
Abstract
Splenic artery aneurysm (SAA) rupture in pregnancy is an unpredictable and rare emergency associated with maternal and fetal mortality. Ruptured SAA is characteristically diagnosed at laparotomy and managed with splenectomy, with embolisation favoured for uncomplicated cases. We report a case of a ruptured SAA in a morbidly obese pregnant woman with medical comorbidities, who presented as a diagnostic dilemma, but was subsequently managed successfully with interventional radiology at the time of caesarean section.
Keywords
Introduction
Splenic artery aneurysm (SAA) rupture in pregnancy is a true emergency, associated with a high maternal and perinatal mortality rate. 1 We report a case of a ruptured SAA in a morbidly obese pregnant woman, which was managed successfully with interventional radiology (IR) at the time of caesarean section.
Case report
A 34-year-old Gravida 3 Para 1 at 34 weeks and 3 days gestation presented to the Maternity Unit with upper abdominal pain.
Her relevant history included one previous caesarean section, type 2 diabetes mellitus, controlled with insulin, and class IV obesity (booking weight 198 kg). She had no relevant family history of connective tissue or cardiovascular disorders. She received multidisciplinary care at our tertiary centre. Growth scans demonstrated fetal macrosomia, and her pregnancy was otherwise uncomplicated.
The woman described the acute onset of epigastric pain that woke her from sleep. The pain was colicky in nature and migrated across the abdomen, with associated nausea but no vomiting. She denied any change to fetal movements, vaginal loss, or change to urinary or bowel habits. She was tachycardic with a heart rate of 107 b/min, tachypnoeic with a respiratory rate of 32 breaths/mn, and hypotensive 94/62 mmHg (compared to a baseline antenatal blood pressure of 120/76). On abdominal examination, there was generalised tenderness in the upper quadrants, with no peritonism. There was no uterine activity palpable. A cervical examination was unremarkable. A fetal cardiotocograph (CTG) demonstrated fetal tachycardia. Maternal and fetal tachycardia both responded to intravenous fluid resuscitation. She had a new finding of anaemia with a haemoglobin of 102 g/L (Previously 125 g/L at 30 weeks gestation). There was a normal white cell count, renal and liver function, and C-reactive protein. An upper abdominal ultrasound was unremarkable but was of poor quality secondary to body habitus. Her pain improved with oral analgesia, and a proton pump inhibitor.
Ten hours after presentation, the woman experienced a further episode of severe generalised abdominal pain radiating to the shoulder tip, with associated hypotension with a systolic blood pressure of 80 mmHg, tachycardia of 128 b/min, and a brief episode of loss of consciousness. A Medical Emergency Team response was called, and further fluid resuscitation was undertaken with a good response. A plan for computed tomography (CT) pulmonary angiogram and abdomen was made to exclude pulmonary embolus, SAA or aortic pathology; however, whilst awaiting imaging, the CTG demonstrated absent variability and fetal bradycardia of 8 min with recovery. Due to her undifferentiated abdominal pain and history of a previous caesarean section, there was an obstetric concern for a uterine rupture or placental abruption. The decision for emergency delivery was made.
Entry by Pfannenstiel incision led to the discovery of a massive haemoperitoneum with an intact uterus. A live female infant was delivered in poor condition. There was no placental abruption. The uterus was closed, and there was adequate uterine tone following. The woman was resuscitated following activation of the massive transfusion protocol and administration of intravenous tranexamic acid. There was evidence of ongoing bleeding running down from the upper abdomen. The differential diagnosis included a ruptured SAA, and a ruptured benign liver tumour, such as an adenoma, that can increase in size during pregnancy due to increased oestrogen. A multidisciplinary team, including general and vascular surgeons and an interventional radiologist were called to attend. Due to her habitus, the upper abdomen was unable to be accessed through the Pfannenstiel incision, and extension to a midline laparotomy was considered to not only be technically challenging but could further delay definitive treatment due to revision of pannus retraction and patient positioning. Following careful consideration, the abdomen was packed, and the woman was transferred for a CT angiogram, which demonstrated a ruptured SAA (Figure 1). She was then transferred to a hybrid angiography suite where she underwent successful embolisation of the ruptured SAA (Figure 2). The abdominal packs were then removed, uterine atony was noted, and intravenous uterotonics were administered to good effect. The pelvis was irrigated and subsequently closed, with a drain left in situ for the residual haemoperitoneum.
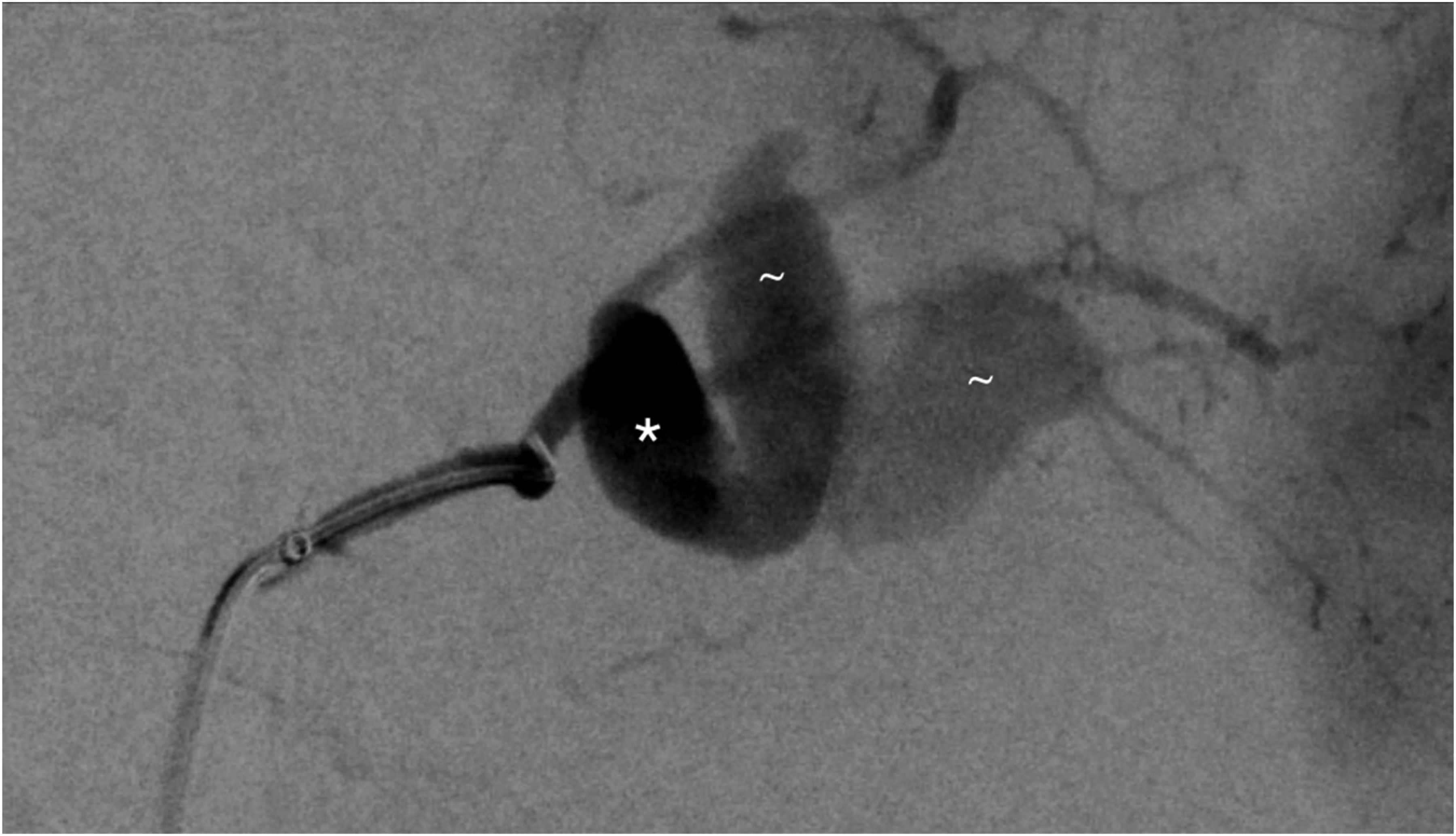
Splenic artery digital subtraction angiography (DSA) showing partially collapsed splenic artery aneurysm (*) at splenic artery bifurcation with large, lobulated pseudoaneurysm (∼) contained by sentinel clot.
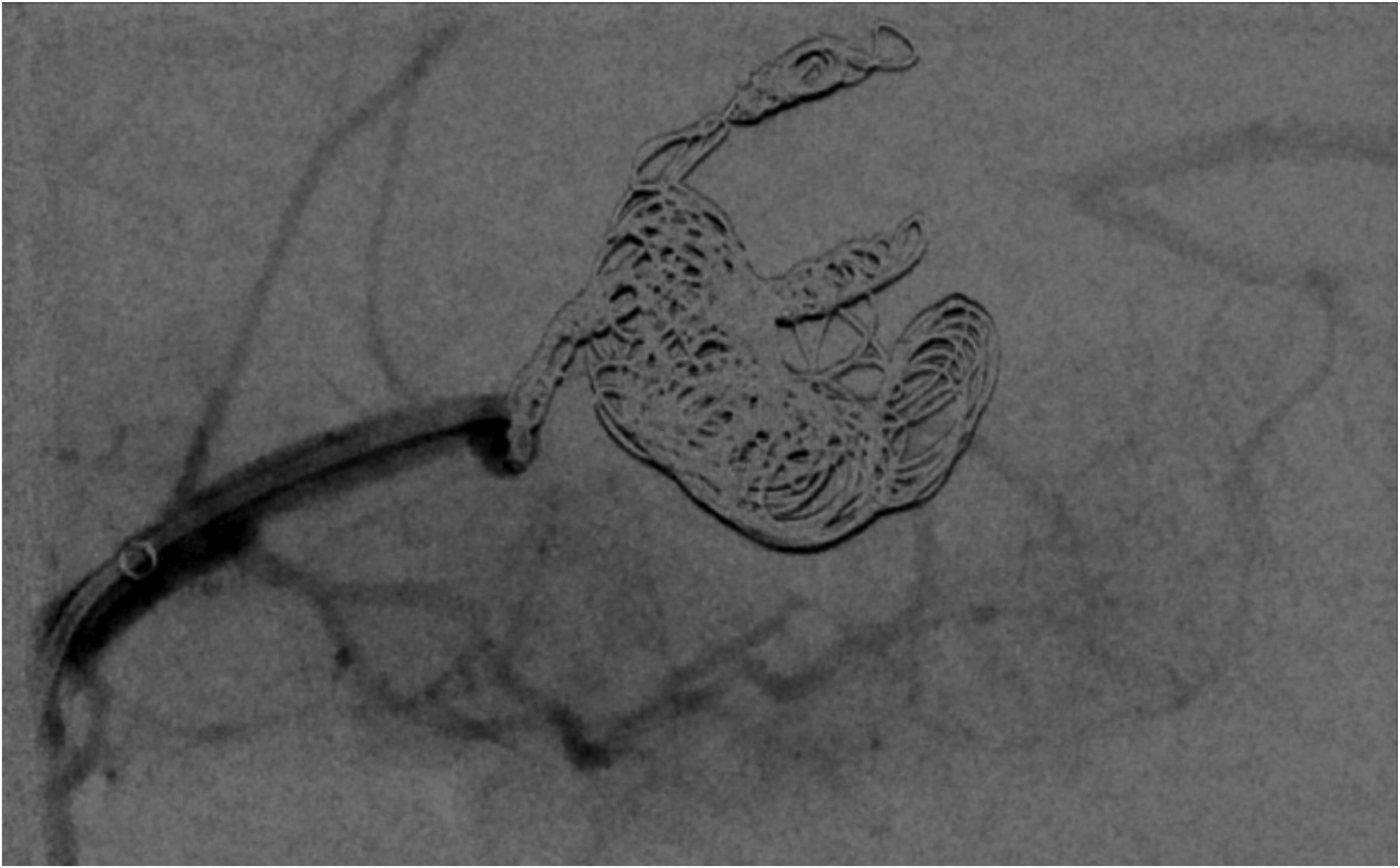
Completion DSA post-endovascular coiling demonstrating complete occlusion of the aneurysm with lower pole splenic perfusion preserved by collateral supply.
Post-operatively, she was admitted to ICU and later to the surgical ward. She received a total of five packed red blood cells, 10 units cryoprecipitate, and five fresh frozen plasma. This woman was high risk for postpartum venous thromboembolism; prophylactic enoxaparin was commenced on day 1 postpartum and continued on discharge for a total of six weeks. Imaging on day three post-operatively confirmed successful occlusion of the previously ruptured SAA with no evidence of a rebleed. The superior pole of the spleen was infarcted, but the inferior pole remained well perfused. There was no evidence of cirrhosis or stigmata of portal hypertension. She was discharged home on day nine post-operatively. The neonate had respiratory distress syndrome, anaemia corrected by a blood transfusion, and hypoglycaemia. She did remarkably well with no evidence of neurological impairment and was discharged home at 13 days of life.
We followed the woman up at three months postpartum. We have recommended against any future pregnancy, due to a high risk of recurrence of aneurysm rupture.
Discussion
SAA rupture in pregnancy is an unpredictable and rare emergency associated with a high risk of maternal and fetal mortality. 1 Ruptured SAA is characteristically diagnosed at laparotomy and managed with splenectomy. Advancements in IR have provided an alternative to surgical intervention, with the advantage of rapid haemorrhagic control, preservation of splenic function in select cases, and minimally invasive techniques.
Successful embolisation of a ruptured SAA has been described in several cases diagnosed in the midtrimester.2, 3 One case has described successful embolisation of a ruptured SAA diagnosed at the time of caesarean section as a temporising measure prior to splenectomy. The neonate did not survive. 4 Most cases in the literature describe surgical intervention during caesarean section, with extension to a midline laparotomy for surgical access and splenectomy. 1 In our case, morbid obesity provided a significant challenge for surgical access. The multidisciplinary team evaluated the complexities of an alternative surgical approach (via a supraumbilical midline laparotomy incision), versus stabilisation of the woman and transfer for CT angiogram with subsequent embolisation.
Our case also highlights the unique challenges with diagnosis and management in the morbidly obese woman. The most common first-line radiological investigation is a transabdominal ultrasound, which will commonly demonstrate free intraabdominal fluid and a perisplenic haematoma. 5 In our case, the diagnostic utility of ultrasound was significantly reduced, which subsequently delayed the diagnosis. Surgical intervention in the morbidly obese woman also poses challenges, including patient positioning with appropriate bariatric equipment, pannus retraction, additional staff to retract, and longer operating time. 6 Post-operative complications are also more common. 6
Furthermore, our case is also characteristic of the double rupture phenomenon observed in ruptured SAA. 7 This phenomenon describes a two-phase process of haemorrhage, where initially the SAA ruptures into the lesser omental sac and is contained by a sentinel clot. This containment will often present with symptoms of abdominal pain and mild hypotension, consistent with the initial presentation for our case. The sentinel clot will then commonly rupture sometime after, resulting in catastrophic rupture into the peritoneal cavity, leading to haemorrhagic shock, progressive fetal heart rate abnormalities secondary to maternal shock, and if left untreated, maternal and fetal death.
In summary, whilst IR techniques have been successful in the management of SAA, their concurrent use with caesarean section has not been frequently reported. In centres without IR, surgical intervention for ruptured SAA should remain the treatment of choice, and management should be individualised and approached with a multidisciplinary team.
Footnotes
Contributorship
EW wrote the first draft of the manuscript and conducted a literature review. TR provided images. All authors reviewed and edited the manuscript and approved the final version.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This case study was granted an exemption from the Human Research Ethics Committee review.
Informed consent
The patient provided written informed consent for their anonymised information to be published in this article.
Guarantor
EW is the guarantor who ensures the accuracy, completeness and validity of the case report.