
Abstract
Objective
This study evaluates obstacles peripartum patients with additional medical needs face and services that would be helpful in obtaining this care.
Study Design
A survey was administered to 226 patients at a clinic specializing in internal medicine care for peripartum patients. Data was analyzed through descriptive statistics and linear regression.
Results
The three most reported barriers that interfered with attending medical appointments included the inability to leave work (41%), being too busy (33%), and lack of childcare (29%). Hispanic and Black patients reported more barriers to care as compared to White patients. The three most reported interventions that would be helpful in attending appointments were more virtual appointment options (38%), increased insurance coverage (31%), and provision of childcare (30%). Interventions were widely rated as helpful regardless of barriers faced and race reported.
Conclusions
Targeted interventions are needed to enhance access to peripartum care, especially for patients from marginalized racial and ethnic populations.
Introduction
Peripartum patients have unique health needs which may necessitate frequent medical appointments. Access and engagement in peripartum care have been associated with improved maternal and fetal outcomes, particularly for patients with underlying medical conditions.1–7 However, many women, particularly women from marginalized racial and ethnic populations and women from lower socioeconomic backgrounds, are less likely to receive prenatal and postpartum care. This may contribute to the disparities seen in maternal morbidity and mortality.8–10
Prior research examining the common barriers patients face when attempting to engage in peripartum care has identified some common obstacles including transportation, cost, and childcare. 11 However, existing studies have primarily surveyed the general peripartum population, not patients who have medical needs that may necessitate increased appointments. Additionally, few studies have examined which interventions patients believe would be most helpful to assist in attending their medical appointments. While it has been well established that women from marginalized racial and ethnic populations, particularly women identifying as Black and/or Hispanic, face decreased access to peripartum care, more research is needed to determine how barriers to care differ by race and ethnicity.12,13
The primary aim of this study was to assess reported barriers to care and the perceived helpfulness of interventions among women referred to receive specialized obstetric medicine care due to additional peripartum health needs. The secondary aim was to determine if racial or ethnic disparities existed in reported barriers and the perceived helpfulness of interventions.
Methods
Study setting
An anonymous survey was administered to 226 patients at a Rhode Island internal medicine clinic serving peripartum patients who require specialized care during their pregnancy. The survey was available in English and Spanish as well as in paper form and online using a QR code. Surveys were administered from March to October 2023.
Study design
Survey questions assessed the following: demographic data (ethnic identity, insurance status, zip code), pregnancy data (weeks pregnant, first pregnancy), obstacles to attending medical appointments (lack of childcare, lack of transportation, unable to afford cost, unable to get out of work, lack of language assistance, lack of insurance coverage, lack of technology for virtual appointments, too busy with other things), and helpfulness of interventions in improving attendance of medical appointments (childcare provided, transportation provided, fee waivers provided, increased insurance coverage, virtual appointment options, simpler follow-up scheduling). Survey barriers and interventions were informed by existing literature.10–12,14–19
Survey questions were listed in multiple-choice and 5-point Likert scale formats. See the supplemental file for a complete list of survey questions. A Likert scale was used as it provides granularity, ensures an accurate and representative understanding of responses, and is commonly used to understand the attitudes and perceptions of individuals.20,21 A 5-point scale was used in particular because it allowed for a neutral response option and has been shown to have high reliability, validity, and discriminating power.20,21
Quality improvement staff and clinic providers guided the development of survey questions ensuring the use of language appropriate for a sixth-grade reading level, as recommended by the American Medical Association and National Institute of Health, 22 to support comprehension by all respondents. Quality improvement staff were trained, certified, and worked as part of the Brown University Office of Research Integrity “to educate and assist the Brown research community in the conduct of research that is compliant with applicable federal regulations and institutional policies.” 23 Clinic providers were attending medical physicians who completed obstetric and consultative medicine fellowships and were associate professors of medicine at Brown Medical School. Their expertise in obstetric medicine, years of medical practice in the study clinic, and extensive knowledge of the study patient population helped guide survey development.
The survey underwent a four-week testing phase before being officially deployed for data collection. Adjustments to question phrasing and the addition of the zip code question were made based on patient and provider feedback during this period.
Recruitment
Medical assistants at the clinic distributed paper surveys that also contained a QR code leading to a virtual survey option for all pregnant and peripartum patients coming into the clinic for an appointment.
Recruitment inclusion criteria were patients attending in-person appointments at the clinic who agreed to complete either a paper or virtual survey. Recruitment exclusion criteria were individuals who were not attending in-person or virtual appointments at said clinic, those who declined completing the survey, and those who did not comprehend English or Spanish. Patients were not permitted to complete the survey more than once. Medical assistants distributing the surveys ensured this by asking patients if they had previously completed the survey before providing it to them.
Data collection and analysis
All survey data was anonymous. Patient-reported zip code was used to collect data on social determinants of health domains, including average household size, percentage of households with no internet access, median household income, percentage of the population with a bachelor's degree, percentage of housing units with no vehicle available, and percentage of the population with any private health insurance. This data was collected from the publicly available U.S. Census Bureau's American Community Survey 2022 data profile. 24
Data was compiled into a password-protected Excel spreadsheet only accessible to project investigators. Data was analyzed using descriptive statistics and linear regression using STATA 17 with an a priori significance level of <.05.
Results
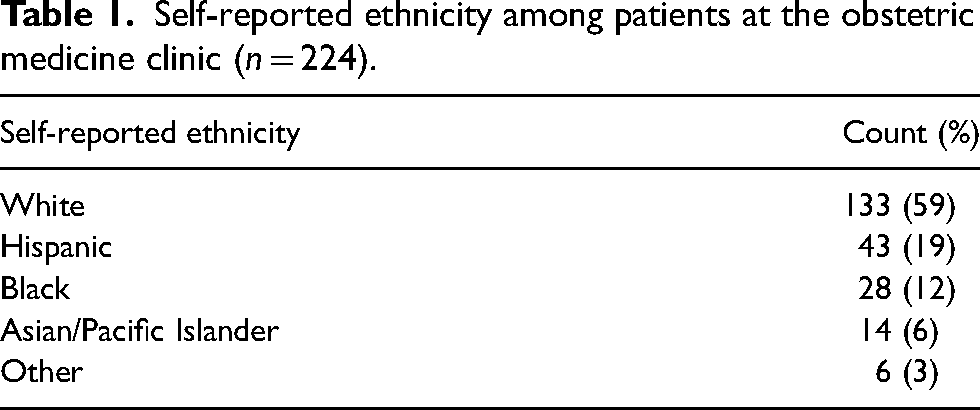
In terms of demographic findings, the study population was identified as 59% White, 19% Hispanic, 12% Black, 6% Asian or Pacific Islander, and 3% other ethnicity (Table 1). All respondents were insured. 50% of respondents were new patients and the other 50% were established patients.
Self-reported ethnicity among patients at the obstetric medicine clinic (n = 224).
Pregnancy data revealed that 30% of respondents were postpartum and not currently pregnant, 19% were in their first trimester, 31% were in their second trimester, and 21% were in their third trimester. Additionally, among those who reported being pregnant, 36% specified it was their first pregnancy.
The three most reported barriers that interfered with attending medical appointments to at least some degree included the inability to leave work (41%), being too busy (33%), and lack of childcare (29%) (Figure 1). On average, 18% of total respondents reported barriers to attending medical appointments (15% of White women, 33% of Hispanic women, 20% of Black women, and 14% of Asian/Pacific Islander women). After adjusting for pregnancy status, as compared to White women, Hispanic and Black women were significantly more likely to rate lack of childcare (p = .02, p = .02) and being too busy (p = .01, p = .01) as barriers to attending medical appointments (Table 2). Additionally, Hispanic women were also significantly more likely to rate lack of transportation (p = .002), inability to afford the cost (p = .01), lack of language assistance (p = .01), lack of insurance coverage (p = .02), and lack of technology for virtual appointments (p = .001) as barriers to attending medical appointments (Table 2).

Barriers to attending medical appointments according to patients at the obstetric medicine clinic (n = 226).
Analysis of associations between barriers to attending medical appointments and self-reported ethnicity with adjustment for pregnancy status in patients at the obstetric medicine clinic.

Note: Linear regression was used to assess associations between barriers to attending medical appointments and self-reported ethnicity, with adjustment performed for pregnancy status, among patients at the clinic.
Zip codes with a greater average household size, a greater percentage of households without internet access, and a greater percentage of housing units without a vehicle reported multiple significantly increased barriers to attending medical appointments. Conversely, zip codes with a higher median household income, a greater percentage of the population with a bachelor's degree, and a greater percentage of the population with any private health insurance reported significantly fewer barriers to attending medical appointments. A detailed summary of these results can be found in Supplemental Table 1.
The three most reported interventions that respondents felt would be helpful or very helpful in attending appointments were more virtual appointment options (38%), increased insurance coverage (31%), and provision of childcare (30%) (Figure 2). After adjusting for pregnancy status, as compared to White women, Hispanic and Asian/Pacific Islander women were significantly more likely to rate provision of transportation (p = .00, p = .03) and simpler follow-up scheduling (p = .05, p = .004) as helpful in attending medical appointments (Table 3). Women identifying as Asian/Pacific Islander were also significantly more likely to rate the provision of fee waivers (p = .03), increased insurance coverage (p = .03), and virtual appointment options (p = .00) as helpful interventions (Table 3). However, these findings should be interpreted cautiously due to the limited sample size of women identifying as Asian/Pacific Islander in this study.
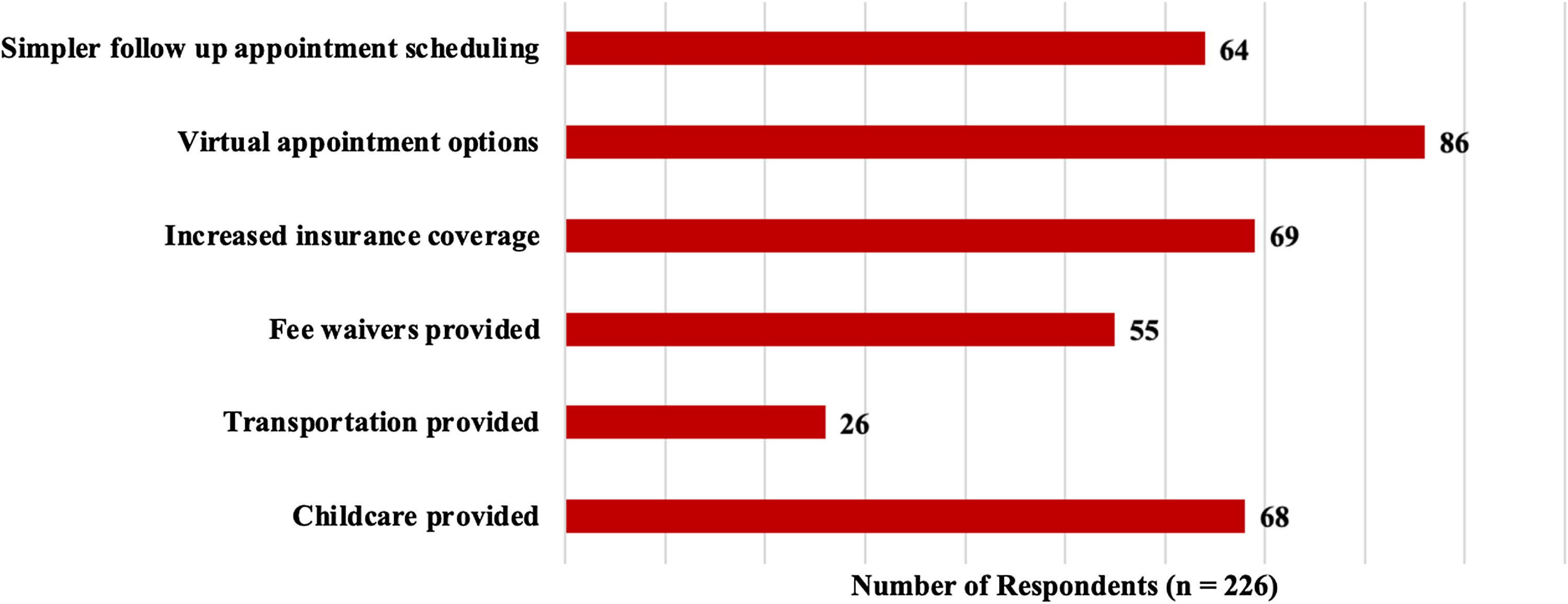
Perceived helpfulness of interventions in attending medical appointments according to patients at the obstetric medicine clinic (n = 226).
Analysis of associations between perceived helpfulness of interventions in attending medical appointments and self-reported ethnicity with adjustment for pregnancy status in patients at the obstetric medicine clinic.

Note: Linear regression was used to assess for associations of perceived helpfulness of interventions in attending medical appointments and self-reported ethnicity, with adjustment performed for pregnancy status, in patients at the clinic.
Those who reside in zip codes with a greater median household income, a greater percentage of housing units without a vehicle, and a greater percentage of the population with any private health insurance were all significantly less likely to report certain interventions as helpful in attending medical appointments. A detailed summary of these results can be found in Supplemental Table 2.
Discussion
In this study, 226 participants who attended at least one medical appointment at an internal medicine clinic serving peripartum patients requiring additional specialized medical care in Providence, RI, were surveyed regarding barriers to care and perceived helpfulness of interventions. Participants reported significant barriers to accessing care, most commonly inability to leave work, being too busy, and lack of access to childcare (Table 3).
While prior studies have also demonstrated that difficulty in obtaining leave from work can hinder access to peripartum care, it has rarely been reported as the predominant reason for the inability to engage in medical care.11,12,14–16 Our findings suggest that lack of parental leave or flexible work arrangements for pregnant patients poses a significant barrier to obtaining needed healthcare. Although clinics can incorporate measures to improve access for patients with inflexible work hours, such as extended clinic hours or virtual appointment options, addressing and advocating for paid parental leave and extended insurance coverage postpartum at the state and national policy level would likely be most impactful.25,26 Similarly, previous research has identified access to childcare as a substantial obstacle for patients seeking peripartum health appointments.10–12,14–19 Our results underscore the difficulties patients encounter in accessing childcare, with 29% of the study population citing it as a barrier to attending appointments. Numerous patients also identified “being too busy” as a primary obstacle to attending medical appointments. Prior qualitative studies examining barriers to accessing prenatal care have emphasized that having hectic schedules and addressing essential needs such as food and shelter, take precedence over medical appointments, especially for low-income women,.15,16 For instance, a study conducted among low-income women in New York City found that one of the top two reasons for delaying care was “needing time and energy to deal with other problems.” 15
Interventions that were most commonly perceived as helpful by participants in this study included virtual appointment options, increased insurance coverage, and provision of childcare (Figure 2). Notably, more participants rated interventions as helpful for attending appointments than reported barriers to attending appointments, indicating that many interventions would be widely utilized by patients regardless of barriers faced.
The availability of virtual appointment options could mitigate numerous barriers linked to accessing peripartum care, including the aforementioned challenges of accessing childcare and the inability to take leave from work. Research indicates that patients have positive impressions of and high satisfaction with virtual appointments for peripartum care. Furthermore, these appointments offer additional benefits including enhanced comfort, convenience, and ease of communication. 27 Our findings support the argument that healthcare systems catering to peripartum patients should expand virtual appointment offerings when deemed medically suitable. Many patients also frequently viewed increased insurance coverage as beneficial when attending appointments. In Rhode Island, all patients who are pregnant and postpartum to 12 months with income below 250% of the Federal Poverty Line are provided with medical insurance, resulting in our population having no uninsured patients. 28 However, despite this insurance provision, research demonstrates that financial barriers persist for many patients as a result of being underinsured.14,15,17,19,29,30 Improved insurance coverage could alleviate the financial strain associated with accessing peripartum healthcare. Lastly the implementation of childcare services has proven effective in other healthcare systems. Specifically, a public health system in Texas partnered with a community-based organization to pilot childcare services after surveys identified childcare as the most commonly reported reason reproductive-age patients missed or delayed healthcare. Initial reports indicated the engagement of 175 patients and over 270 children. 31 Nevertheless, few healthcare organizations have established comparable programs, highlighting the substantial need for such services. An intervention to collectively mitigate barriers due to insurance coverage, appointment options, and the burden of childcare is patient navigation, which has also been shown to be especially effective among populations facing health disparities. 32
In this study, 59% of participants identified as non-Hispanic White, whereas statewide 70% of residents identified as non-Hispanic White. 33 Black, Asian/Pacific Islander, and Hispanic participants were slightly overrepresented in the sample compared to state demographics, possibly due to the clinic's location in Providence, RI, which is more ethnically diverse than the state of Rhode Island.33,34 Hispanic and Black patients reported experiencing more barriers to care compared to patients of other ethnicities in the study, suggesting significant racial and ethnic disparities in access to peripartum care. This finding aligns with prior literature demonstrating increased social determinant of health barriers for Black and Hispanic pregnant patients.8–10,13,16,17,30 These health barriers stem from systemic and structural racism and factors affected by social determinants of health rather than race or ethnicity itself.35,36 Race and ethnicity are socially constructed and reflect multiple dimensions of cultural, historical, and political factors that influence health perceptions, behaviors, and outcomes.35,36 These barriers, influenced by the social constructs of race and ethnicity, likely contribute to the observed maternal health disparities between White and non-White patients.37,38 Our findings may aid in improving health outcomes and directing resources appropriately for these marginalized racial and ethnic populations, thereby centering health equity in care. In conclusion, our findings underscore the importance of future interventions targeting the reduction of barriers to care for peripartum patients, with a specific focus on outreach to Black and Hispanic patients to mitigate existing disparities.
Limitations
Our study had several limitations. Firstly, our survey was only administered to patients who attended at least one obstetric medicine clinic appointment. As such, it did not capture patients who were unable to attend any appointments and were therefore possibly facing the most barriers to care. However, since interventions were generally rated as helpful regardless of barriers, this group would likely also benefit from the interventions outlined in this study. Additionally, our survey was administered at a clinic within a northeastern state that provides medical insurance for all patients during pregnancy and the postpartum period up to 12 months. 28 Therefore, the conclusions of our survey may not be generalizable to other geographic areas in which not all peripartum patients have access to insurance coverage. Moreover, the response rate for the survey could not be ascertained as information on the number of patients offered the survey was not collected. Also, while our study found that language was not a significant barrier to care, it is important to note that we did not assess lack of cultural competency as a barrier, which can contribute to disparities in care.39,40 Lastly, zip code data in the supplemental table was used as a proxy for sociodemographic factors, as exact sociodemographic information was not available.
Conclusion
In this study, 226 patients at an obstetric medicine clinic in Providence, RI serving peripartum patients referred due to additional health needs experienced barriers to care, including the inability to take leave from work, being too busy, and lack of access to childcare. Many participants, regardless of barriers faced, perceived interventions such as increased virtual appointment options, increased insurance coverage, and provision of childcare to be helpful in accessing care. Hispanic and Black patients were significantly more likely to report experiencing barriers to care compared to White patients, suggesting racial and ethnic disparities in access to peripartum care. As maternal morbidity and mortality increase in the United States, ensuring equitable access to and engagement in peripartum care remains of the highest priority. 41 Our results demonstrate that future interventions may be most impactful by focusing on the provision of virtual appointments and childcare services as well as increased efforts to reduce financial barriers for patients, especially those from marginalized racial and ethnic backgrounds.
Supplemental Material
sj-docx-1-obm-10.1177_1753495X241255812 - Supplemental material for Accessing peripartum care in an internal medicine clinic: Barriers, interventions, and racial disparities
Supplemental material, sj-docx-1-obm-10.1177_1753495X241255812 for Accessing peripartum care in an internal medicine clinic: Barriers, interventions, and racial disparities by Kanika Malani, Sarah Arbaugh and Courtney Bilodeau in Obstetric Medicine
Footnotes
Authors’ Notes
Kanika Malani and Sarah Arbaugh contributed equally to this work.
Acknowledgments
We would like to thank the Women's Medicine Collaborative for supporting this work.
Author contributions
Conceptualization: KM, SA, and CB; methodology: KM, SA, and CB; formal analysis: KM; investigation: KM and SA; resources: CB; data curation: KM and SA; writing original draft: KM and SA; writing-review and editing: KM, SA, and CB; visualization: KM and SA; supervision: CB; project administration: KM, SA, and CB.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study was deemed to be a quality improvement study and not human subjects research by the Brown University Human Subjects Research Self Determination Tool and the National Institute of Health Human Subjects Research Decision Tool.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
All patients provided informed consent to participate in this study.
Guarantors
Kanika Malani, Sarah Arbaugh, and Courtney Bilodeau
Data transparency statement
The data that support the findings of this study are not openly available due to reasons of sensitivity and protection of participant privacy. An anonymized version may be made available from the corresponding author upon reasonable request. Data are located in controlled access data storage.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.