
Abstract
Familial chylomicronaemia syndrome (FCS) is a rare genetic disorder characterised by significantly elevated triglyceride levels which increases the risk of acute pancreatitis. Due to the changes in lipid metabolism during pregnancy, triglyceride levels may rise further, particularly in the third trimester, and cause challenges in the management of these patients. Apart from strict dietary restriction of all fats, there is limited evidence on the efficacy of pharmacological treatment with omega-3 fatty acids and fibrates in maintaining triglyceride levels below the desired threshold of 10 mmol/L. Familial chylomicronaemia syndromes are particularly resistant to treatment and escalation of treatment to more invasive procedures such as plasma exchange may be required in pregnancy. We present two cases of FCS in pregnancy which posed different challenges and both required management with plasma exchange but led to the safe delivery near term without adverse consequences to the mother or fetus.
Introduction
Chylomicronaemia is the accumulation of chylomicrons, large, triglyceride-rich lipoprotein particles produced after meals and that persist in the plasma despite fasting.1,2 Familial chylomicronaemia syndrome (FCS) is a rare autosomal recessive disorder in which high levels of circulating triglycerides (TGs) are secondary to pathogenic genetic variant homozygosity. 1 Mutations in the LPL (lipoprotein lipase) gene are responsible for >90% of FCS with an incidence of 1:1,000,000 individuals.2,3 Other genes have now been identified, some with very few kindreds worldwide (APOC2, APOA5, LMF1 genes). 2 Pregnancy is a state of hyperlipidaemia, particularly in the third trimester, where maternal fat deposition plays an important role in fetal growth and, as a consequence, circulating levels of different lipid fractions are increased. 4 More pronounced increases in TG levels have been reported in women with genetic chylomicronaemia during pregnancy, increasing the risk of acute pancreatitis.2,5 We report two cases of FCS managed at a tertiary Obstetric Medicine centre which posed different challenges and required escalation to plasma exchange.
Case 1
A 35 year-old woman with known FCS was referred during her second pregnancy. The diagnosis of FCS was established at the age of 11 years-old and known to be secondary to two pathogenic variants of the LPL gene. In her previous pregnancy, her TG levels had significantly increased from 19 weeks of gestation onwards and she was managed with plasma exchange 3-times a week, until an induction of labour (IOL) at 36 weeks’ gestation. She had a history of recurrent pancreatitis (3–5 episodes per annum) including during her previous pregnancy and had a cholecystectomy at three months postpartum. Her booking body mass index (BMI) was 19 kg/m2 (weight: 50.3 kg), and she was on a strict low-fat diet, omega-3-acid esters, 2 g, four times a day and fenofibrate, 267 g, once daily, which had been stopped by the patient at the start of pregnancy. She was referred at 11 + 3 weeks of gestation for admission in view of hyperemesis gravidarum and raised TG of 40.53 mmol/L (reference range <1.70 mmol/L). The total cholesterol was 8.9 mmol/L (reference range <2.5 mmol/L), and HDL was 0.35 mmol/L (reference range >1.2 mmol/L). Following this presentation and due to persistently high TG levels, she had her first plasma exchange (PlEX) and a plan was made for weekly TG level monitoring and potential weekly PlEX. Bezafibrate 200 mg, twice daily, was started at 15 weeks of gestation and omega-3-acid esters increased to 12 g, daily at 22 weeks’ gestation, after comprehensive discussion with the patient regarding risk versus benefit. The frequency of PlEX increased as pregnancy progressed from twice weekly at 19 weeks’ gestation to four times a week at 33 weeks’ gestation and daily from 35 weeks’ gestation as rebound TG were persistently >30 mmol/L (Figure 1) with a total of 72 plasma exchanges performed during pregnancy. A decision was made for induction of labour (IOL) at 36 weeks. The estimated fetal weight was on the 10th percentile. A female infant was delivered vaginally at 36 + 5 weeks of gestation weighing 2280 g.
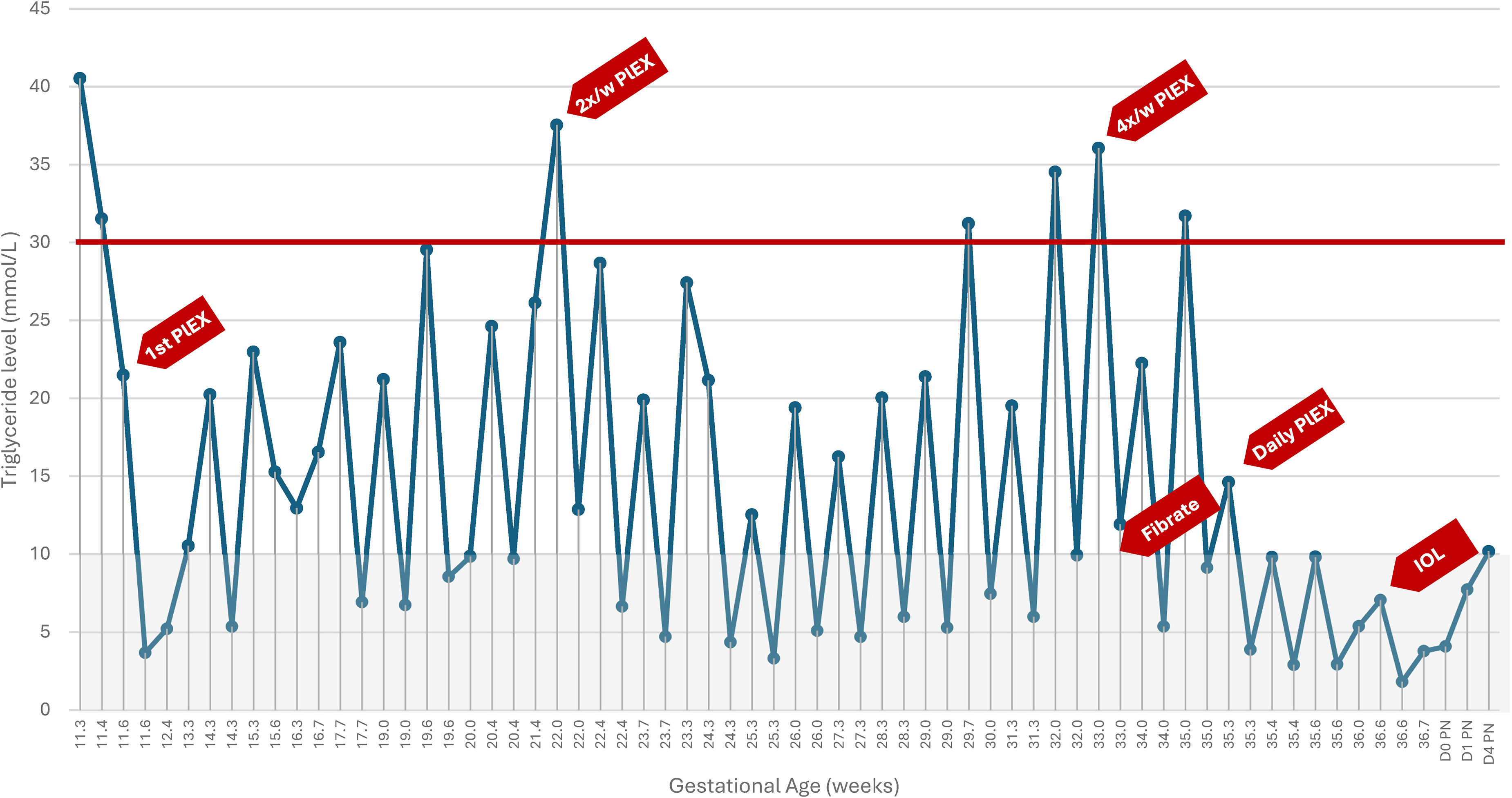
Graphic representation of triglyceride levels measured against gestational age for case 1. D: day; IOL: induction of labour; PlEX: plasma exchange; PN: postnatal. The grey shaded area represents the desired threshold of triglycerides <10 mmol/L. The red line represents the thresholds at which PlEX was considered (triglycerides > 30 mmol/L). The red arrows highlight important events as labelled.
Case 2
A 30 year-old woman, para 3 (all vaginal deliveries) was diagnosed with hypertriglyceridemia detected on ‘routine’ blood tests following the birth of her last child. She was prescribed regular omega-3-acid esters, 2 g, twice daily. The three previous pregnancies were complicated by gestational diabetes but no other complications of note. There was no history of acute pancreatitis. Genetic analysis showed homozygosity for the APOA5 pathogenic variant. The family history was unremarkable with no history of dyslipidaemia or premature cardiovascular disease. She was referred at 14 weeks’ gestation to the Obstetric Medicine clinic. On examination, the BMI was 23 kg/m2 (weight 62.3 kg), there were no stigmata of dyslipidaemia, the triglyceride (TG) level was 8.09 mmol/L, total cholesterol level was 4.9 mmol/L and HDL was 0.63 mmol/L. The risks of pancreatitis and plan to maintain TG <10 mmol/L were discussed. The patient was advised on continuing a strict low-fat diet and increasing omega-3-acid esters to 3 g twice a day. Regular testing of TG level was undertaken and these data are presented in Figure 2. At 33 weeks’ gestation, bezafibrate 200 mg twice daily was added to omega-3 in view of a significant increase in TG level which coincided with a period of non-adherence with diet and prescribed medication. At 35 weeks’ gestation a decision was made for plasma exchange in view of ongoing increase in TG level. Three plasma exchanges occurred at 35 + 6, 36 + 4 and 36 + 6 weeks’ gestation and IOL initiated at 37 + 0 weeks of gestation. She had an uncomplicated vaginal delivery of a female infant weighing 3620 g.
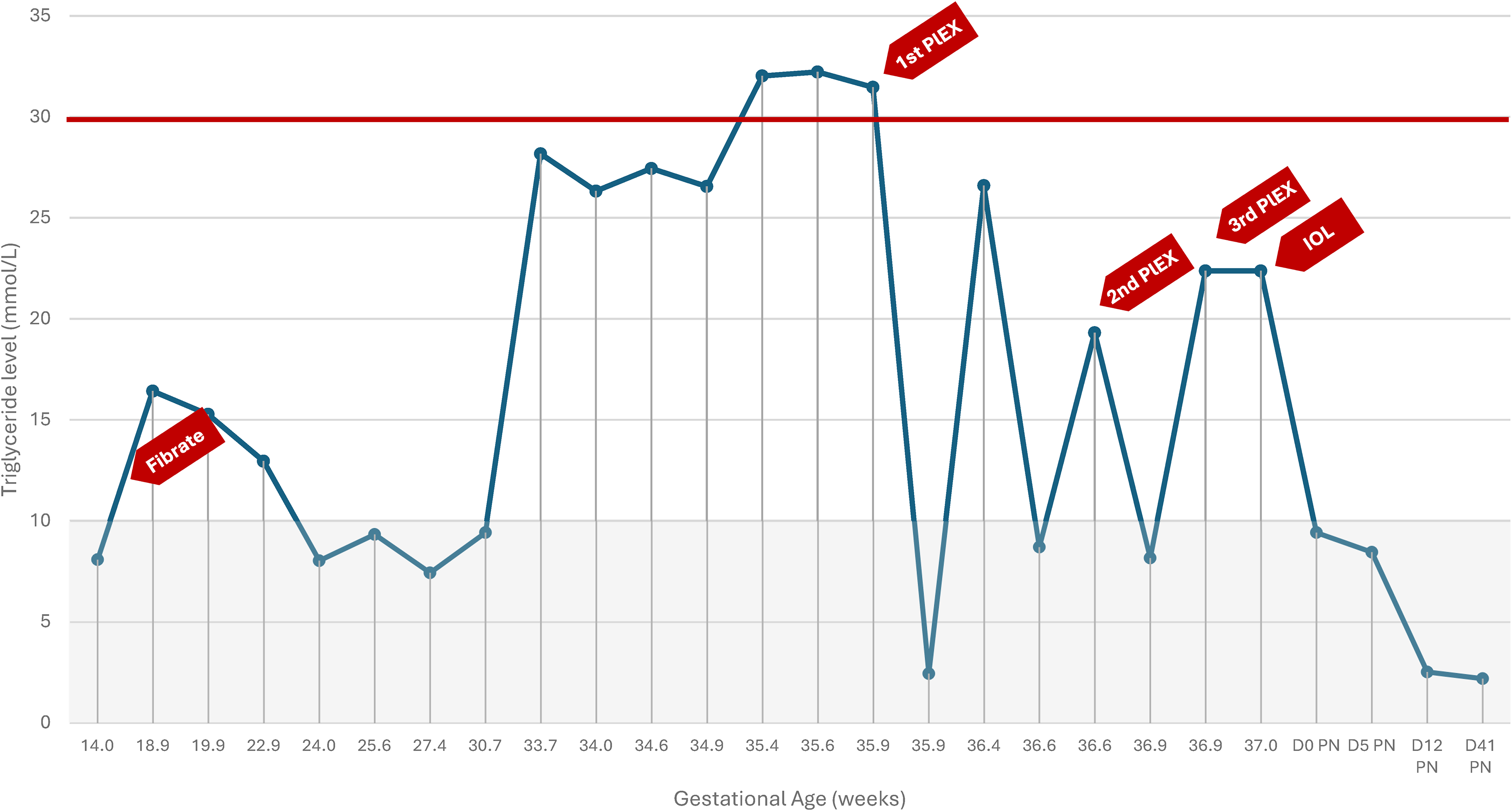
Graphic representation of triglyceride levels measured against gestational age for case 2. D: day; IOL: induction of labour; PlEX: plasma exchange; PN: postnatal. The shaded area represents the desired threshold of triglycerides <10 mmol/L. The red line represents the thresholds at which PlEX was considered (triglycerides > 30 mmol/L). The red arrows highlight important events as labelled.
Discussion
Acute pancreatitis is the most serious concern associated with FCS due to its complications and high mortality. 2 The absolute risk is highest when TG >20 mmol/L but the threshold for commencing plasma exchange should be based on several factors, including maternal history of pancreatitis, local expertise and, maternal choice. 2 The aims of treating FCS in pregnancy are to reduce the risk of acute pancreatitis in the short-term and reduce the risk of cardiovascular disease in the long-term. 3 Additionally, the risks to the fetus from exposure to high triglyceride concentrations in utero are largely unknown. Pancreatitis is rare during pregnancy with higher incidence in the third trimester and mostly secondary to gallstone disease. 6 Pancreatitis secondary to hypertriglyceridaemia is thought to be caused by toxic fatty acids derived from increase pancreatic lipase activity which hydrolyses the excess triglycerides. 7 These aggregate in micellar structures with detergent activity promoting microvessel injury and local ischemia.3,6–8 High concentrations of chylomicrons also increase blood viscosity causing further pancreatic ischemia and acidosis. 7 FCSs are particularly resistant to pharmacological treatment, especially the homozygous forms.3,9 The commonest pathogenic variant in FCS is homozygosity for LPL causing the loss of function of the LPL gene.2,10 APOA5 is most commonly associated with multifactorial chylomicronaemia syndrome and its dysfunction can impact LPL activity and availability. 10 Patients with non-LPL FCS usually experience better hypertriglyceridemia control compared to LPL FCS and this is demonstrated in our two cases with the patient in Case 1 (LPL mutation) requiring frequent PlEX and experiencing rapid rebound hypertriglyceridemia. 10
The mainstay of treatment is a very low-fat diet with restriction of dietary fat to 10–15% of the total daily energy intake which corresponds to about 20–40 g of fat per day. Achieving this can be particularly challenging as most Western diets consist of about 120 g of fat/day.1,9 Both our patients demonstrated good adherence to diet and had BMIs within normal range. At high doses (4–6 mg), omega-3 fatty acids block VLDL production and increase lipolysis and clearance of chylomicrons via inhibition of apolipoprotein (apo)C-III. 2 It is postulated that these are processed differently to saturated fatty acids and affect the formation of chylomicrons in the enterocytes leading to a reduction in circulating TG.9,11 Studies have shown conflicting results as there are different preparations containing omega-3 fatty acids and only pharmacological preparations containing highly purified fatty acids will be effective. 9 Omega-3 fatty acids are safe in pregnancy and, in both cases reported, an escalation in dose was tried earlier in the pregnancy, although their true efficacy has not been established. 2 It is believed that the additional fatty acid load does not affect triglyceride levels. 12 The use of medium-chain triglycerides (MCT) has also been suggested as these do not stimulate the production of chylomicrons and seem to reduce TGs. There is anecdotal evidence of these being successfully used in pregnancy and they can contribute to the overall caloric intake, although it is not our practice to use these.10,12 There is limited evidence on the use of fibrates in pregnancy and the BNF (British National Formulary) advises against their use in pregnancy and breastfeeding. However, our group has used both fenofibrate and bezafibrate in pregnancy without adverse outcomes identified. Fibrates can be used in pregnancy for their lipid lowering activity by increasing LPL activity.5,9 TGs levels can be reduced up to 50% with fibrates but it takes a few weeks to observe an effect. In case 1, the patient had stopped her fibrate before pregnancy and was reluctant to take these until 15 weeks of gestation. The baseline TG levels remained relatively high and unchanged with the addition of fibrates. In case 2, there was a drop in TG levels after initiating fibrates until about 24 weeks of gestation but there was a significant increase in TG levels around 33 weeks of gestation and despite escalating the dose of omega-3 esters and fibrates, TG levels continued to increase.13,14 For urgent and immediate lowering of TG levels, PlEX may be required. 6 Fibrates can be useful in patients with a functional lipolytic pathway. 12 Fibrates seemed to work better in case 2, where the pathogenic variant was non-LPL related. The threshold for PlEX should be made on a case–case basis by a multidisciplinary team, in discussion with the patient. Sufficient time for planning and organisation should be given. In case 1, PlEX was considered early in the pregnancy due to the significantly high TG levels at presentation and in view of the patient's previous history (recurrent pancreatitis, previous PlEX in a previous pregnancy). In this patient, there was a relatively quick rebound in TG levels (within a week) to levels between 20 and 30 mmol/L and a decision was made to continue with weekly PlEX which was then escalated to twice weekly at around 22 weeks’ gestation. From the third trimester onwards, a time where there is a physiological significant increase in TG levels, there was worse and quicker rebound prompting escalation to 4x/week PlEX. Levels of TGs were only under the desired threshold of 10 mmol/L after increasing PlEX to daily. In case 2, worrying levels of TGs also occurred in the third trimester (in this case at 35 weeks’ gestation) with a short term effect subsequently requiring repeated PlEXs. PlEX can reduce TG by 60–70% rapidly with limited maternal or fetal side-effects.1,6,15 The effect of PlEX is transient and therefore careful monitoring is required. 16 Guidelines advocate the use of PlEX in pregnancy as ‘fibrates are contraindicated’. 16 In both cases, PlEX was effective in lowering TG levels albeit of short duration.
FCS is a condition that is not frequently encountered and different clinicians will have different therapeutic approaches. The lack of truly effective therapies have led to researching novel therapeutic options including microsomal triglyceride transfer protein inhibition (MTTP, lomitapide), lipoprotein gene therapy, diacylglycerol O-acyltransferase 1 inhibition, APOB interference, APOC3 interference (volanesorsen, olezarsen), angiopoietin-like protein 3 interference (evinacumab).2,12 Although it is unlikely there will be trials of these drugs in pregnancy, more therapeutic options may come into clinical practice after safety and efficacy have been proven. Perhaps our experience and ease of access to PlEX has influenced our therapeutic decisions and both cases highlight the safety of plasma exchange in pregnancy without any maternal or fetal adverse events reported. It also highlights the importance of multidisciplinary input, in our case, Obstetricians, Obstetric Physicians and the Metabolic Medicine team to agree on strategy and timing of delivery.
Footnotes
Acknowledgements
The authors would like to thank the wider multidisciplinary team involved in the management of these women, in particular, Dr Alessia David and lipid nurse specialist Lucy Barton.
Authorship
SJ and FDS conceived the idea. FDS produced the first draft. SJ, SW, JC and CNP reviewed and provided input in subsequent versions. All authors edited and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Francois Dos Santos is the guarantor for the present work.