
Abstract
Nausea, vomiting and anaemia are common complications of pregnancy. A case of hyperemesis and unexplained anaemia in a woman of South Asian ethnicity is presented. Further investigation revealed hypothalamic–pituitary–adrenal axis insufficiency and lead toxicity, most likely secondary to an Ayurvedic powder she had recently ceased. The importance of considering adulteration of complementary and alternative preparations as a cause of pregnancy complications is discussed.
Case report
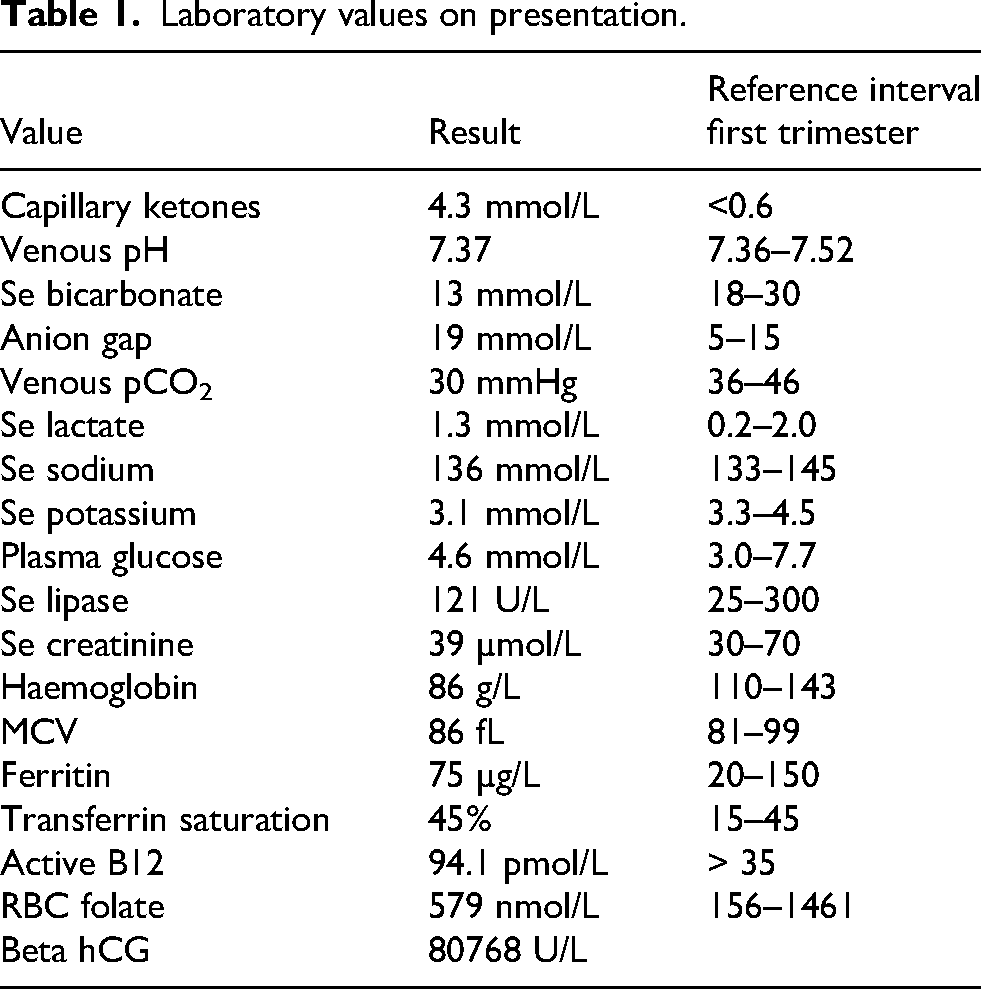
A 27-year-old woman, 7 weeks’ gestation in her first pregnancy, presented with the inability to tolerate oral intake due to persistent vomiting despite treatment with doxylamine and ondansetron, having had three admissions to another hospital in the prior 2 weeks for hyperemesis gravidarum. She had noted recent weight loss of 4 kg, lethargy and fatigue, but no change in skin pigmentation, and denied salt craving or orthostatic presyncope. Other than an increase in chronic anxiety, her husband had not noted any change in her mental state or cognition. The woman and her husband had migrated from Pakistan to Australia 10 weeks earlier. She denied any significant past history, intake of complementary therapies, medications other than prescribed anti-emetics, or application of skin-lightening creams. On examination, pulse was 80/min regular, and blood pressure was 100/60 mmHg. Investigations on presentation revealed capillary ketonemia, a metabolic acidosis with compensatory respiratory alkalosis, hypokalaemia, normal serum sodium, plasma glucose, lactate, lipase and thyroid function, and a normocytic anaemia with normal iron studies, ferritin, active vitamin B12 and red cell folate with no evidence of haemolysis (Table 1).
Laboratory values on presentation.
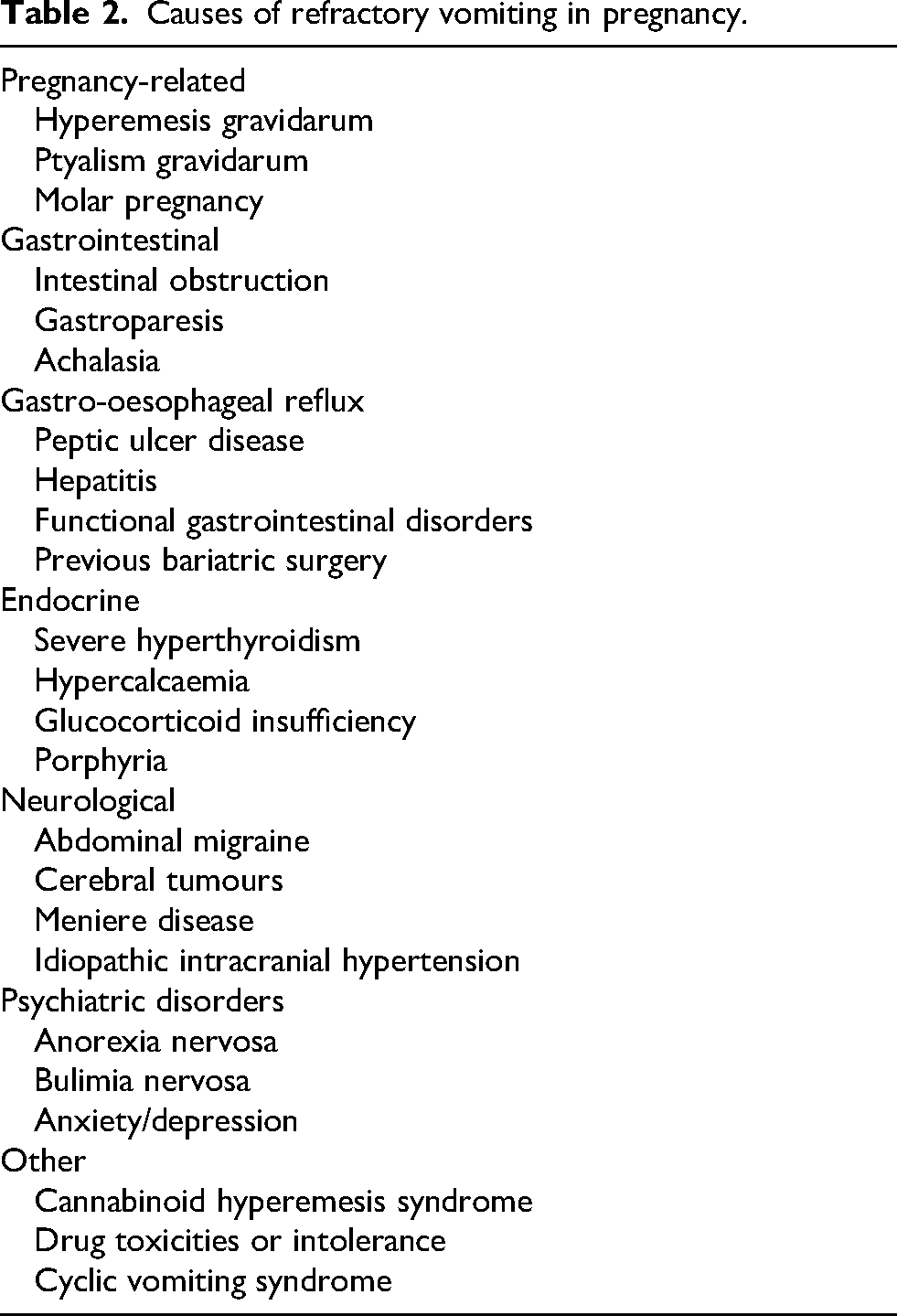
Causes of refractory vomiting in pregnancy.
The woman was diagnosed with starvation ketoacidosis in the setting of hyperemesis gravidarum and commenced on intravenous dextrose and ondansetron, with resolution of ketoacidosis. Further investigation revealed hypothalamic–pituitary–adrenal axis (HPA) insufficiency with a 7 am serum cortisol of 94 nmol/L (normal first trimester 300–900) with ACTH 15 ng/L (non-pregnant 10–50), serum IGF-1 of 5.8 nmol/L (12–36) suggestive of growth hormone deficiency, and lead toxicity with serum lead level of 0.34 umol/L (< 0.24). Serum prolactin was appropriately elevated for first-trimester levels. On further questioning, the woman disclosed the use of a powder she regarded as an Ayurvedic preparation for approximately 2 years, provided by a traditional healer in a neighbouring village in Pakistan. The preparation had been ceased on moving to Australia. The woman denied geophagia/pica and was previously living in a small village in Pakistan, where water and soil were unlikely to be contaminated with heavy metals. An attempt to cease the powder approximately 6 months prior to migration had also resulted in severe vomiting and fatigue.
The woman was commenced on prednisone 12.5 mg mane with resolution of nausea and vomiting, improvement in fatigue and anxiety, and subsequent weight gain. Doxylamine and ondansetron were ceased. A toxicology service was consulted and recommended deferring chelation therapy with observation of maternal serum lead levels. The powder the woman had been using was not available for analysis. Eight weeks later, having reduced prednisone to 5 mg mane, her HPA axis had recovered with serum cortisol 558 nmol/L (measured by High Performance Liquid Chromatography to avoid assay interference), IGF1 had risen into the normal range at 13 nmol/L, Hb had improved to 104 g/L, and serum lead level had fallen to 0.23 µmol/L. Prednisone was ceased given recovery of the maternal HPA axis. Fetal ultrasound revealed normal morphology, and serial growth progressed along the 50th centile on scans at 28, 32 and 36 weeks’ gestation. The woman proceeded to a spontaneous vaginal delivery of a healthy female infant, birthweight 3090 g at 38 weeks’ gestation. The baby's serum lead was 0.17 µmol/L. A toxicologist was consulted, who advised that breastfeeding was acceptable, and no treatment of the baby other than ongoing observation of lead levels was indicated.
Discussion
Nausea and vomiting occur in up to 74% of pregnant women, with half experiencing vomiting alone. 1 Causes to consider with refractory vomiting in pregnancy are listed in Table 2.
Hyperemesis in early pregnancy has rarely been reported as the primary presenting feature of previously undiagnosed cortisol deficiency due to Addison disease.2–6 Many of the non-specific features of Addison disease are common in normal pregnancy, including nausea and vomiting, relative hypotension, hyperpigmentation and the physiological fall in serum sodium of 3–5 mmol/L. Factors which should prompt consideration of Addison disease in pregnant women with refractory vomiting include marked weight loss, orthostatic presyncope, increased pigmentation of non-sun-exposed areas, salt craving, hypoglycaemia, hyponatraemia, hyperkalaemia, and a personal or family history of autoimmune disease. The diagnosis of secondary/tertiary cortisol deficiency as a cause of refractory vomiting, fatigue and weight loss may be more difficult to consider as hyperpigmentation does not occur, and as mineralocorticoid production remains intact, hyperkalaemia and salt craving are absent, and there is a lower likelihood of hypotension. A high index of suspicion is therefore required in considering HPA axis insufficiency in women with hyperemesis.
The diagnosis of cortisol deficiency and differentiation of primary and secondary/tertiary insufficiency are affected by the significant progressive physiological increase in maternal serum cortisol and ACTH in pregnancy. In the non-pregnant state, an early morning basal serum cortisol of less than 102 nmol/L is consistent with adrenal insufficiency. 7 A random morning serum cortisol of less than 300 nmol/L in the first trimester, less than 450 nmol/L in the second trimester, and less than 600 nmol/L in the third trimester should raise a clinical suspicion of adrenal insufficiency.8,9 Trimester-specific values for 250 µg synacthen stimulation tests below 700, 800 and 900 nmol/L for first, second and third trimester, respectively, are consistent with adrenal insufficiency, although stimulated salivary free cortisol values may be a more consistent measure of synacthen-stimulated adrenal function in pregnancy. 9 Mean ACTH levels rise approximately 6-fold above pre-conception values during the course of pregnancy. 10 Published cases of newly diagnosed primary adrenal insufficiency in pregnancy reported serum ACTH levels between 678 and 1173 ng/L.2,3,11
Cortisol deficiency may also cause reversible normocytic anaemia and may have been an additional factor, together with lead toxicity, in causing anaemia in the case presented.2,12
Acute lead toxicity in adults may be associated with anaemia, neuropsychiatric manifestations (anxiety, depression, poor concentration, encephalopathy, seizures) and gastrointestinal symptoms (anorexia, abdominal pain, constipation, nausea, vomiting), as well as marked fatigue and sleep disturbance. Chronic exposure may result in tremor, hearing loss, sensorimotor neuropathy, psychiatric symptoms, neurocognitive decline, hearing loss, anaemia, nephropathy, infertility, and an increased risk of hypertension, ischaemic heart disease, and overall mortality.13–15
Ayurvedic lead poisoning results in a greater haemoglobin decrement of 36.2 g/L than lead paint intoxication, postulated to be due to late presentation and co-exposure to arsenic in 25% of Ayurvedic cases. 16 Seventy-five per cent of Ayurvedic-poisoned patients with blood lead 1.93–3.86 µmol/L had haemoglobin values less than 100 g/L. 16
A correlation has been previously demonstrated between low serum IGF-1 levels and elevated blood lead levels in children and adolescents with short stature and growth hormone deficiency, even with low-level lead exposure.17,18
Maternal blood lead concentration is a major risk factor for preeclampsia, even at low blood lead levels. 19 A meta-analysis found that an increase in blood lead of 0.048 µmol/L was associated with a 1.6% increase in the likelihood of preeclampsia. 20
Lead freely crosses the placenta, and even slight elevation in maternal blood lead levels may be associated with fetal toxicity, resulting in adverse effects on neurodevelopment, reduced fetal growth, and increased risk of miscarriage and premature birth. 21
Lead is secreted in breast milk, and mothers with a blood lead level greater than 1.93 µmol/L should not breastfeed. 22
The relative contributions of glucocorticoid deficiency following withdrawal of the ayurvedic preparation, chronic lead toxicity, and pregnancy alone to the woman's symptoms of vomiting, weight loss, fatigue and anxiety are unclear. Glucocorticoid therapy may be effective in many aetiologies of nausea and vomiting, including hyperemesis gravidarum. The development of similar symptoms 6 months prior to presentation when non-pregnant, and rapid resolution with a relatively small dose of prednisone during pregnancy, suggests glucocorticoid deficiency was likely to be a significant factor. This case emphasises the importance of asking individuals about historical use, and not just current use of complementary preparations, given the development of HPA axis insufficiency following cessation of the preparation, and the ongoing effects of chronic lead exposure.
Ayurveda, a traditional system of medicine, has been widely practised in South Asia since the 2nd century BC. 23 Ayurvedic medications are primarily composed of herbs, animal products, and a small amount of heavy metals, in particular lead, arsenic and mercury. 24 Due to the practice having been passed from generation to generation, and the perception of the composition of Ayurvedic preparations being of ‘natural’ origin, they are often regarded as being ‘safer’ medicines. Traditional healers, however, may provide powders adulterated with drugs and heavy metals in the name of Ayurvedic medicine. 25
It has been estimated that more than 80% of the developing world's population use complementary and alternative systems of medicine (CAM), while approximately half of the population in industrialised countries use CAM. 26 Multiple analytic studies have demonstrated adulteration of CAMs, including up to 100% of Ayurvedic medications in India being adulterated with toxic levels of heavy metals in some studies, and 39% adulterated with glucocorticoids (Table 3).
Analytical studies of adulteration of complementary products.
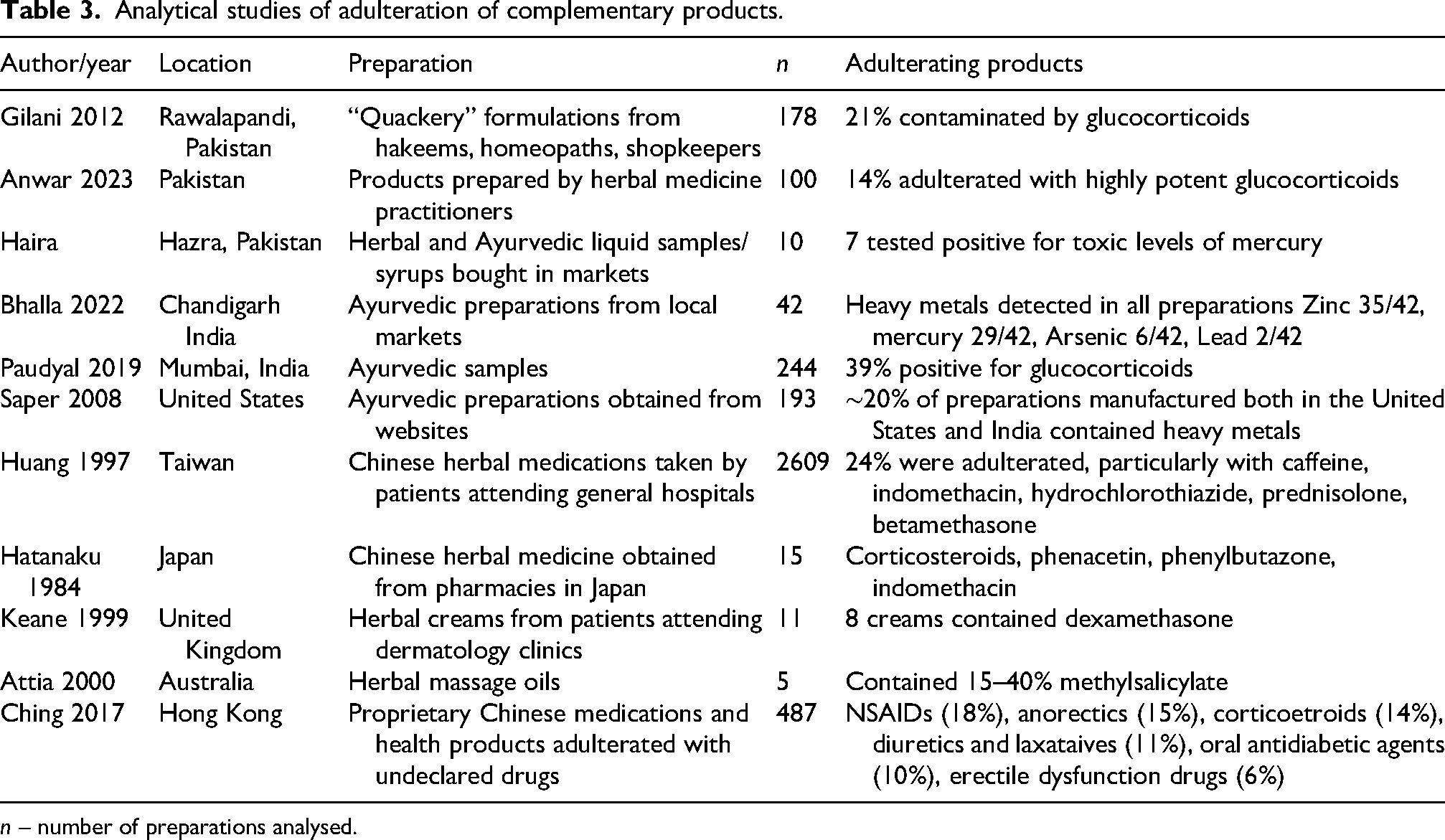
n – number of preparations analysed.
A retrospective chart review conducted on all deliveries at a hospital in New York City between 1999 and 2005 (the first 6 years after initiation of universal screening) found the prevalence of lead toxicity to be 1.7%. 27 None of the affected women were born in the United States, with 46% immigrating to the US while pregnant. Most common maternal birthplaces were Mexico (45%), Pakistan (27%), India (7%) and Bangladesh (9%). Duration of residence in the US was less than 6 months in 39%, 6–12 months in 7%, 13–24 months in 14%, and more than 24 months in 40%.
During 2011–2012, the New York City Department of Health and Mental Hygiene investigated six cases of lead poisoning in foreign-born pregnant women associated with the use of 10 oral ayurvedic preparations made in India. 28
The American College of Obstetrician and Gynecologists include the use of alternative or complementary substances, herbs or therapies traditionally used by East Indian, Indian, Middle Eastern, West Asian and Hispanic cultures that may be contaminated by lead among the risk factors for lead exposure in pregnant and lactating people. 29 Some authors advocate for universal lead testing in pregnancy. 29
Skin-lightening creams, commonly used during pregnancy in western Africa and South Asia, may also be adulterated with highly potent glucocorticoids, mercury and hydroquinone.
The use of herbal medicines in pregnancy is also common globally. A study of 9483 women in Europe, North America and Australia found that 29.3% of women reported using herbal medicine during pregnancy. 30 A prospective cohort study in China found that 45% of mothers consumed Chinese herbal medicines during pregnancy and the postpartum period. 31 Ethnobotany studies found that medicinal plants were consumed during pregnancy by 90% of women in Eastern Ivory Coast and 80% of women in Mali.32,33 It is commonly reported that migrant women transfer cultural practices to their new country.
A meta-analysis of global studies revealed a 67% non-disclosure rate for biologically based CAM to medical providers. 34
Exposure to cadmium, mercury and arsenic during pregnancy may be associated with low birthweight. 21 Cadmium exposure is also associated with increased risk of preeclampsia, arsenic exposure may be associated with reduced birth length and head circumference, and exposure to mercury may be associated with abnormal anthropometric measurements at birth. 35
Conclusion
Awareness of the high prevalence of use of complementary and alternative systems of medicine, the potential for adverse effects due to adulteration of preparations, and possible non-disclosure of their use is important for health care professionals caring for women in pregnancy.
Footnotes
Ethical approval
Ethical approval was provided by Mater Health Human Research and Ethics Committee QACR/MML/116423 (V1).3
Informed consent
Written informed consent was provided by the patient for publication of this article.
Contributorship
AM cared for the patient, researched, wrote and reviewed the manuscript.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
AM.