
Abstract
Maternal mortality is the death of a woman while pregnant or within 42 days of the end of pregnancy. Late maternal deaths are from 42 to 365 days thereafter. Maternal mortality is an important surrogate indicator of a woman's overall health, social and economic status, and the provision of antenatal and emergency obstetric care at regional and national levels. Canada does not have a national system to report on maternal mortality; rather, maternal death investigations fall under the legal purview of coroners and medical examiners within each individual province or territory. Furthermore, the Canadian Perinatal Surveillance System is limited by its access to a comprehensive dataset. Hence, there is no accurate national picture of mortality prevalence or trends. The implementation of a national confidential enquiry system is a crucial step toward detailing pregnancy and post-pregnancy maternal mortality in Canada and should be organized in accordance with existing successful international systems.
Introduction
This analysis describes maternal mortality in Canada, within a global context. Details are given about national and regional mechanisms for capturing maternal deaths during pregnancy, and up to 1 year thereafter. Finally, we describe international best practices for maternal mortality surveillance and prevention.
What is a maternal death?
A maternal death is an often-preventable event that has devastating consequences for families and care providers. Maternal mortality is widely acknowledged as an important societal indicator of overall health,1,2 the individual's social and economic status,3,4 her access to antenatal and emergency obstetric care, and the provision of that care at both regional and national levels. 5
Maternal mortality has previously been defined as ‘the death of a woman while pregnant or within 42 days of ending of pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes’. 6
The 42-day limit conventionally used to define of a maternal death has been challenged.7–9 In 1993, the WHO Working Group on Maternal Mortality extended that definition to up to one year after the end of a pregnancy. Those deaths beyond 42 days, but within 365 days after the end of a pregnancy, are classified as late maternal deaths. 6 Maternal mortality may be considered as either direct or indirect. Direct maternal deaths ‘result from obstetric complications related to pregnancy, labour, and the puerperium, or from interventions, omissions, incorrect treatment, or from a chain of events resulting from any of the above’. 6 A death due to a pre-existing disease, a condition that develops over the course of pregnancy, or one that is aggravated by the physiologic effects of pregnancy, is classified as an indirect maternal death. 6
Global maternal mortality
Globally, maternal deaths declined in the last century partly because of advances in obstetric care and improved family planning. From 2000 to 2017, the relative global maternal mortality rate declined by 38%. 10 Yet, the WHO estimates that more than 300,000 women continue to die each year from pregnancy or childbirth-related complications. 11 In 2017 alone, approximately 810 women died each day from preventable causes related to pregnancy and childbirth. 12 Sub-Saharan Africa and Southern Asia accounted for approximately 86% of these deaths (Figure 1), with two-thirds (196,000) from sub-Saharan African nations. 11

Global maternal mortality ratios (MMR) in 2017. MMR are defined as the number of women who die from pregnancy-related causes per 100,000 livebirths. Countries with the five highest national MMRs (dark red) and three lowest MMRs (blue dashed) are indicated, in addition to the United States, Canada, United Kingdom, Australia, and New Zealand (black). Sub-Saharan Africa and Southern Asia accounted for approximately 86% of the estimated global maternal deaths in 2017. Map modelled using most recent global data from the World Health Organization.
Despite the United Nations Millennium Development Goal for a 75% reduction in maternal mortality between 1990 and 2015, the reported maternal mortality rate in the US more than doubled between 2000 and 2014 13 – potentially partly an epiphenomenon of improved ascertainment of maternal deaths within national death statistics datasets.13,14
Canadian maternal mortality in a global context
In 2010, the WHO suggested that there was a sharp increase in maternal mortality in Canada. 15 These findings prompted the Society of Obstetricians and Gynaecologists of Canada (SOGC) to work with federal and provincial partners to review maternal mortality surveillance. 16 The investigating committee found that national maternal health surveillance faced serious barriers related to data access, timeliness and completeness. Moreover, they observed little standardization across jurisdictions with respect to definitions, data collection or maternal mortality review processes.16,17 Although several provinces and territories have since established their own maternal death review committees, there is no national system that synthesizes and reports on all maternal deaths; hence, there is no accurate national picture of mortality prevalence or trends.16,17 Complicating the issue is the fact that, since the initial work by the SOGC, the demographics and risk profiles of child-bearing women in Canada have changed, including more women with advanced maternal age, a greater number of medical comorbidities and substance use, and a growing number of immigrant women who are now part of Canada's childbearing population. 16
Although the global maternal mortality ratio (MMR) declined by 45%, from 385 in 1990 to 211 per 100,000 livebirths in 2017, most recent data available from the Public Health Agency of Canada estimates that Canada's MMR, excluding Quebec, increased from 5.1 in 1990 to 11.9 per 100,000 in 2015.18,19 Statistics Canada reported that the national MMR was 3.4 in 2000 and 7.1 per 100,000 in 2015, considering all provinces and territories, rising to 8.4 per 100,000 livebirths in 2020. 20 The SOGC and international agencies, such as the WHO and UNICEF, suggest that maternal death rates may be higher than those reported by Statistics Canada (Figure 2). If true, then Canada's national MMR might actually be closer to 10.0 per 100,000 livebirths, placing it between the US and UK in ranking, 21 and double the rate of other high-income countries, such as the Netherlands, Ireland and Japan (Figure 3). 21
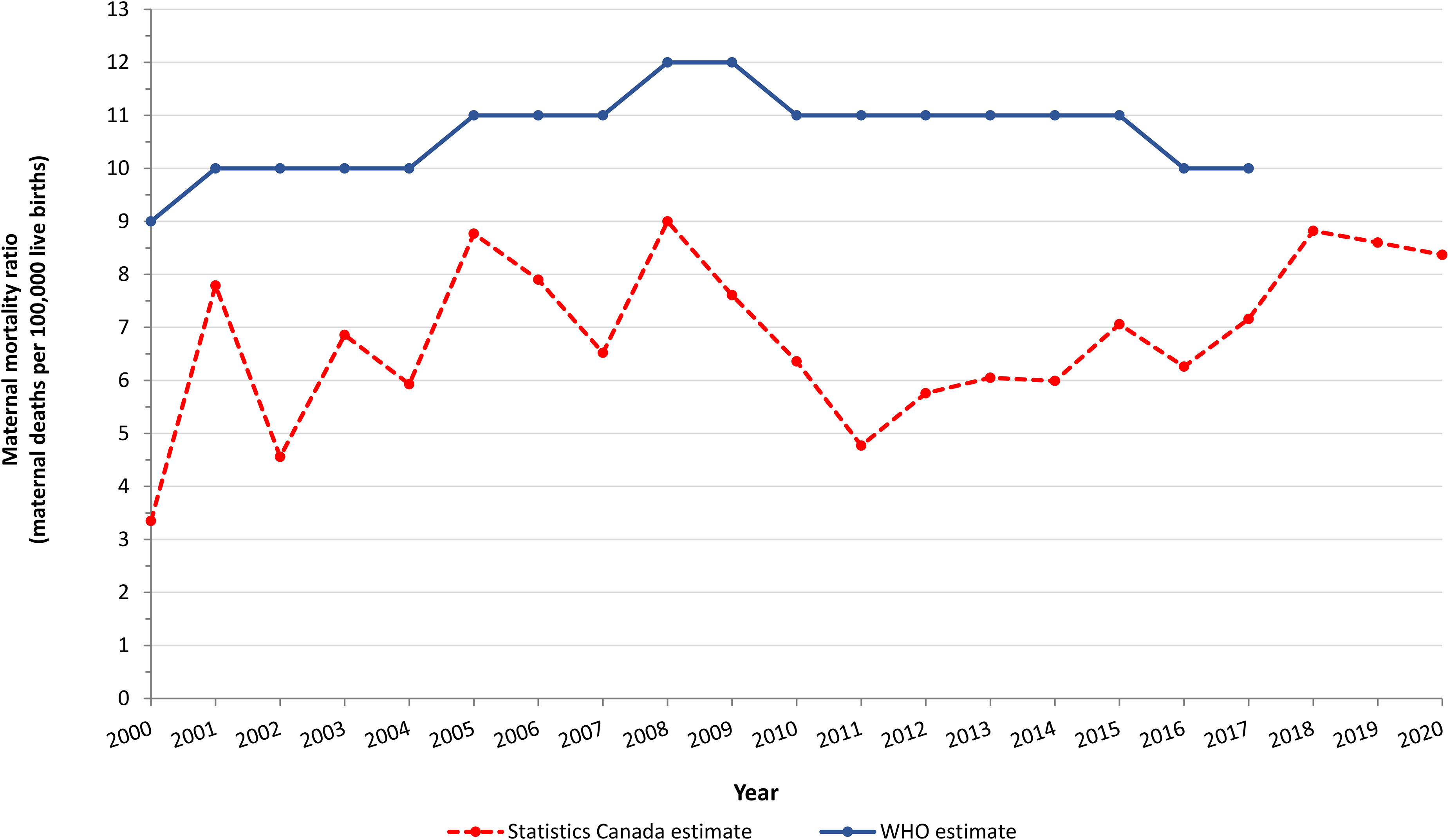
Maternal deaths per 100,000 livebirths in Canada, 2000 to 2020. Estimates are based on data published by Statistics Canada (dashed red) and the World Health Organization (WHO [blue]). The latest global data available from the WHO is from 2017. The WHO used a correction coefficient of up to 60% for national data from Canada to account for underreporting.

Maternal deaths per 100,000 livebirths in 2017 among the top-10 high-income countries with the largest gross domestic product in 2021. The World health organization assumes that Canada's maternal mortality ratio is nearly double (red) that reported by Statistics Canada (blue). Presented data are from Statistics Canada and Trends In Maternal Mortality 2000 to 2017: Estimates by WHO, UNICEF, UNFPA, World Bank and UNPD.
Of note, maternal deaths occur at disproportionately higher rates in vulnerable Canadian sub-populations, including Black and Indigenous women.19,22,23 Data from the United States indicates that American Indian and Black women have about a 2–3 times higher maternal mortality rate than non-Hispanic White women. 24 Such disparities in maternal mortality among these sub-populations are a serious concern, and remain understudied in Canada.
Severe maternal morbidity as a proxy for mortality
Maternal mortality statistics do not necessarily reflect morbidity arising during pregnancy or after birth. 25 Inroads have been made in the study of severe maternal morbidity (SMM) – a ‘near miss’ proxy for maternal mortality.26–28 There is a dose-response relation between the rate of SMM and a woman's chances of dying during pregnancy, childbirth or within 42 days postpartum. 23 As SMM may be up to 100 times more common than maternal death, it can be used as an indicator of quality of care during pregnancy and postpartum, 29 and also enables a more robust analysis of factors that may also contribute to maternal deaths, as well as potential health disparities. 30 It is also recognized that morbidity from substance use and mental illness also significantly contributes to maternal deaths in Canada,31,32 alongside advanced maternal age 33 and pre-existing medical conditions. 18
Maternal mortality surveillance in Canada
Canadian perinatal surveillance system
Currently, maternal mortality surveillance in Canada relies on provincial and territorial hospitalization data available in the Discharge Abstract Database provided by the Canadian Institute for Health Information (CIHI), and also Vital Statistics data from Statistics Canada. CIHI data appear to provide a more accurate picture of maternal mortality than the death registration database from Statistics Canada, 34 but CIHI lacks information from Quebec. Even so, maternal mortality surveillance using the CIHI databases provides limited information about the clinical and social context surrounding a peri-pregnancy death. 35
The Canadian Perinatal Surveillance System (CPSS) is the national health surveillance program tasked with reviewing national maternal mortality data, under the Public Health Agency of Canada. The CPSS publishes their findings through the Canadian Perinatal Health Report and peer-reviewed literature. The inability of the CPSS to have access to comprehensive national data is a recognized limitation. 35
The WHO uses an adjustment coefficient for Canada of 60% upward, to correct for perceived under-reporting of maternal deaths. 36 Efforts to correct this perceived under-capture of deaths has been hindered by Canada's province-based approach to healthcare administration, inconsistencies in data collection on pregnancy and mortality between databases, barriers to data sharing, and a lack of funding, oversight and personnel. 16 Progress is now being made by the SOGC, in partnership with four provincial perinatal programs (Alberta, British Columbia, Nova Scotia and Ontario), using models from the WHO, 37 the UK 38 and the US CDC 39 to develop a Canadian toolkit for a confidential inquiry into maternal mortality and SMM. That toolkit will provide policies and procedures, standardized data and information fields, and guidelines for maternal morbidity and mortality review best practice, aligning with a confidential inquiry-type system. Moreover, a confidential inquiry system, such as the UK-MBRRACE, can provide a template for Canadian healthcare providers to implement targeted preventive and intervention strategies.
Regional coroners and medical examiners
Canada lacks an overarching federal authority responsible for pregnancy death investigations, which fall under the legal purview of each individual province or territory (Table 1). 35 Only six provinces have a mandated maternal death review process in place; even so, there are inconsistencies therein related to definitions and data collection protocols. For example, some provinces use the WHO's definition of a maternal death up to 42 days after the end of pregnancy, others include deaths up to 365 days postpartum, and some do not capture the postpartum period at all. 16
Regional differences between timing of maternal deaths captured on death certificates by Canadian province or territory.
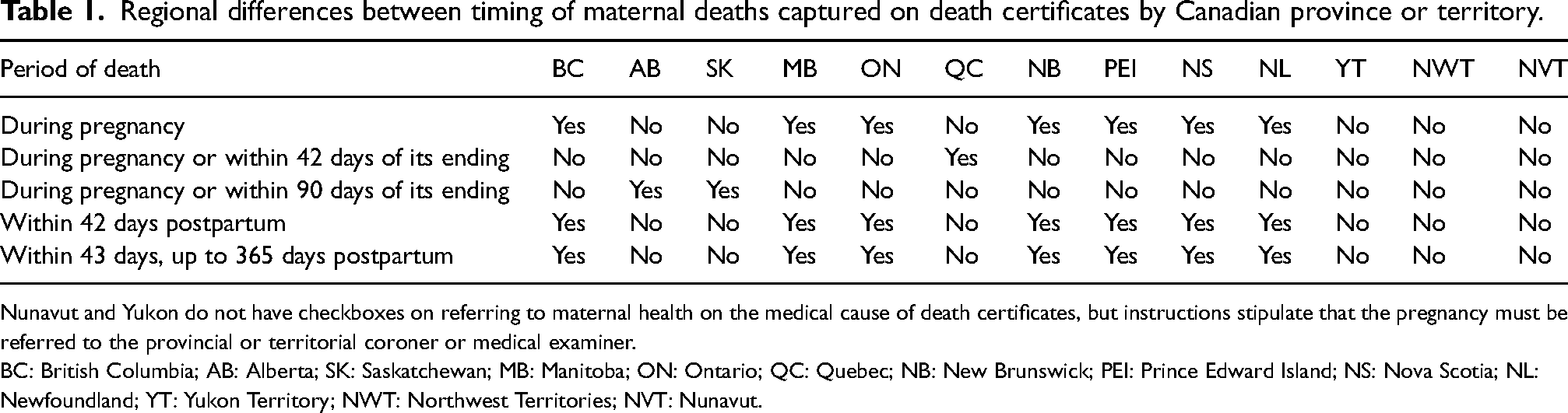
Nunavut and Yukon do not have checkboxes on referring to maternal health on the medical cause of death certificates, but instructions stipulate that the pregnancy must be referred to the provincial or territorial coroner or medical examiner.
BC: British Columbia; AB: Alberta; SK: Saskatchewan; MB: Manitoba; ON: Ontario; QC: Quebec; NB: New Brunswick; PEI: Prince Edward Island; NS: Nova Scotia; NL: Newfoundland; YT: Yukon Territory; NWT: Northwest Territories; NVT: Nunavut.
By virtue of Canada's province-based approach to healthcare administration and legislation, two different death investigation systems have emerged: the coroner's system and the medical examiner's system. 35 The coroner's system originated in medieval England, 40 and is used in most provinces and territories, including Ontario. 35 In Ontario, the Coroner's Act legislates that a coroner must be a physician. 40 Across other jurisdictions, coroners are elected officials with no medical professional training. 41 The medical examiner's system originated in the US. Medical examiners are physicians, often pathologists, appointed by the regional authority. 41 In Canada, the medical examiner's system is used in Alberta, Manitoba, Nova Scotia and Newfoundland and Labrador. 35
All Canadian coroner and medical examiner systems are required to investigate certain types of deaths to identify the decedent, determine the cause of death, and establish the manner of death. Most coroners and medical examiner systems are also mandated to conduct a ‘public enquiry’. Following an investigation, the coroner or medical examiner can make recommendations to the chief coroner or chief medical examiner as to whether an inquest or an inquiry should be held. The purpose of a public inquiry is to develop and disseminate policy recommendations to prevent similar deaths from occurring in the future.
International best practices in maternal mortality surveillance
UK confidential enquiry into maternal deaths
The UK confidential enquiry into maternal deaths (Mothers and Babies: reducing risk through audit and confidential enquiry; MBBRACE-UK) is a widely respected national surveillance system that conducts reviews of maternal mortality events in the UK, Ireland and Wales. MBBRACE-UK is regarded as the global reference standard, with the methodology having been adopted elsewhere.42,43
MBBRACE-UK reviews nationwide data collected by midwives, nurses, obstetricians, coroners, vital statistics and linked birth-death records that are submitted on a timely basis. 44 Thus, MBBRACE-UK generates a comprehensive and near-complete picture of the social and clinical circumstances surrounding each documented maternal death.
The UK Obstetric Surveillance System (UKOSS) was initiated in 2005 to study uncommon pregnancy complications and SMM events. 45 UKOSS is used in all obstetric units in the UK, and requires collection of data related to all cases of a particular pregnancy condition, especially severe cases and near-miss events. Data collected through the system are more detailed than from routine hospital records, and are captured by appropriately skilled personnel.
US pregnancy mortality surveillance system
In April 2016, a collaboration between the CDC, Association of Maternal and Child Health Programs, and Merck (on behalf of their Merck for Mothers program) was formed ‘to support the functions of regional Maternal Mortality Review Committees through common data’. 39 As part of these efforts, the Maternal Mortality Review Information Application was developed. The platform is a centralized data storage system for local death review committees, to provide clinical and non-clinical data, with the aim of improving documentation of maternal mortality and SMM across the US.
The WHO's maternal death and surveillance response
In regions lacking a comprehensive vital statistics database, a maternal death and surveillance response (MDSR) system is an effective strategy to collect data on maternal deaths. MDSR is a continuous cycle that builds on established approaches, such as maternal death reviews. 37 The MDSR system cycle begins with the accurate and timely identification of a maternal death, notification of the death to the appropriate authorities, followed by an expert committee review, and deployment of any measurable actions to prevent such a future death. The MDSR system has been adopted in low- and middle-income countries, including Uganda, 46 Sierra Leone, 47 and Cameroon. 48 MDSR has also been utilized in humanitarian settings, such as in refugee camps. 49
Conclusion
This review outlines how maternal mortality is measured in Canada and elsewhere. Several options are outlined for improving and standardizing current processes, which are needed to ensure that a comprehensive review system is in place for documenting all maternal deaths during and after pregnancy, including up to 1 year thereafter. Canadian stakeholders have recently refocused efforts towards developing a standardized national system, largely based on the UK model of confidential enquiry. Existing international best practices for maternal mortality surveillance and prevention should continue to be adopted in Canada.
Footnotes
Contributorship
KA and JGR researched literature and conceived the study. KA wrote the first draft of the manuscript. Both authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Physicians’ Services Incorporated Foundation (grant number 22-13).
Ethical approval
This work did not require approval from a research ethics board.
Informed consent
This work did not require written consent.
Guarantor
KA.