
Abstract
Background
There are limited data regarding intermittently scanned continuous glucose monitoring (isCGM) in pregnancy for women with Type 2 diabetes. We have tested the acceptability and feasibility of an isCGM method using Libre device.
Method
In a hospital-based service improvement project, 23 pregnant women (March 2022-April 2023), with Type 2 diabetes got isCGM for monitoring from 20 weeks until delivery. Women completed a structured and validated questionnaire assessing satisfaction, equipment issue, relationship with diabetes team.
Results
Two-thirds of the women were satisfied with the convenience and found it reliable. 86% wanted to use it for future pregnancies, and 90% would recommend it to others. Sensor falls off was seen in three obese women and about a tenth felt the reliability was poor in extreme ranges of sugar levels. The relationship with the diabetes team was rated high.
Conclusion
isCGM could be a useful and well-received tool for improving glycaemic control in pregnancies with Type 2 diabetes.
Keywords
Background
Type 2 diabetes mellitus (T2DM) accounts for 54% of women entering pregnancy with diabetes, doubling in the last two decades. 1 Women with T2DM face additional healthcare inequalities and are frequently not prepared for pregnancy. In the UK, women with T2DM are more likely to be of non-White Ethnic groups and live in areas of social deprivation. 1 The rate of neonatal deaths is also higher in T2DM mothers than in those with type 1 diabetes (T1DM). 2 T2DM, poor glycated haemoglobin (Hba1c) control, and social deprivation are independent risk factors for perinatal death. Based on the findings of the CONCEPPT trial in women with T1DM in pregnancy, 3 NICE have recommended the use of continuous glucose monitoring (CGM). 4 The National audit report highlighted the need to evaluate whether Libre or intermittent scanning CGM (isCGM) use could improve levels of glucose control, including target HbA1c attainment, and ultimately affect neonatal outcomes in pregnant women with T2DM. 1
Many women with T2DM are inexperienced in performing blood glucose monitoring when they become pregnant, with several of our patients reporting they found capillary fingerstick testing mentally and physically burdensome. 5 Compliance rates with finger stick monitoring can be variable, with many women not performing the recommended minimum amount of daily readings by NICE (four readings per day, including fasting and one-hour post-breakfast, lunch, and dinner). Poor compliance with monitoring makes it challenging to tailor treatment to individual needs, likely leading to undertreatment.
CGM could offer an alternative and improve compliance and engagement with diabetes care. The first step in evaluating the use of CGM in pregnant women with T2DM is to determine the acceptability of the technology. However, few studies have explored the role of isCGM for women with T2DM in pregnancy. It is not known whether this technology can improve compliance and engagement with glucose monitoring during pregnancy, or what the optimal time in range for women with T2DM might be in order to improve perinatal outcomes.
As part of a clinical service improvement project to improve glucose monitoring compliance in women with T2DM, we sought to determine the feasibility and acceptability of using isCGM in this population.
Methods
A service improvement project was conducted within the Oxford University Hospitals (OUH) NHS Foundation Trust, UK. The OUH provides maternity care across two sites (the John Radcliffe Hospital in Oxford and Horton Hospital in Banbury) for around 7500 pregnancies each year. Of these, about 50 are pregnant people with type 2 diabetes. The Trust guideline for the management of T2DM in pregnancy is in line with NICE recommendations for diabetes in pregnancy. 4 This project was aimed at women with diagnosed T2DM prior to pregnancy or meeting the criteria for T2DM during pregnancy. The inclusion and exclusion criteria are illustrated in Table 1.
Participant inclusion and exclusion criteria.
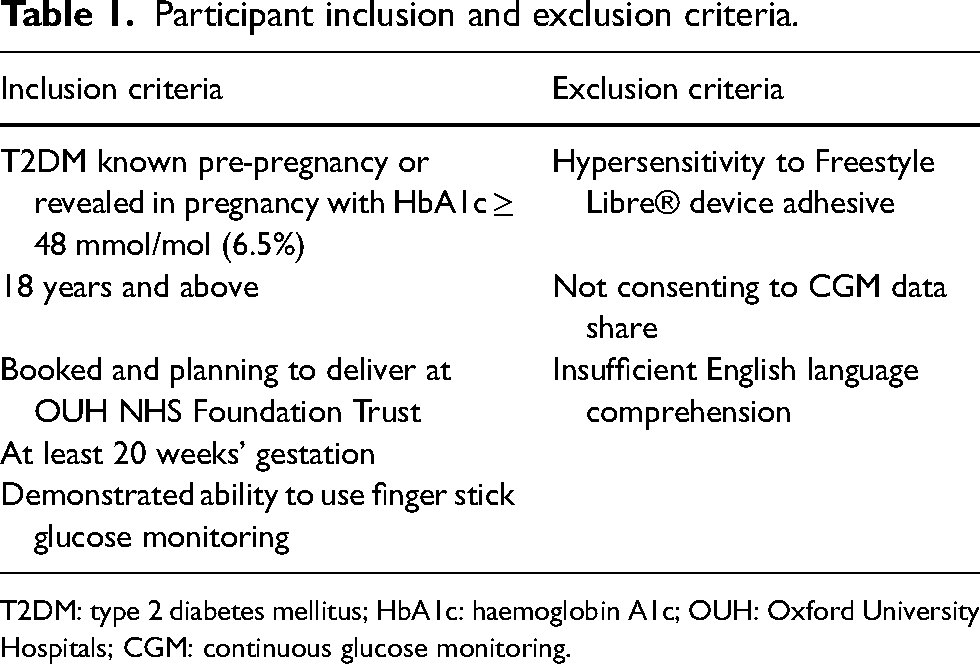
T2DM: type 2 diabetes mellitus; HbA1c: haemoglobin A1c; OUH: Oxford University Hospitals; CGM: continuous glucose monitoring.
The project lead (SB) approached all women meeting the inclusion criteria in the pregnancy and diabetes specialist clinic held at the John Radcliffe Hospital. Participation was voluntary and non-renumerated. If women agreed to participate, they were provided with information related to the Libre device system, as well as the sensors and reader. The majority of women who chose not to take part disliked the thought of having to wear a sensor all day. This was unrelated to ethnicity or whether or not they did not speak English. There was good participation from women who identified as being from different ethnic groups. Prior to enrolment, eligible women were encouraged to use the GDm-HealthTM app on their smartphones to record fasting and postprandial values. Training on how to use the Libre device was provided both face-to-face and virtually, with help from existing educational tools from the manufacturers (https://pro.freestyle.abbott/ie-en/home/scientific-resources-education/patient-education.html).
Participants were asked to perform all glucose testing by isCGM. Results were recorded in one of three ways: (1) by manually entering fasting and 1-hour post-prandial glucose readings into the GDM-Health AppTM, 6 (2) by recording the same values on a paper record, or (3) by sharing data through the Libre View AppTM where time in the recommended pregnancy range (3.5–7.8 mmol/mol) could be assessed. The results were remotely monitored and reviewed up to three times per week by a member of the diabetes clinical team. Participants attended antenatal multidisciplinary clinics every fortnight, with monthly ultrasound scans through the third trimester as per the existing Trust care pathway.
The primary outcomes for this project were feasibility and acceptability. Feasibility was determined by the number of participants who continued to use the device until delivery. Acceptability and satisfaction with the system were assessed through a structured questionnaire completed by participants during pregnancy or within four weeks of delivery: the validated Oxford Maternity Diabetes Treatment Satisfaction Questionnaire (OMDTSQ) was used as the questionnaire. 7 The OMDTSQ comprises 10 questions designed to assess general satisfaction with diabetes care, the acceptability and reliability of the technology, and the perceived relationship with the diabetes care team. Only nine questions were applied to the present study. Participants were asked to score their agreement with statements on a 7-point Likert-type scale, ranging from +6 (strongly agree) to −0 (strongly disagree). The OMDTSQ was plainly worded in English. At the end of the questions, women were encouraged to write free-text responses to provide additional feedback and/or suggestions. 7 The questionnaire was sent to participants electronically, with paper copies available in the clinic if preferred. At the end of the questionnaire, free text responses were captured about any aspects of their glucose monitoring or diabetes care. All questionnaires were anonymised and free text comments were analysed using thematic analysis. Information on individual characteristics and birth outcomes from the hospital electronic patient record (Cerner MillenniumTM).
Glucose control in the third trimester was determined by mean glucose in range on the Libreview App or on the GDM Health App. For those using Libreview, we used the T1DM CGM target of 70% in the pregnancy glucose range (3.5–7.8 mmol/L). For participants recording fasting and one-hour post-prandial interstitial glucose levels, we defined meeting target as not having more than three out-of-range readings per week.
Given the small sample size, descriptive baseline and delivery data are presented only, with no inferential statistics.
Results
Between March 2022 and April 2023, 48 pregnant women with T2DM were managed through our Trust. Of these, 23 women met the entry criteria and agreed to participate in the study, with 20 using the device until delivery (Figure 1). At follow-up, one participant dropped out of the project, and two stopped using isCGM and switched back to finger sticking for self-monitoring. A total of 22 participants answered the qualitative feedback survey between 28 and 36 weeks’ gestation. Whilst 14 women were in a second or subsequent pregnancy with type 2 diabetes, all participants were using the isCGM device for the first time.
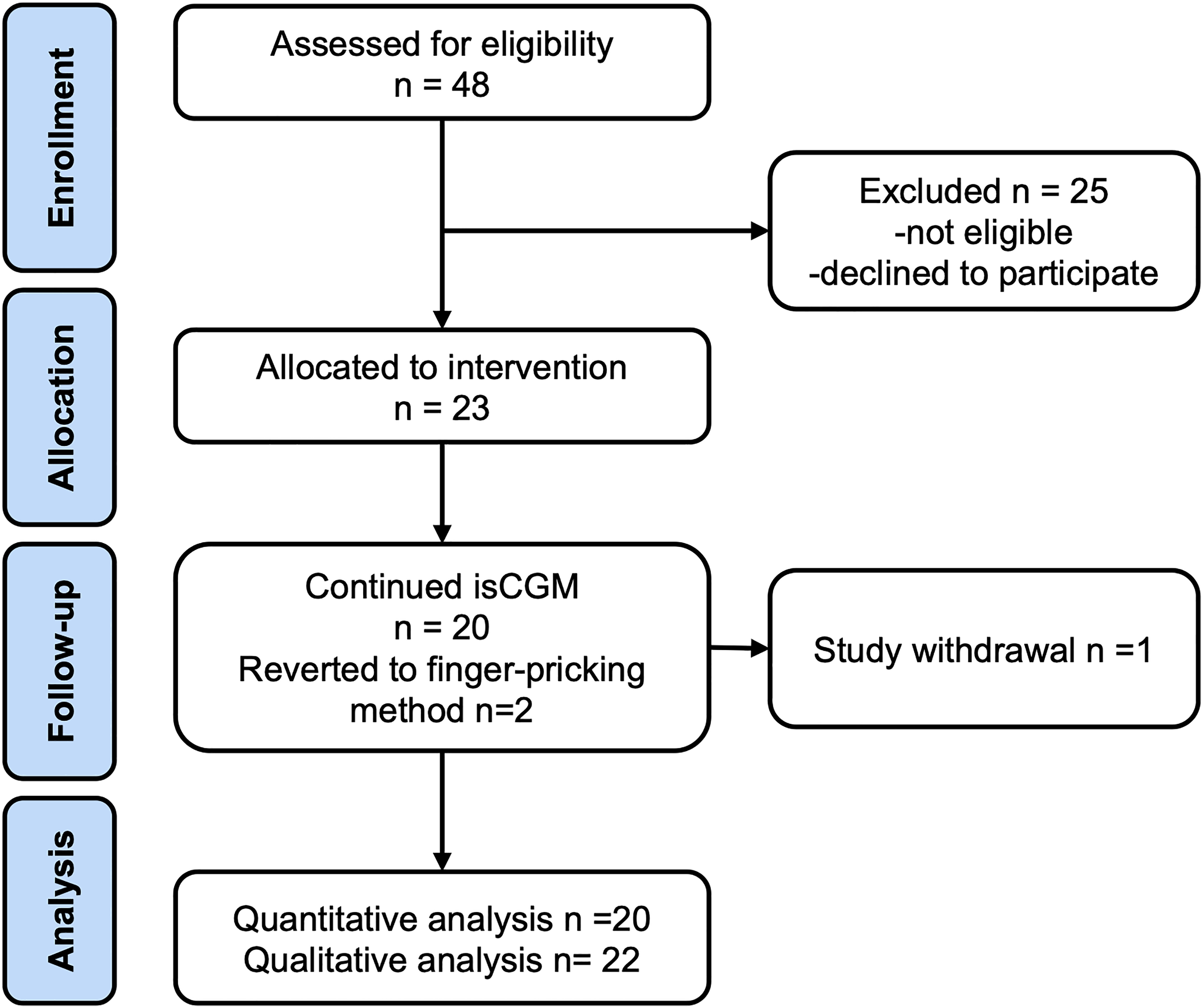
CONSORT flow diagram of patients eligible, recruited, numbers followed-up and included in analysis. Abbreviations: number of participants (n); intermittently scanned continuous glucose monitoring (isCGM).
Table 2 displays the baseline characteristics of participants and their pregnancy outcomes. Most women were overweight or obese, defined as having a body mass index (BMI) of 25–30 and over 30 kg/m2, respectively. The BMI for the entire sample ranged from 24 to 45 kg/m2 with only one participant with BMI less than 25 kg/m2. Almost a third of participants developed a hypertensive complication of pregnancy, and most delivered by caesarean birth. There were no perinatal deaths.
Baseline characteristics of the 23 participants.
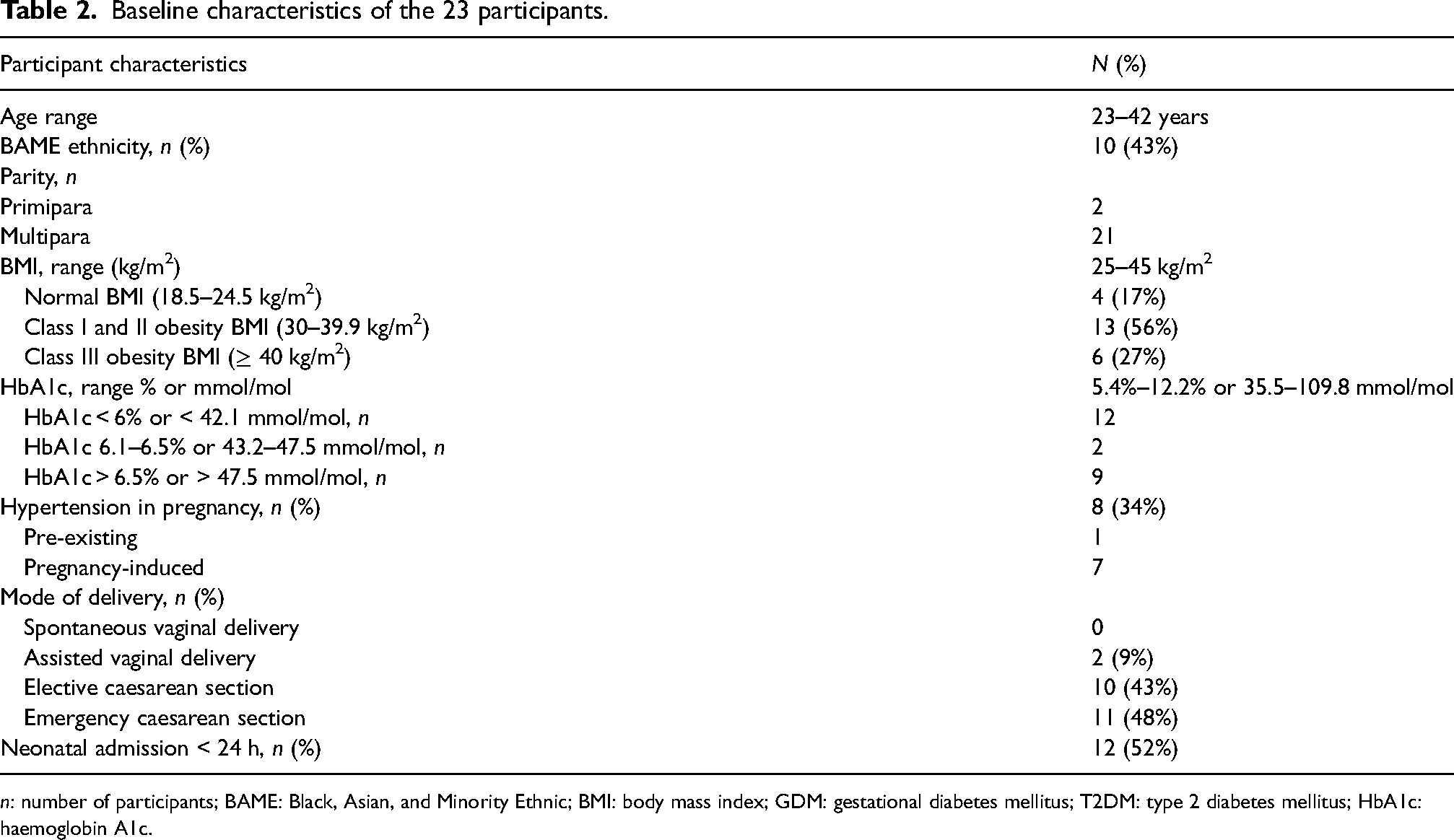
n: number of participants; BAME: Black, Asian, and Minority Ethnic; BMI: body mass index; GDM: gestational diabetes mellitus; T2DM: type 2 diabetes mellitus; HbA1c: haemoglobin A1c.
Satisfaction with Libre 2 CGM monitoring in pregnancy
Table 3 summarizes the qualitative feedback received through the questionnaires. Most participants were very satisfied with their care. Sixteen participants reported they were very satisfied with the convenience of CGM equipment for monitoring blood glucose. Additionally, 15 women found that the equipment was very reliable. There was less agreement over whether the type of monitoring fitted in well with daily activities throughout pregnancy, with around half of participants agreeing with this statement. Of the 14 participants who had experienced a previous pregnancy affected by T2DM, 11 rated their glucose monitoring experience as much better compared to that of previous pregnancies. Most participants expressed that they would be interested in using the CGM device for continuous blood glucose monitoring in future pregnancies, while 19 would recommend the device to friends and/or family also affected by T2DM irrespective of pregnancy status.
Summary of quantitative patient feedback.
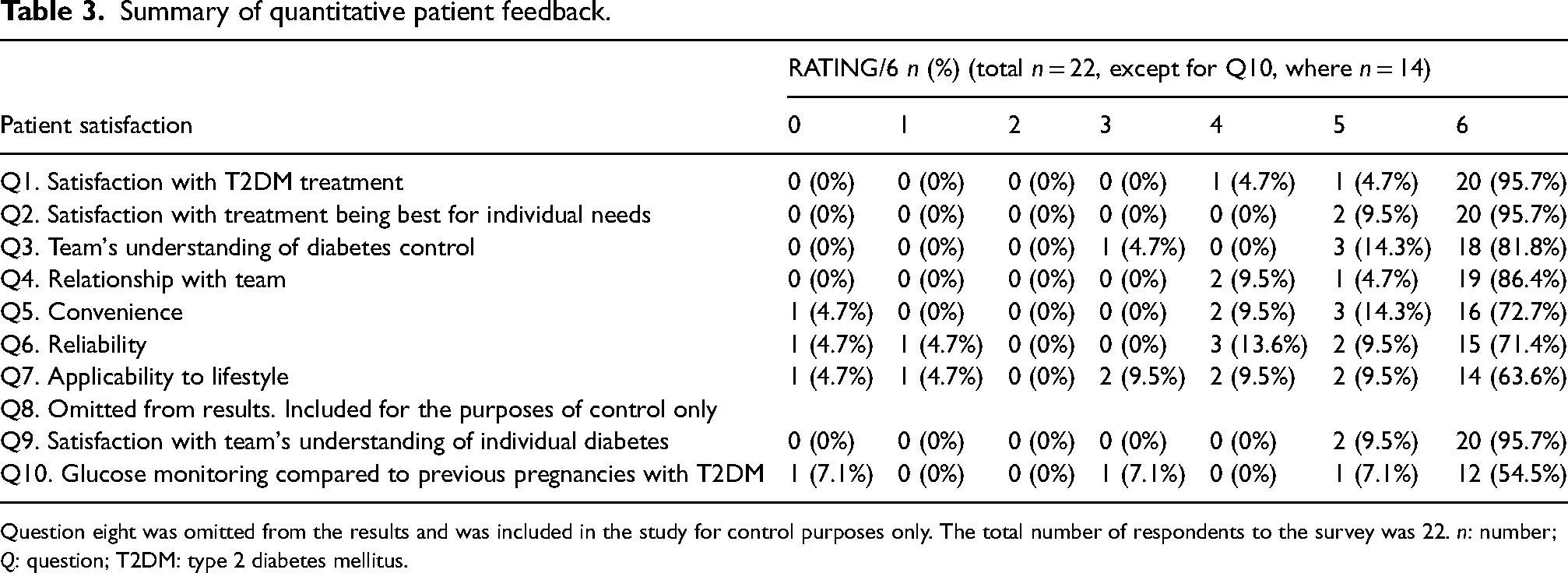
Question eight was omitted from the results and was included in the study for control purposes only. The total number of respondents to the survey was 22. n: number; Q: question; T2DM: type 2 diabetes mellitus.
Satisfaction with the diabetes team
Overall, all participants were satisfied with both the treatment received and their relationship with the diabetes team. The average score for how satisfied patients were with treatment received for their T2DM was 5.6 out of 6 (range: 4–6). Most patients felt that the maternity diabetes team understood individual levels of diabetes control (average score of 5.7 out of 6, range: 3–6) and that the relationship with the maternity diabetes team was positive (average score of 5.8 out of 6, range: 4–6). All patients felt that the maternity diabetes team understood individual needs and concerns (average score of 5.9 out of 6, range: 5–6).
Emergent themes of qualitative open feedback
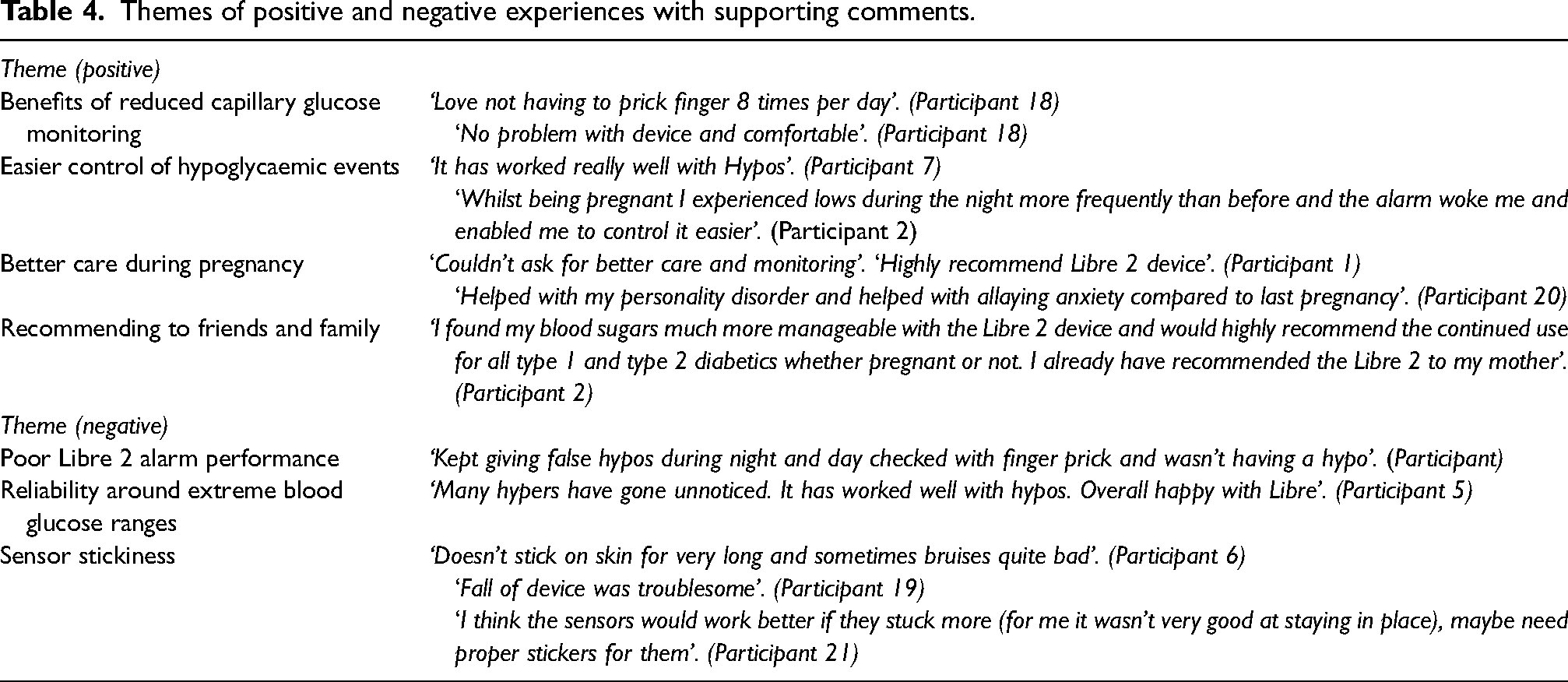
Written comments supported the scores. Four themes were identified around positive experience with the technology (1) benefits of less finger pricking, (2) perceived easier control of hypoglycaemic events, (3) feeling that they had better care during pregnancy, and (4) recommending it for self, family, and friends. The three main areas where challenges were experienced were (1) poor alarm performance, (2) reliability around upper and lower glucose ranges, and (3) sensor stickiness to the skin. The themes are summarized in Table 4.
Themes of positive and negative experiences with supporting comments.
Discussion
We demonstrate the feasibility and acceptability of isCGM among women with T2DM in the second and third trimesters of pregnancy in our population. We note that some women living with obesity reported adhesion problems with the sensors and concerns about device accuracy in the extremes of glucose. Overall, however, the response from participants was extremely positive towards using this technology. We believe this is a first step towards including isCGM as part of clinical care for women with T2DM in pregnancy.
The women participating in the study were representative of our clinic population, with 10 participants (43%) being of Black, Asian, or other minority ethnicity, and 83% being obese. Overall, an acceptable time in the glucose target range was achieved by the majority of women using isCGM, with 16 participants achieving a time in the range of more than 70% in the third trimester. This qualitative study has shown that women with T2DM found isCGM management using the Libreview 2 device system acceptable, suitable, and convenient. Based on the feedback provided, most women felt the technology was more convenient than finger sticking. They also felt well-supported and very satisfied with their care. There were no major barriers to uptake. However, reliability at extreme ranges of glucose and device sensor falling off was a noticed theme. This correlates with issues identified in other published research.8–10 In this study, more than two-thirds of women continued to use the device for glucose monitoring, suggesting high acceptability.
CGM is an established method for comprehensive glucose data and is convenient for the patient. Our study suggests that CGM is acceptable to women with T2DM during pregnancy and feasible in the context of intensive monitoring required in the management of such high-risk pregnancies. However, several questions remain unanswered with regards to CGM use in pregnant patients with T2DM, namely (1) whether CGM is a better technique for women who have entered pregnancy mostly without the ability to even self-monitor their blood glucose, (2) whether CGM is an answer for women who struggle with escalating from no glucose monitoring to the intensive management required in pregnancy to prevent poor outcomes, and (3) whether CGM can improve maternal and fetal outcome in high-risk and unplanned pregnancies.
Strengths and limitations
The strengths of this project are the high completion rate of the questionnaire (95%) and the continuation of participation at follow-up (87%). The OMDSTQ-validated questionnaire demonstrated a good level of participation and feedback. Using only a single tool of a structured questionnaire for the measurement of satisfaction was a limitation, although written comments by participants were highly congruent with their corresponding question scoring. The sample size of the service improvement project was small, hence these encouraging results need confirmation in a larger clinical study. As participants were voluntary and the condition was pre-existing, some women may have been motivated or experienced with the device. However, most women (95%) enrolled were using the CGM for the first time.
Conclusion
The result of this study encourages the progression in researching the role of CGM for the management of T2DM in pregnancy to improve women's experience and glucose monitoring compliance, which is strongly correlated with maternal and fetal outcomes. We propose that future research could expand this project as part of a multicentre study on the use of CGM for T2DM in pregnancy and also explore the correlation between the use of CGM in the management of T2DM in pregnancy and outcomes in a variety of populations. A detailed cost analysis, including the costs of equipment, staff, and infrastructures are essential in strengthening the candidature of CGM as an alternative way to self-monitoring blood glucose in high-risk pregnancies.
Supplemental Material
sj-docx-1-obm-10.1177_1753495X241233030 - Supplemental material for Acceptability of and satisfaction with continuous glucose monitoring in pregnant women with type 2 diabetes mellitus: A service improvement project
Supplemental material, sj-docx-1-obm-10.1177_1753495X241233030 for Acceptability of and satisfaction with continuous glucose monitoring in pregnant women with type 2 diabetes mellitus: A service improvement project by Sridevi Beriwal, Federica Re, Sharon Gibson, Gaya Thanabalasingham, Katharine R. Owen, Ruth Houlden, Anastasios Malakasis and Jane E Hirst in Obstetric Medicine
Supplemental Material
sj-docx-2-obm-10.1177_1753495X241233030 - Supplemental material for Acceptability of and satisfaction with continuous glucose monitoring in pregnant women with type 2 diabetes mellitus: A service improvement project
Supplemental material, sj-docx-2-obm-10.1177_1753495X241233030 for Acceptability of and satisfaction with continuous glucose monitoring in pregnant women with type 2 diabetes mellitus: A service improvement project by Sridevi Beriwal, Federica Re, Sharon Gibson, Gaya Thanabalasingham, Katharine R. Owen, Ruth Houlden, Anastasios Malakasis and Jane E Hirst in Obstetric Medicine
Footnotes
Acknowledgements
The authors would like to thank Charlotte Lang and Aaron Lorente Lozano for their assistance in this research.
Author contribution
JEH and SB conceived the study. SB researched literature and successfully applied for the grant. FR was involved in data analysis and editing. SB wrote the first draft of the manuscript. SG helped with recruitment. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Oxfordshire Health Services Research Committee (OHSRC), part of Oxford Hospitals Charity (registered charity number 1175809, Grant unique cost centre 8413).
Ethical approval
Ethical approval was not sought for the present study because it was a service improvement project approved and registered with clinical governance. This study was completed in accordance with the Helsinki Declaration as revised in 2013.
Informed consent
Written informed consent was obtained from all subjects before the study.
Guarantor
Jane E Hirst (JEH).
Trial registration
Not applicable because it was a service improvement project and not a trial.
Supplemental material
Supplemental material for this article is available online.
Correction: (March 2024):
Update to author’s name: Federica Re
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.