
Abstract
Background
Transthoracic echocardiography, a validated tool for risk assessment in non-pregnant population with sickle cell disease (SCD), uses tricuspid regurgitant velocity (TRV) over 2.5 m/s is an independent mortality risk factor. Its applicability in obstetrics lacks sufficient evidence.
Methods
In this multicenter retrospective cohort study across five tertiary centers, we aimed to validate TRV as a determinant of increased maternal and fetal risk. Data was collected on 93 women and included 21 patients with TRV of at least 2.5 m/s. The maternal primary composite outcome included occurrence of vaso-occlusive crisis, acute chest syndrome, gestational hypertension, preeclampsia, and mortality. The fetal primary composite outcome comprised perinatal mortality, premature delivery, reduced birth weight, and fetal distress.
Results
Adverse maternal and fetal events arose in both groups with no statistical difference.
Conclusion
This study cannot support TRV of 2.5 m/s or more as an independent predictor of adverse obstetric outcomes among women with SCD.
Introduction
During pregnancy, pulmonary hypertension is associated with increased morbidity and mortality.1,2 Women with sickle cell disease (SCD) can be affected by pulmonary hypertension at childbearing age and, therefore, be prone to adverse obstetric events, including increased incidence of preeclampsia, premature delivery, small birth weight, and SCD-related complications such as acute chest syndrome (ACS) and vaso-occlusive crisis (VOC).3–8
Right heart catheterization is the gold standard to diagnose pulmonary hypertension but is invasive and not readily available. To screen patients in preconception or during pregnancy, other non-invasive methods, such as transthoracic echocardiography (TTE) are more convenient. Outside of pregnancy, studies have demonstrated that a tricuspid regurgitation velocity (TRV) of 2.5 m/s or more is an independent risk factor of mortality in patients with SCD. 9 However, few studies aimed to validate its use in pregnancy. The Royal College of Obstetricians and Gynaecologists (RCOG) recommends TTE screening for pregnant patients with SCD, 10 but more research is needed to support these guidelines.
Our hypothesis was that a TRV of at least 2.5 m/s would be a risk factor for maternal and fetal complications. The objective of this study was to validate TTE use as a reliable screening tool in pregnancy. It will help guide clinicians as to which patients are at increased obstetric risk, to provide better preconception guidance and individualized follow-up throughout pregnancy.
Methods
A multicenter retrospective cohort study was conducted on revised charts from 1 January 2003, to 31 December 2018. Women with SCD who delivered or were hospitalized after 20 weeks of gestation were screened in these five Canadian tertiary and quaternary centers: Centre hospitalier de l’Université de Montréal, Centre hospitalier universitaire Sainte-Justine, Hôpital Maisonneuve-Rosemont, Centre universitaire de Santé McGill and Centre hospitalier et universitaire de Sherbrooke.
Inclusion criteria were adult pregnant women with SCD with a minimum of 20 weeks of gestation who had a TTE done within 1 year prior to conception or during pregnancy. The study population was subclassified as an exposed group (TRV of at least 2.5 m/s) and a non-exposed group (TRV under 2.5 m/s, or undetectable). In the latter group, we included patients with no tricuspid regurgitation, as pulmonary hypertension was considered to be very unlikely in this context.3,11
Exclusion criteria were non-singleton pregnancies and patients that had a significant echocardiographic abnormality unrelated to pulmonary hypertension, such as valvulopathy (except for tricuspid regurgitation) or left ventricular dysfunction. Also, if a patient had multiple pregnancies during the screening period, only the first pregnancy was included.
The primary maternal outcome was a composite of the occurrence of VOC, ACS, gestational hypertension, preeclampsia, and mortality. The primary fetal outcome was a composite of the occurrence of perinatal mortality, premature delivery, reduced birth weight, and fetal distress. VOC was defined as an episode of acute bone pain requiring opioid use that was not better explained by another etiology. 12 ACS was defined as an episode of respiratory symptoms (dyspnea, cough, rales, or indrawing) associated with a new pulmonary infiltrate on chest X-ray. 13 Definitions of gestational hypertension and preeclampsia were consistent with Magee et al.'s definition (2016). 14 Perinatal mortality included intrauterine death occurring after 22 weeks of gestation and neonatal death within seven days of life. 15 Premature delivery was a birth occurring before 37 weeks of gestation. 16 Reduced birth weight was a weight under the 10th percentile according to gestational age and sex of the newborn. 16 Finally, fetal distress was defined by an APGAR under 5 at 5 min, a pH under 7 on the umbilical cord blood gas analysis, or abnormal fetal heart rate tracings leading to an assisted vaginal delivery or a caesarean section.
Secondary maternal outcomes were eclampsia, thromboembolic event, stroke, antepartum and postpartum hemorrhage, induction of labor, caesarean section, and the need for transfusion or erythrocytapheresis during pregnancy. Antepartum hemorrhage was defined as vaginal bleeding occurring after 20 weeks of gestation and which was not related to labor or delivery. Postpartum hemorrhage was diagnosed if the blood loss estimated by the obstetric team during labor was over 500 ml for vaginal delivery or over 1000 ml for a caesarean section. The secondary fetal outcomes were neonatology admission, birth weight, gestational age, and Apgar score under 7 at 5 or 10 min.
Data were collected on maternal age at delivery, parity, SCD genotype, BMI, smoking status, university education, pregestational evaluation in specialized clinics for high-risk pregnancies, past medical history (caesarean section, chronic or gestational hypertension, preeclampsia, pre-existing or gestational diabetes, fetal growth restriction, placental abruption, ACS, stroke, proliferative retinopathy, and chronic kidney injury), use of hydroxyurea, prophylactic or therapeutic erythrocytapheresis and prophylactic or therapeutic transfusion in preconception, and aspirin during pregnancy. Baseline levels of hemoglobin, lactate dehydrogenase (LDH), bilirubin, reticulocytes, and creatinine were recorded, as well as the nadir level of hemoglobin and the zenith levels of LDH, bilirubin, reticulocytes, and creatinine reached during pregnancy.
The primary objective was to compare maternal and fetal outcomes depending on tricuspid regurgitation velocities (<2.5 m/s vs ≥2.5 m/s), either measured pre-pregnancy or per-pregnancy. The secondary objectives were to determine the prevalence of a TRV of 2.5 m/s or more in our population, the effect of genotypes (HbSS, HbSC, HbSB+, HbSB0) on the presence of an increased TRV (≥2.5 m/s), and to compare the severity of hemolysis parameters depending on TRV values.
Data analysis
Sample size is relatively small and due to concerns of non-normality, results are presented as median and interquartile range. Binary variables are presented as proportions. The Wilcoxon signed-rank test was used to test the research hypothesis. A two-tailed alpha of 0.05 was considered significant for all analysis. Data were analyzed with the use of the R programming language. Boxplots were produced to visually assess the discriminant value of TRV.
Informed consent was not sought for the present study because it was a retrospective cohort study involving de-identified patient data obtained from medical records and did not involve any direct patient contact. Ethical approval for this study was obtained from the CHUM Institutional Research Board (MP-02-2020- 8533).
Results
We screened a total of 137 patients and excluded 44 patients because 37 had no TTE, two had twin pregnancies, one was under 18 years old, and four had other abnormal echocardiographic findings (one TTE showed abnormal left ventricular contractility and three demonstrated significant valvulopathies). Altogether, 93 women were included for analysis. Seventy-two had a TRV under 2.5 m/s and 21 had a TRV of at least 2.5 m/s (Figure 1). When comparing their demographic characteristics, both groups were similar in terms of SCD-related complications, obstetric history, and paraclinical parameters, amongst others (Table 1). The only exceptions were bilirubin levels and c-section history that were higher in the group with TRV of 2.5 m/s or more. Other parameters of hemolysis were also concordantly slightly more elevated, but not attaining statistical significance.

Study cohort.
Demographic characteristics of pregnant patients.

IQR: interquartile range; LDH: lactate dehydrogenase (U/L); sPAP: pulmonary systolic artery pressure (mmHg); TTE: transthoracic echocardiogram; TRV: tricuspid regurgitation velocity (m/s).
More specifically, pregestational evaluation were made in specialized clinics for high-risk pregnancies.
Baseline laboratory results were obtained within 6 months prior to conception or during the first trimester.
The median TRV was 2.1 m/s (IQR [1.9, 2.3]) in the non-exposed group and 2.7 m/s in the exposed group (IQR [2.6, 3.0]) (Table 1). Estimated pulmonary systolic arterial pressures (sPAP) ranged from 8 to 26 mmHg, and from 28 to 48 mmHg in the non-exposed and exposed groups, respectively. The primary maternal outcome occurred in 68% of the non- exposed patients, and in 50% of the exposed patients, with no statistically significant difference. The primary fetal outcome occurred in 55% and 30% of the non-exposed and exposed groups respectively, again with no statistically significant difference (Table 2). Each composite of maternal and fetal primary outcomes evaluated separately were also similar in both groups. The occurrence of secondary outcomes in both groups did not differ, except for higher rate of induction of labor and bilirubin levels in patients with a TRV of 2.5 m/s or more.
Primary outcomes.
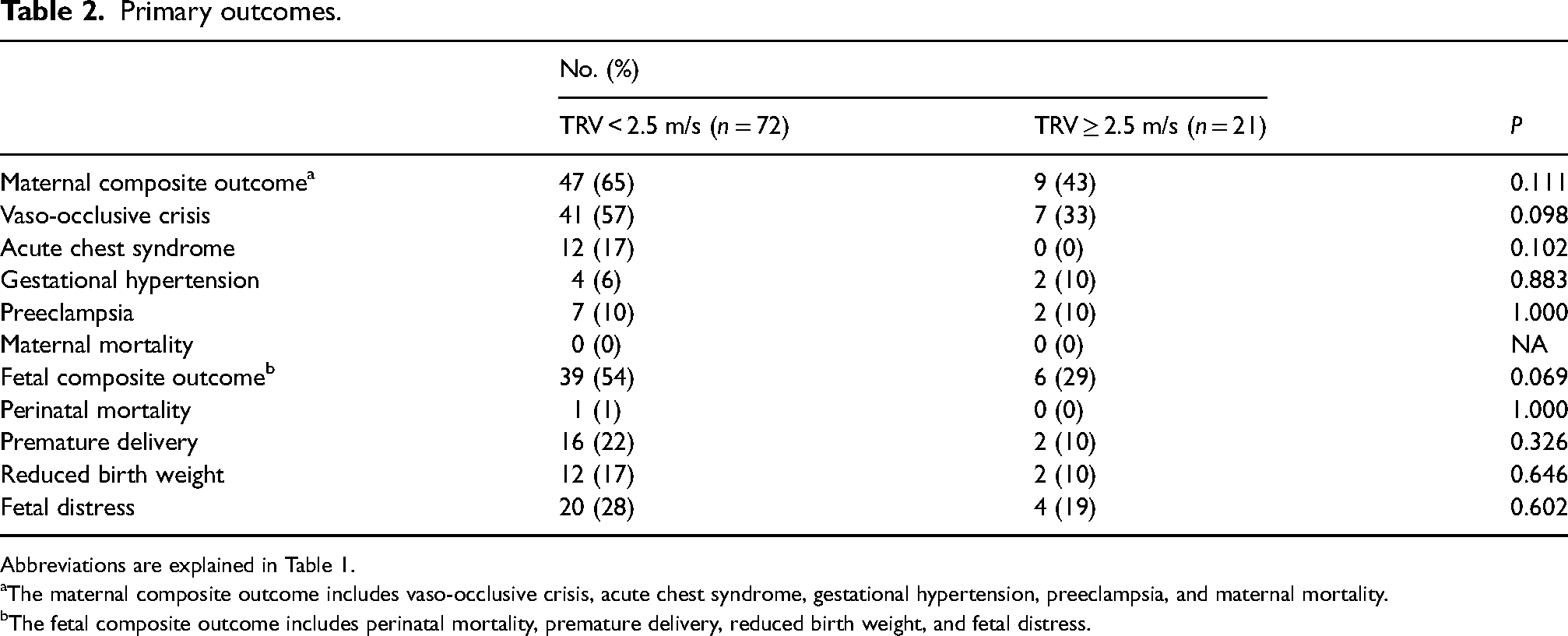
Abbreviations are explained in Table 1.
The maternal composite outcome includes vaso-occlusive crisis, acute chest syndrome, gestational hypertension, preeclampsia, and maternal mortality.
The fetal composite outcome includes perinatal mortality, premature delivery, reduced birth weight, and fetal distress.
The prevalence of a TRV of at least 2.5 m/s was 23% in our population. Of interest, we had six patients with a TRV of at least 3.0 m/s, which represents a 5% prevalence in our subset of patients. By comparison, the Soh et al.'s study had a prevalence of TRV of 2.5 m/s or more of 24% in their population, and no patients with a TRV of at least 3.0 m/s (Table 3). 17
Secondary outcomes.

IQR: interquartile range; LDH: lactate dehydrogenase; PCI: placental cord insertion; TRV: tricuspid regurgitation velocity; VBAC: vaginal birth after caesarean.
A postterm pregnancy is defined as a pregnancy that extends beyond 40 weeks.
Clinician decisions were based on maternal comorbidities.
Discussion
To our knowledge, this is currently the largest study aiming to determine the clinical impact of a TRV of 2.5 m/s or more on pregnancy outcomes in sickle cell patients. Based on our results and on previous literature, a TRV of at least 2.5 m/s is not, thus far, a validated independent risk factor for obstetric adverse events in this specific population.
TRV is, inter alia, a parameter of disease severity. During protocol development, we anticipated that the demographic profiles at baseline of our two groups (Figure 1) would diverge, and that the group of patients with a TRV of 2.5 m/s or more would have a more complicated medical history, as opposed to the patients with a TVR under 2.5 m/s. However, both groups had comparable baseline characteristics, beside a trend towards higher hemolysis markers in the group with TRV of at least 2.5 m/s. Similar obstetric outcomes were shown post-analysis as well. As the rate of maternal and fetal complications in our SCD study population is higher than the general population, even in women with TVR of less than 2.5 m/s, this underlines the importance for multidisciplinary approach and careful monitoring during pregnancy.
The fact that these women were followed in tertiary and quaternary centers, mainly by hematologists, and, that 18 patients (19%) were pre-evaluated in specialized clinics for high-risk pregnancies, may have selected the most favorable patients to conceive and render the two groups of our study more similar. Patients who were at higher risk, either based on their TTE parameters or other considerations, such as the severity of their disease, were possibly not screened. Therefore, our results might be more applicable to patients from urban settings with access to specific health care expertise.
A strength of this study was to include patients with an undetectable TRV on their TTE, considering its very low risk of elevated sPAP. Also, patients that had their TTE 12 months prior to conception as well as during pregnancy were included. Tso et al. demonstrated that TTE measurements before and during pregnancy are consistent, despite physiologic cardiovascular and cardiopulmonary changes. 18 The purpose of limiting these exclusion criteria was to increase study power in this small population and to avoid sampling bias. However, even with these supplemental measures, 44 patients (33%) had to be excluded mainly because they had no prior TTE. It cannot be excluded that these patients had different demographic profiles or medical follow-ups. A future prospective study with standardized TTE measurement is required.
Gladwin et al. showed that a TRV as mildly elevated as 2.5 m/s was statistically significant with an associated increased risk of mortality (rate ratio, 10,1; P < 0.001) in their non-pregnant and slightly older population (mean age of 36 years) compared to patients with TRV under 2.5 m/s. The usual TRV threshold for suspecting pulmonary hypertension is 2.9 m/s and more. Considering the younger age and the pregnancy status of our study population, a hypothesis could be that the discriminant cut-off value for these patients is higher. Consequently, it would have been of interest to evaluate the statistical and clinical impact on obstetric outcomes of a more elevated TRV value, but since its prevalence is even lower, an analysis with the same population pool would be underpowered.
Two other studies attempted to evaluate the prognostic value of TRV of at least 2.5 m/s in this context. Soh et al., with only eight patients with a TRV of 2.5 m/s or more, was underpowered and unable to demonstrate a difference in obstetric and perinatal ouctomes. 17 Marshal et al. which was published after our data collection, recruited 43 women (59 pregnancies) including 31 pregnancies with TRV of at least 2.5 m/s and found that these patients were at higher risk of adverse hematologic events (as defined in their study as a composite of venous thromboembolic event, VOC, ACS and need for transfusion in pregnancy, P = 0.03). However, there was no significant association with TRV ≥ 2.5 m/s and adverse cardiac and obstetric events. 19 In our study, however only one patient suffered from venous thromboembolism and had a normal TRV, which cannot corroborate the previous results.
Lastly, as the studies previously mentioned, the HbSS and HbSB0 genotypes were more prevalent in the exposed group (67% versus 33%) compared to other genotypes (HbSC and HbSB+), but with no statistically significant difference. Patients with HbSS and HbB0 genotypes commonly have more SCD-related adverse events and could possibly benefit the most from pulmonary hypertension screening. But, as there were still seven patients with HbSC or HbSB+ genotype with a TRV of 2.5 m/s or more, TTE screening should not be restricted to HbSS or HbSB0 patients based on these results.
Footnotes
Acknowledgments
John Davison provided editorial assistance to the authors during preparation of this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the CHUM Institutional Research Board (MP-02-2020- 8533).
Informed consent
Informed consent was not sought for the present study because it is a retrospective cohort study involving de-identified patient data obtained from medical records. The study design did not involve any direct patient contact, and confidentiality was strictly maintained to ensure anonymity.
Guarantor
MM.
Contributorship
AL reviewed the protocol, collected the data, contributed to data analysis, and drafted the manuscript. VW designed the study, collected the data, and reviewed the manuscript. PG, MT, NC, and VN collected the data and reviewed the manuscript. SG, BW, VC, and JV reviewed the protocol and the manuscript. MM overviewed the conduct of the study, contributed to study design and to results interpretation and reviewed the manuscript. All authors read and approved the final manuscript.