 and 14 years prior to delivery. All women had an FEV1 greater than 50% at the start of pregnancy. Baseline characteristics and measures of illness severity are summarized in Table 1.
Baseline characteristics.

BMI: body mass index; FEV1: forced expiratory volume; CFRD: cystic fibrosis-related diabetes; IVF: in vitro fertilization; IUI: intrauterine insemination.
Five pregnancies among four women were complicated by CFRD diagnosed prior to the pregnancy, all of which were well-controlled with HbA1c ≤ 7%. CFRD was managed with insulin in four pregnancies and no pharmacotherapy in one pregnancy. Fifteen pregnancies among 12 women were complicated by GDM diagnosed during the pregnancy. The average gestational age of diagnosis was 17.9 weeks (range: 6.1–30.3 weeks). Nine of these 15 pregnancies were managed with insulin, one with both insulin and metformin, and five did not receive pharmacotherapy.
Obstetric and neonatal outcomes among all women are presented in Table 2, and outcomes compared between women with CFRD, GDM, and without diabetes are presented in Table 3. Among the 38 pregnancies, 21 required at least one hospital admission for non-obstetric causes. Of those, 18 pregnancies required admission for a pulmonary exacerbation. There were no differences in admission rates or indications between pregnancies that were and were not complicated by diabetes.
Aggregate pregnancy outcomes.
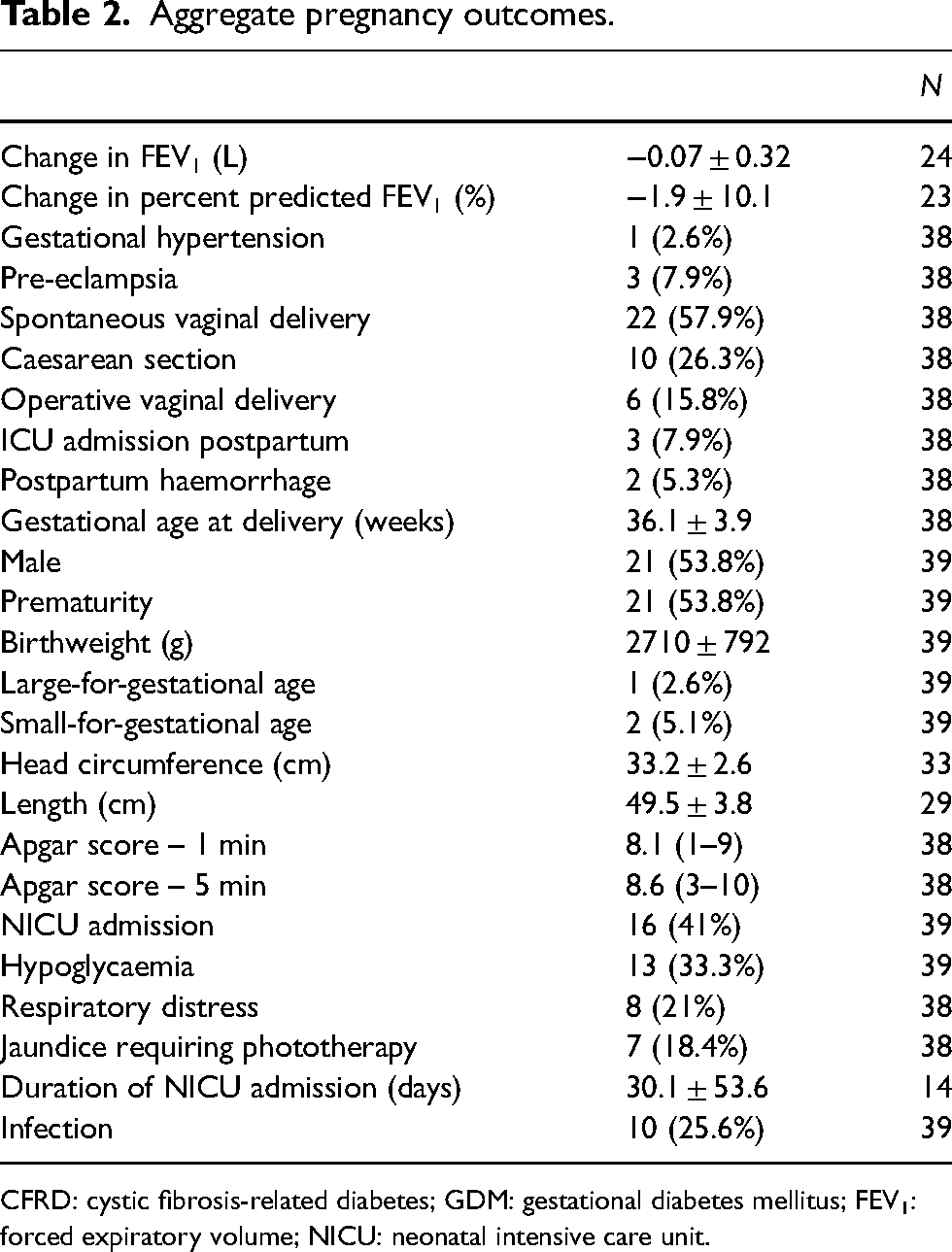
CFRD: cystic fibrosis-related diabetes; GDM: gestational diabetes mellitus; FEV1: forced expiratory volume; NICU: neonatal intensive care unit.
Pregnancy outcomes by diabetes type.

CFRD: cystic fibrosis-related diabetes; GDM: gestational diabetes mellitus; FEV1: forced expiratory volume; NICU: neonatal intensive care unit.
including one long stayer (89 days NICU stay due to preterm delivery at 27 weeks in the setting of pre-eclampsia, IUGR and fetal distress), 7.0 ± 6.6 without that infant.
including one long stayer (196 days NICU stay due to preterm labour and delivery at 24 weeks), 4.1 ± 2.3 without that infant.
The average gestational age of delivery across all groups was 36.1 weeks, and 54% of infants were premature. While 31.5% (6/19) of the preterm deliveries were spontaneous, the most common reason for preterm delivery was worsening respiratory status or other CF-related concerns (8/19). Only one patient was delivered due to her diabetes, and this patient had GDM. Among the 15 women who required a caesarean section or operative vaginal delivery, the indication for this delivery mode was CF in 4 women with no differences between groups. All women were alive at the time of discharge after delivery. Three women required ICU admission in the postpartum period, two for postpartum haemorrhage and one for severe pre-eclampsia, portal hypertension, and bacteraemia. Both women who had prior lung transplants had CFRD, required preterm delivery (one due to respiratory function concerns and one for severe pre-eclampsia), and required ICU admission postpartum. Table 3 shows the outcomes for women with CFRD including and then excluding the two women with a prior lung transplant.
Sixteen of the 39 infants required neonatal intensive care unit (NICU) admissions, with an average length of stay of 30 days (range: 1–196 days). Most infants were admitted to the NICU for prematurity (11/16). There were two infant deaths in this cohort. One infant was delivered at 23 weeks 5 days of gestation due to premature rupture of membranes, and the infant died shortly after birth. The other infant was born at 24 weeks 2 days of gestation due to preterm labour and died after spending 196 days in the NICU. All infants were appropriate-for-gestational age apart from one infant who was large-for-gestational-age (LGA, > 90th percentile) and two who were small-for-gestational-age (SGA, < 10th percentile). The infant who was LGA was born to a mother with CFRD, while the two SGA infants were born to women without diabetes. Neither of the SGA infants had mothers with pre-eclampsia. Infants born to women with GDM and CFRD were more likely to have hypoglycaemia after birth. When comparing women with CFRD to those with GDM, there was also a trend towards higher rates of premature delivery and NICU admission in women with CFRD.
Discussion
This study aimed to characterize current pregnancy outcomes for women with CF in Queensland as well as compare outcomes between women with and without diabetes. The findings of this study support that pregnancy outcomes in women with CF have improved in Australia and are consistent with international results.4,6–9 There were no maternal deaths in the study, and the overall decrease in FEV1 during pregnancy was minimal with some women even having improvements in their lung function. Similar findings were previously reported in Australia by Lau et al., 7 and they noted this is likely reflective of intensive monitoring and possibly increased patient compliance due to pregnancy. However, one limitation of this study is that study was limited to tertiary obstetric hospitals. This may have resulted in the selection of women who have better access to pre-conception counselling, specialized care and health optimization prior to pregnancy, which could improve their outcomes. This is supported by the fact that all women had an FEV1 greater than 50% at the start of pregnancy.
Although maternal outcomes were overall positive, this minimal reduction in lung function was in the setting of high rates of premature delivery. While less than 50% of preterm deliveries were secondary to the mother's respiratory function, prematurity was ultimately responsible for the majority of NICU admissions and both infant deaths. Therefore, this highlights the difficult balance between the risk to respiratory function with prolonged pregnancy and the risk to the neonate with preterm delivery.
With the introduction of the new CFTR modulators and the resulting improvements in health, it is likely that pregnancy rates in women with CF will continue to rise. However, the data on CFTR modulator use in pregnancy is limited. While the preliminary data is promising with no evidence of teratogenic effects in the preclinical data and no strong evidence of harm in the few published case series, the long-term consequences remain unknown and modulators are still not recommended to be continued in pregnancy.15–17 No women received CFTR modulator therapy in this study which, although surprising given the clinical benefit found from these agents, is likely reflective of this recommendation. However, registry-based studies in pregnant women on CFTR modulators are underway which may change future recommendations about modulator use.
This study is the first in Australia to report the outcomes associated with diabetes in pregnancies affected by CF. We found infants born to women with CFRD and GDM had a trend towards higher rates of neonatal hypoglycaemia, NICU admission, and preterm birth. While the findings were somewhat different from Reynaud et al. who found an increased rate of caesarean section, both studies support that while there may be increased risks, women with CF and diabetes can have a successful pregnancy. 13 Management of diabetes in patients with CF is complicated by the balance between limiting hyperglycaemia while ensuring adequate nutrition in the presence of malabsorption, particularly when a fetus measures SGA in the setting of hyperglycaemia. Given there were only one LGA and two SGA infants in this study, we do not have enough data to inform the management of diabetes in the setting of CF, but this should be a focus in future cohorts. Finally, only one patient had diabetes listed as an indication for delivery, suggesting that the presence of diabetes in CF patients has a limited impact on delivery timing and the rate of premature delivery.
When comparing women with CFRD and their counterparts with GDM, the women with CFRD in this study had a trend towards worse outcomes. Specifically, they had higher rates of premature delivery, maternal ICU admission postpartum, and infant NICU admissions. In this study, we also found that those with GDM had a trend toward less reduction in their FEV1 throughout pregnancy than those without diabetes or with CFRD. This is not statistically significant and therefore difficult to place clinical emphasis on, but the more important conclusion is that GDM does not appear to be a risk factor for worsening lung function in pregnancy. However, one limitation of this study was the low rates of CFRD, so these statistical comparisons between women with CFRD and GDM should be interpreted with caution. In addition, it is possible the difference in outcomes was secondary to the severity of their underlying CF and not the CFRD itself. Another factor is that we included two women with a previous lung transplant. While they had stable transplants more than 10 years prior to pregnancy, both had CRFD and both required preterm delivery for maternal concerns and were admitted to ICU postpartum. We recognize their data may influence the dataset but have not excluded them as women with lung transplants are also increasingly becoming pregnant and including their data in the available literature are important. Examining the CFRD cases without the transplant cases still demonstrates high rates of pregnancy complications such as preeclampsia, C-section, NICU admission and LGA infants.
Overall, pregnancy outcomes are improving for women with CF. While the impacts of diabetes on pregnancy are well established, managing GDM in patients with CF and CFRD present unique challenges. This study supports the conclusion that CFRD carries likely similar risks to GDM and should not be overlooked. Further research should focus on obtaining larger cohorts to more accurately identify the outcomes associated with CFRD compared to GDM. In particular, a collaboration between CF services to pool data and develop registries is crucial to improving care for pregnant women with CF.
Footnotes
Acknowledgements
The authors would like to thank the multidisciplinary healthcare teams who provided care to the women in this study including the CF and Lung Transplant teams at The Prince Charles Hospital, the CF team at Mater Hospital Brisbane, and the Obstetric Medicine teams at Mater Mother's Hospital and the Royal Brisbane and Women's Hospital for making this study possible.
Contributorship
HLB conceived the study, developed the protocol, and obtained ethical approval. SJD, MF and HLB collected data for the study. SJD performed data analysis and wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Human Research Ethics Committee of the Royal Brisbane & Women's Hospital approved this study (HREC/17/QRBW/239).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
A waiver of consent was granted by the Human Research Ethics Committee for this study.
Guarantor
HLB is the guarantor of the present work.