
Abstract
Background
Pregnancies in women on dialysis remain rare but are increasing in number.
Methods
Retrospective observational audit of seven cases from 1977 to 2022 of all women who conceived prior to dialysis or conceived whilst on dialysis.
Results
Of a total of seven women, three were referred from regional centres in Australia, between the 6 and 20 weeks of gestation, generally without any opportunity for pre-conception counselling. Five were managed with intensive haemodialysis aiming for six sessions per week; one patient continued peritoneal dialysis until birth by caesarean section. Five women out of seven had live births, two of which were conceived whilst on dialysis. Four were delivered prematurely between 27 and 31 weeks of gestation, and one at term via spontaneous vaginal delivery.
Conclusions
Outcomes for women with pregnancies on dialysis benefit from intensive dialysis management however the practical implementation remains challenging. Our cases highlight the diversity of experience in our centre across two decades.
Introduction
Pregnancies in women with kidney failure on dialysis are clinically challenging. Compared with the general population, there is a greater risk of maternal mortality, uncontrolled hypertension and preeclampsia including HELLP syndrome (haemolysis, elevated liver enzymes and low platelets), and greater risks to the fetus including miscarriage, small for gestational age (SGA), polyhydramnios, prematurity, neonatal intensive care admissions and intrauterine fetal and neonatal death. 1 Increased capability to provide intensive dialysis to pregnant women over the past 30 years has allowed greater success and safety, improving outcomes for both mother and baby.
The rate of conception whilst on chronic dialysis and subsequent live birth rates are increasing. The Australian and New Zealand Dialysis and Transplant (ANZDATA) Registry reported 11 pregnancies between 2018 and 2020, 85% resulting in a live birth, 2 compared with data from 1966 to 2008 where the live birth rate was 79%. 3 The literature describes superior pregnancy outcomes of women who conceive before beginning dialysis (CBD), compared with those who had conceived whilst on dialysis (COD) who may be less likely to have significant residual kidney function and therefore the greater requirement for haemodialysis intensity to reach serum urea targets. 4
We present cases of pregnancy in women on dialysis from a tertiary centre highlighting the time of conception, dialysis management and fetal outcomes and compare our management with the available literature. 5
Methods
We reviewed cases at the Royal Brisbane and Women's Hospital (RBWH), a metropolitan tertiary hospital with co-located obstetric, obstetric medicine, maternal and fetal medicine and kidney services.
All pregnant women on kidney replacement therapy between January 1977 (commencement date of ANZDATA Registry) and June 2022 at the RBWH were included. Data was collected from ANZDATA and medical records including age, cause of kidney failure, comorbidities, dialysis duration and modality, and obstetric and perinatal data. This study was approved by the RBWH Human Research Ethics Committee (HREC) (LNR/2021/QRBW/74239).
Results
Seven cases were identified via ANZDATA (see Table 1) and all were included in this review.
Summary – characteristics of women who received dialysis whilst pregnant.

KF: kidney failure; SLE: systemic lupus erythematosus; HUS: haemolytic uraemic syndrome; GN: glomerulonephritis; FSGS: focal segmental glomerulosclerosis; Anti-GBM: anti-glomerular basement membrane; COD: conception on dialysis; CBD: conception before dialysis; HD: haemodialysis; PD: peritoneal dialysis.
Case 1 (2006)
A 28-year-old female with a background of focal sclerosing glomerulonephritis, presented at 12 weeks’ gestation. She had been on haemodialysis for 2 years prior to the birth. Serum urea levels at the time of conception varied but were as high as 44 mmol/L. Despite a dialysis duration of 4 h, 3 times per week continuing she had a spontaneous miscarriage at 14 weeks’ gestation. The cause of fetal death was not apparent from the post-mortem examination.
Case 2 (2007)
A 25-year-old female from a regional area with biopsy-proven fibrillary glomerulopathy had a history of nephrotic range proteinuria (9.9 g/24 h), hypoalbuminemia (serum albumin 20 g/L) and baseline urea 6.0–8.0 mmol/L and creatinine 77–120 µmol/L. Treatment with cyclophosphamide and prednisolone had minimal response. One year later she was referred to our unit at 20 weeks’ gestation, with > 20 g protein/24 h urine collection and serum albumin < 15 g/L. No pre-conception counselling was documented. At 24 weeks’ gestation, her serum urea was consistently > 10 mmol/L and she commenced haemodialysis via a tunnelled central venous catheter (CVC) at 4–5 h 6 days per week, aiming to keep serum urea < 10 mmol/L (average was 9.1 mmol/L). She had a reasonable residual urine output of 1.8 L/24 h. She had a live delivery via lower uterine segment caesarean section (LUSCS) at 30 + 4 weeks’ gestation for intrauterine growth restriction (IUGR); birth weight 1172 g. She remained dialysis-dependent from this point and was subsequently listed for a kidney transplant which she received 5 years later.
Case 3 (2009)
A 19-year-old female with a background of systemic lupus erythematosus (SLE) with kidney involvement (biopsy proven Class IV, 2 years prior to pregnancy), complicated by suboptimal compliance to medications and progression to kidney failure, presented at 6 weeks’ gestation with serum urea 12.5 mmol/L and creatinine 253 µmol/L. Her C3 was low at 0.58 g/L, C4 normal range and dsDNA high at 26 IU/mL. She had nephrotic-range proteinuria (urinary protein creatinine ratio 300–500 g/mol creatinine) and developed severe anaemia with haemoglobin 50–60 g/L (from baseline of ∼110 g/L pre-conception) with normal platelets and no signs of haemolysis (blood film negative for fragments and bilirubin normal). At conception, she had ∼2 L residual urine output. Serum urea climbed to 16–19 mmol/L and creatinine 250–300 µmol/L in the following 2 weeks and she was commenced on intensive haemodialysis via tunnelled CVC at 8 weeks’ gestation, 4–5 h 6 days per week to target serum urea < 15 mmol/L. An average pre-dialysis reading of 13.6 mmol/L was achieved. Amniocentesis was performed at 16 weeks (negative for aneuploidy). She had a live delivery via LUSCS at 29 weeks’ gestation – expedited due to IUGR (reduced growth velocity from 11% to < 3% centile of estimated fetal weight) and maternal hypertension. The birth weight was 906 g and the baby was admitted to the neonatal intensive care unit (NICU). She remained dialysis-dependent following the pregnancy.
Case 4 (2010)
A 29-year-old Indigenous Australian female from a regional area developed kidney failure at the age of 27 years secondary to SLE presenting with nephrotic syndrome, arthralgia, episcleritis, seizures and biopsy-proven WHO Class IIb lupus nephritis. She had been treated with cyclophosphamide but progressed to require peritoneal dialysis. Following this she had two medical terminations of pregnancy (< 15 weeks’ gestation). Anticardiolipin antibodies were low positive on both occasions (10 and 6 µ/mL), and ENA (anti-RNP) positive. She had started workup for kidney transplantation (not yet listed) and had attended the obstetric medicine clinic for pre-conception counselling where the high-risk nature of future pregnancies was discussed. Options for contraception were discussed but no documentation that any was commenced.
She was referred to our unit at 9 weeks’ gestation, unwell with gastrointestinal upset and skin abscesses. Mycophenolate was ceased, prednisone increased from 5 to 20 mg and she commenced enoxaparin 20 mg subcutaneously daily whilst continuing hydroxychloroquine. Her residual urine output was ∼500 mL/24 h at this time and dialysis parameters reflected a Kt/V of 2.57 and creatinine clearance of 113.87 L/week/1.73 m2 on a high transport membrane.
Laboratory investigations showed a low haemoglobin of 83 g/L, normal platelet count of 247 × 109/L, low complements (C3 0.67 and C4 0.08 g/L), positive anti-double-stranded DNA antibody (28 IU/mL), positive direct Coombs’ test and lupus anticoagulant. She had low haptoglobin 0.19 g/L but normal reticulocyte count, lactose dehydrogenase and bilirubin. Given the activity of her lupus, she received counselling and made an informed decision to proceed with the pregnancy. Her dialysis regimen was altered to avoid postural dizziness, and excessive ultrafiltration and target a blood urea level of < 10 mmol/L (see Supplemental Material). At 20 weeks’ gestation, this was switched from automated overnight peritoneal dialysis (APD) to continuous ambulatory peritoneal dialysis (CAPD) to allow for a better varxjkiance of her prescription. Her blood pressure (BP) averaged 115–130/90 mm Hg. Subcutaneous erythropoietin stimulating agent (ESA) and supplementary iron infusion was titrated according to the haemoglobin within our guidelines and she avoided blood transfusion.
Chorionic villus biopsy was negative for aneuploidy. A fetal wellbeing scan at 24 weeks’ showed normal Dopplers but measurements revealed SGA. At 31 weeks’ gestation, she developed preeclampsia with BP of 180/110 mm Hg, headache, and epigastric pain. A 909 g baby was delivered by emergency transperitoneal lower segment caesarean section with Apgar scores of 7 and 9 at 1 and 5 min, respectively. The baby was admitted to NICU requiring supplemental oxygen. As the peritoneum was breached she was started on haemodialysis via CVC at day 2 postpartum. She was discharged on day 5 postpartum remaining locally until the baby's discharge and continued haemodialysis until day 20. She retained her residual urine output and was able to restart APD.
Case 5 (2011)
A 17-year-old female presented with general malaise, anaemia, and oliguria at 15 weeks’ gestation. Glomerulonephritis screen was significant for an anti-GBM titre of 223 AU/mL. She proceeded to a kidney biopsy which confirmed Goodpasture's disease. She was commenced on daily haemodialysis. Serum urea at presentation was 26.2 mmol/L, and though the average over her treatment course was ∼ 15 mmol/L it ranged as high as 25 mmol/L. She also received intravenous immunoglobulin, methylprednisolone and plasma exchange. Unfortunately, she progressed to develop haemoptysis and an oxygen requirement whereby chest imaging demonstrated bilateral pulmonary haemorrhage. This was complicated by the development of pulmonary hypertension (60 mm Hg) and respiratory syncytial virus infection. She was counselled extensively regarding the gravity of her condition. Given the life-threatening condition, with consent and discussion regarding the risks to the fetus, she commenced intravenous cyclophosphamide. The growth scan at 20 weeks’ was reassuring with an estimated fetal weight of 315 g (17%) however showed a short, funnelled cervix. She went on to have a stillbirth at 22 weeks. Placental histology revealed evidence of ascending inflammation indicative of chorioamnionitis. No fetal autopsy was performed as per the woman's wish. Her disease reached remission in the months following however she remained dialysis dependent.
Case 6 (2019)
A 34-year-old Indigenous Australian woman who had four previous spontaneous miscarriages (three at < 15 weeks’ and one at 32 weeks’ gestation), was referred from a regional hospital to our centre at 9 weeks of gestation. She had a background of kidney failure secondary to biopsy-proven diabetic nephropathy, receiving haemodialysis for 2 years prior via an arteriovenous fistula, and was not yet waitlisted for transplantation. She was anuric with significant interdialytic weight gains of 2–3 kg and urea reduction ratios (URRs) indicative of suboptimal clearances in the year prior to conception (43–45), noting frequent missed sessions. Her type 2 diabetes mellitus was diagnosed at age 13 years (negative autoantibodies) requiring insulin therapy, with historically poor control and severe non-proliferative diabetic retinopathy. HbA1c at the time of conception was 6.4% (in the setting of anaemia). She was given a continuous glucose monitor for more intensive monitoring. BP control preconception was reasonable (systolic BP between 130–140 mm Hg post dialysis). Other history included hypertension, asthma, current cigarette smoking and chronic, mild pancytopenia of uncertain cause.
Her haemodialysis frequency was increased from 3 to 6 days per week for 5 h, aiming for a pre-dialysis serum urea of ≤15 mmol/L (blood monitored weekly), achieved within 6 weeks. Anaemia in pregnancy was managed with ESA and iron given intravenously on dialysis was up titrated. She received one unit of packed red cells.
Dialysis was complicated by interdialytic weight gains of 2–3 kg in each 24 h period assessed with a weekly clinical review of ideal body weight and hypertension managed with fluid restriction, ultrafiltration (1–3 L per dialysis session), oral methyldopa and nifedipine aiming for a post-dialysis BP < 140/90 mm Hg. The required 2–3 L ultrafiltration was equivalent to 5%–7.5% of the patient's ideal body weight and contributed to frequent intradialytic hypotension, (with systolic BPs often falling below 100 mm Hg), concerning for compromise of placental blood supply. At 20 weeks’ growth scans demonstrated reassuring growth but an effaced cervix and concerns for an incarcerated uterus – given anuria there was absence of any earlier warning sign. This was confirmed on magnetic resonance imaging (MRI) and restituted with insertion of pessary. Weekly fetal heart rate checks with Doppler ultrasound post dialysis were performed. Her pre-dialysis serum urea at this time was 12–13 mmol/L. At 23 weeks her routine fetal wellbeing scan showed a reduction in growth velocity, SGA and impaired placental blood flow but normal amniotic fluid volumes. Doppler monitoring was increased to twice weekly.
At 27 weeks and 3 days, scans demonstrated absent end diastolic flow in the umbilical artery and reduced cerebroplacental ratio. Steroid loading was given to assist with fetal lung maturity and arrangements were made for emergent LSCS. A live female baby was delivered with a birthweight of 701 g. Immediately, postoperatively care was complicated by post-operative maternal cardiac arrest (pulseless electrical activity and unclear cause) requiring intubation and 2 min of cardiopulmonary resuscitation. The baby was transferred to the neonatal intensive care (NICU) requiring invasive ventilation. The patient was extubated in the following days and the baby transitioned to room air in the coming weeks. The patient and her baby returned to her regional hometown after some months and her usual dialysis regimen post-delivery.
Case 7 (2021)
A 19-year-old female with Senior Loken syndrome presented at her antenatal booking visit at 15 weeks’ gestation with a creatinine of 416 µmol/L and urea of 24.8 mmol/L. She had no previous medical history. She commenced haemodialysis via tunnelled CVC consisting of 5 h, 6 times weekly aiming for serum urea < 12.5 µmol/L. She had difficulty maintaining regular attendance to this intensive regime. Her pre-dialysis serum urea averaged 15–16 mmol/L. Her residual urine output was documented as reasonable (no formal 24-hour collection documented). Phosphate supplementation (fleet) was added to the dialysate. Anaemia management required frequent escalations of intravenous ESA, iron and packed red cells with haemodialysis to maintain a haemoglobin > 80 g/L. Morphology and growth scans (second weekly) were reassuring. Blood pressures on dialysis were occasionally as low as ∼90/70 mm Hg with no documented hypertension. She had a planned induction of labour resulting in the vaginal delivery of a healthy live baby at 37.7 weeks, with a birth weight of 3416 g and they did not require special care. The patient remained on haemodialysis postpartum.
Discussion
Our case series highlights the challenges of management for women who are pregnant with kidney failure and reinforces the need for individualised care. We compared our practice with that recommended by the clinical practice guideline on pregnancy and renal disease published in 2019 5 and our local guidelines (see Supplemental Material), derived from expert consensus and modified based on international guidelines.
Dialysis parameters and residual kidney function
We clinically assessed the women and adjusted the ultrafiltration rate weekly, titrated to the patient's tolerance aiming for a post-dialysis BP of < 140/90 mm Hg whilst avoiding hypotension. Biochemistry was assessed on a weekly basis and dialysis prescriptions were adjusted accordingly, aiming for a serum urea of < 12.5 mmol/L. Concern regarding the fetotoxicity of urea has led to a focus on specific targets, with the literature suggesting an association with improved fetal outcomes when dialysis is initiated when serum urea is 17–20 mmol/L, and maintained such that midweek serum urea is < 12.5 mmol/L. 6 We note that targets appear to have changed from < 10 to <12.5 mmol/L over the decades, as more robust data has been published.
It has been empirically shown in a Brazilian cohort study that a blood urea nitrogen (BUN) of 12.5 mmol/L or less significantly decreased the risk of perinatal death or extreme prematurity. 6 This correlates with a 2016 systematic review and other published literature, suggesting a longer duration of haemodialysis is preventive of preterm delivery (up to 36 h per week).7–9 The mean gestational age for live births occurring during HD in the literature is ∼ 34 weeks with a positive correlation with the duration of HD. 10 The average mean gestation for our cases is below this (31 weeks), though there was significant variation (see Table 1).
There is also an argument against longer dialysis in the literature particularly for women with residual urine output. Some studies have demonstrated that blood urea levels did not correlate with outcomes such as prematurity and perinatal death, 11 and that long intensive dialysis could, in fact, increase the rate of cervical shortening and risk of premature birth.12–14 Other publications show the evidence is less clear.6,15 For all except one of our cases of live birth the mothers had a residual urine output of between 500 mL and 2 L, which likely contributed to the appropriateness of shorter dialysis regimens where still able to achieve the target serum urea. Ultimately, more evidence is needed to assist with tailoring the dialysis regime to the individual woman and this is an area of expanding research.
COD versus CBD
An Australian study showed CBD to have superior live birth rates compared to COD and postulate residual renal function is likely to play a major role.2,6 Of the four patients who had CBD, three had a live birth. The patient who had a stillbirth (Case 7) had an unavoidable need for life-saving immunosuppressive treatment which unfortunately challenged the ability to maintain serum urea targets with daily dialysis, and likely directly increased the risk of infective complications including chorioamnionitis. Our review builds upon the latest systematic review and meta-analysis on the topic of COD. 7 There have been six case reports in the literature from 2016 to 202116–21 and one case series 22 (see Table 2). Comparatively, our two COD cases’ gestational age at birth was lower (31 and 27 weeks vs. an average of 33.6 weeks). Cases 3 and 4 have already been published in the literature. 23
Case reports since 2016 of conception on dialysis.
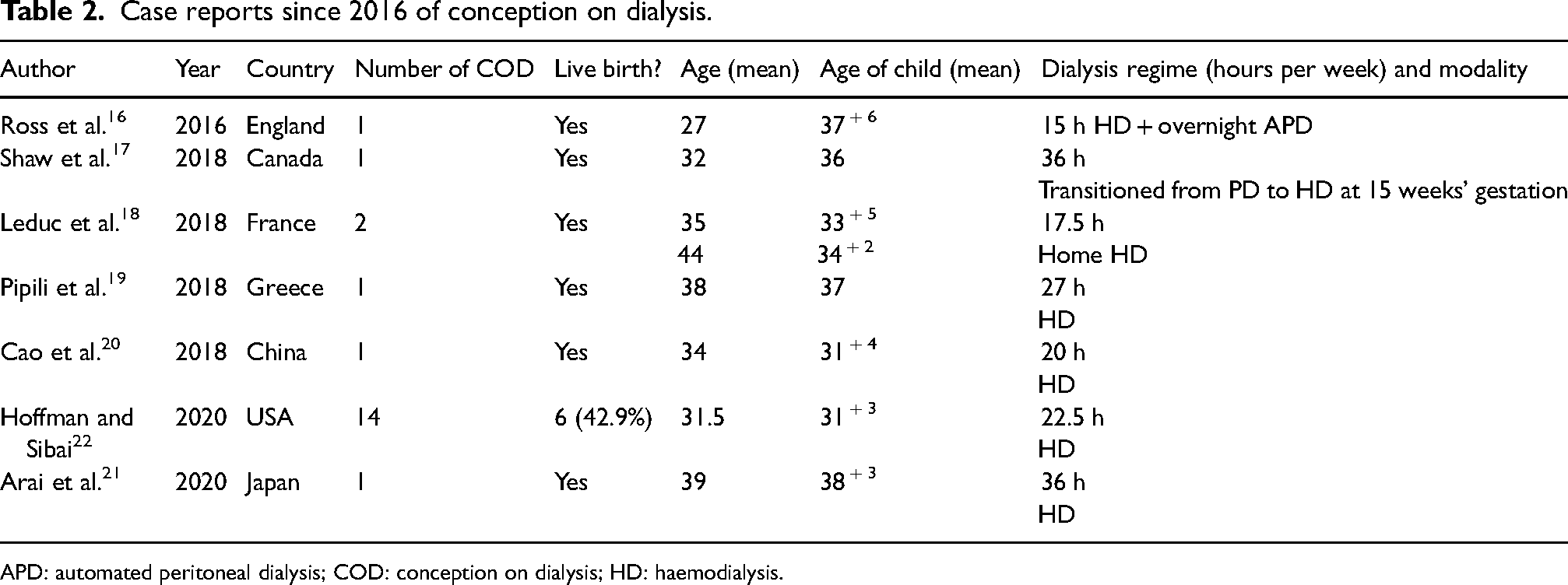
APD: automated peritoneal dialysis; COD: conception on dialysis; HD: haemodialysis.
Modality choices
Case 3 is an example of the continuation of PD throughout pregnancy up until delivery. There is a small amount of data suggesting outcomes are similar regardless of modality.2,24 The outcomes of pregnancy and guidelines for the management of PD remain limited. Despite the suggestion to change women from peritoneal dialysis to haemodialysis in literature, there will be circumstances such as this (patient preference or locality, resources limiting options) whereby it may be necessary to continue with PD until no longer possible.
Accessing care
Distance from and timely access to specialty care is a significant challenge for women living in regional Australia. Four of the cases we present were referred from regional centres where access to specialist obstetric medicine for pre-conception counselling requires either telehealth or significant travel distance, and staying far from support networks is an emotionally onerous and psychologically challenging undertaking is immense. Physical and psychological preparation for a high-risk pregnancy is likely to significantly benefit the woman and baby. There is significant financial cost involved in these situations, especially where ongoing specialist care is required postpartum. Successful pregnancies in women on dialysis heavily rely on thorough counselling regarding these factors. The reality of completing this preconception is challenging, particularly accounting for misconceptions that ESKD causes infertility and women on dialysis who may not be using contraception. A focus on the provision of pre-conception counselling is likely to have the most impact on successful management during pregnancy in the future.
Conclusion
The challenge of providing guideline-based care for women who are pregnant on dialysis is illustrated by the complexities of the cases described here and highlights the need for increased vigilance and multidisciplinary effort required to optimise outcomes for the mother and child.
Supplemental Material
sj-docx-1-obm-10.1177_1753495X241254243 - Supplemental material for Pregnancy in women on dialysis – A case series – Challenges in achieving evidence-based care
Supplemental material, sj-docx-1-obm-10.1177_1753495X241254243 for Pregnancy in women on dialysis – A case series – Challenges in achieving evidence-based care by Laura De Souza, Duc Pham, Ann-Maree Craven, Renuka Sekar, Shilpanjali Jesudason, Sharad Ratanjee, Wallace Walker and Dwarakanathan Ranganathan in Obstetric Medicine
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Royal Brisbane and Women's Hospital HREC (LNR/2021/QRBW/74239).
Informed consent
Written informed consent was not obtained because of the nature of this clinical audit as approved by the Human Research Ethics Committee (HREC).
Guarantor
Not applicable.
Contributorship
All authors contributed to the development, reviewed and edited the manuscript and approved the final version of the manuscript.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.