
Abstract
β-thalassemia minor is associated with high rates of anaemia developing in pregnancy, possibly related to a blunted erythropoietin response. Anaemia with an inadequate erythropoietin response has been demonstrated in non-pregnant individuals with autonomic neuropathy with normal renal function. A case of mild anaemia in pregnancy with severe orthostatic symptoms in a woman with β-thalassemia minor and possible postural orthostatic tachycardia syndrome, with rapid resolution of symptoms and improvement in anaemia with darbepoetin therapy is described. The potential role of erythropoietin-stimulating agents in the management of symptoms in pregnancy-related anaemia in thalassemia minor is discussed.
Introduction
Thalassemia minor is associated with increased rates of fetal growth restriction, low birth weight, fetal distress, neonatal asphyxia and oligohydramnios.1–3 β-thalassemia minor is associated with high rates of worsening anaemia in pregnancy, possibly related to a blunted erythropoietin (EPO) response to anaemia. A blunted EPO response to anaemia has also been demonstrated in autonomic neuropathy due to type 1 and type 2 diabetes mellitus, pure autonomic failure, multisystem atrophy and amyloidosis in non-pregnant individuals with normal renal function.4–7 The potential role of erythropoietin stimulating agents in the management of symptomatic anaemia in pregnant women with β-thalassemia or autonomic neuropathies is discussed.
Case
A 39-year-old woman of Cypriot ethnicity was referred to medical antenatal clinic at 31 weeks’ gestation in her fourth pregnancy because of disabling orthostatic presyncope, syncope, palpitations and dyspnoea impairing activities of daily living. Her history was significant for β-thalassemia minor, an episode of nephrolithiasis, and hypermobility with recurrent shoulder and patella dislocations. The woman's haemoglobin (Hb) had been 110 g/L at 6 weeks’ gestation. (Figure 1) She had first noted orthostatic symptoms at 23 weeks’ gestation when Hb was 94 g/L, serum ferritin was 32 ug/L (normal 30–250), transferrin saturation was 26% (20–45), serum creatinine was 38 umol/L (30–77) and reticulocyte count was 2.6% (< 3%). Active vitamin B12, red blood cell folate, thyroid function, lactate dehydrogenase and serum bilirubin were normal.
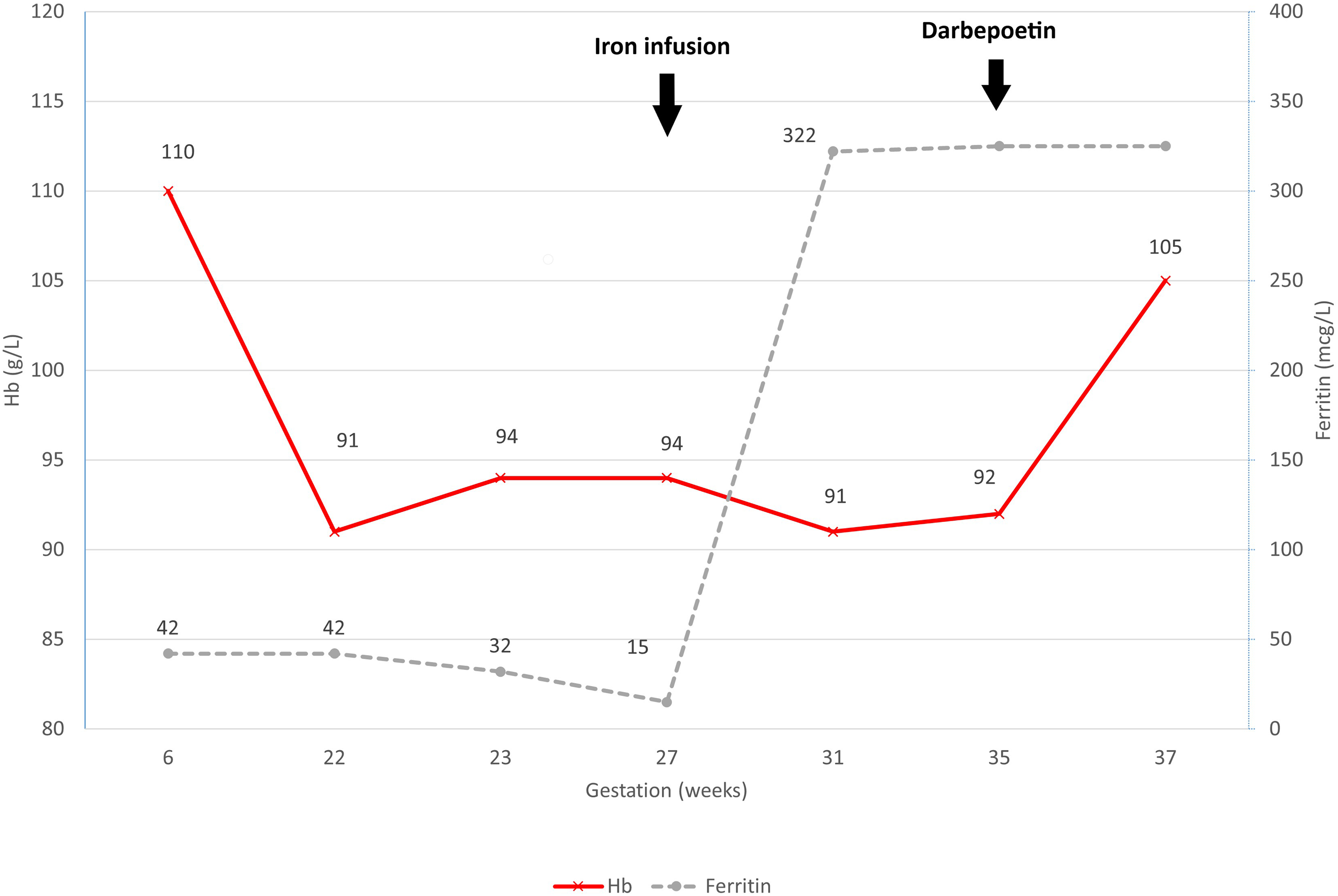
Progression of haemoglobin and serum ferritin during pregnancy.
The woman commenced oral iron supplements; however developed gastrointestinal side-effects. Intravenous ferric carboxymaltose 1000 mg was administered at 27 weeks’ gestation without improvement in Hb, and progressive orthostatic symptoms resulted in repeated presentations to the pregnancy assessment unit and a brief hospital admission during which electrocardiographic telemetry excluded arrhythmia during episodes of presyncope.
Examination revealed a slim woman (pre-pregnancy body mass index 18 kg/m2) with evidence of hypermobility but no other features of Ehlers-Danlos or Marfan syndromes. Pulse was 80/min sitting and 110/min after standing for 45 s associated with presyncope, palpitations and visual disturbance with blood pressures of 110/80 mm Hg without a postural drop. The woman denied any other symptoms of dysautonomia other than chronic constipation. Heart sounds were dual without signs of valvular pathology and neurological examination was normal. Serum cortisol was 466 mmol/L (normal > 300 nmol/L). No symptomatic benefit occurred with water loading, increasing salt intake, other physical manoeuvres, or fludrocortisone 0.3 mg/day. Serum erythropoietin was inappropriately low for the degree of anaemia at 20 mIU/ml. Due to the severity of the woman's symptoms, 40 mg darbepoetin was given subcutaneously at 35 weeks’ gestation following informed consent. Orthostatic symptoms resolved completely within three days, and Hb increased to 105 g/L by 37 weeks’ gestation. (Figure 1) The woman proceeded to spontaneous vaginal delivery of a 2770 g infant following spontaneous rupture of membranes at 38 weeks’ gestation.
Discussion
A study of 347 pregnancies in women with β-thalassemia minor reported Hb less than 90 g /L in 6.9% of women in first trimester, and 31% of women in third trimester. 8 In women with serum ferritin > 50 ug/L anaemia frequently improved in the weeks prior to delivery, with mean Hb rising from 92 g /L in third trimester to 101 g/L at delivery. Antepartum blood transfusion, intravenous iron and erythropoiesis-stimulating agents were administered in 4%, 7.5% and 2% of women respectively. 8 Mean Hb fell to 85 g/L in women postpartum with serum ferritin > 50 ug/L, with 4.3% of women requiring peripartum transfusion, and 8.9% of women having postpartum haemorrhage. 8
During early pregnancy the 40% expansion in plasma volume prompts a 2- to 4-fold rise in erythropoietin (EPO) levels to provide a compensatory increase in red cell mass. A longitudinal study of 263 pregnant women without thalassemia found EPO levels rose from a mean of 22.8 mU/mL at booking to 41.6 mU/ml and 43.7 mU/mL at 32 weeks’ and 38 weeks’ gestation respectively. 9 The correlation coefficient between Hb and EPO was – 0.38. Expansion in red cell mass may be suboptimal in β-thalassemia minor pregnancy due to a blunted EPO response to anaemia. 10 Bianco et al. compared mean EPO levels in women with β-thalassemia and non-thalassemic controls in pregnancy. In first trimester mean EPO levels were 15 mU/ml (paired mean Hb 104 g/L) in women with β-thalassemia minor and 17 mU/L (paired mean Hb 123 g/L) in controls. In third trimester mean EPO levels in women with β− thalassemia minor were 35.6 mU/L (paired mean Hb 97 g/L) and 31.4 mU/L (paired mean Hb 111 g/L) in control women. 11 In non-pregnant individuals with normal renal function the range between 20th and 80th centile of EPO concentrations for four specified Hb levels were EPO 61.8–366 mU/L for Hb < 80 g/L, EPO 43.3–242 mU/L for Hb 81–90 g/L, EPO 31.8–113 mU/L for Hb 91–100 g/L, and EPO 22.3–71.2 mU/L for Hb 101–110 g/L. 12 Thus throughout pregnancy the erythropoietin response to anaemia in individuals with β− thalassemia minor appears to be inadequate.
Bencaiova et al. assessed response to recombinant human erythropoietin (rhEPO) in 19 pregnant women with Hb < 100 g/L with heterozygous haemoglobinopathies (13 β-thalassemia minor, 3 sickle cell trait, 2 alpha-thalassemia minor, 1 heterozygous haemoglobinopathy E). 13 The mean gestational age at the start of therapy was 28 weeks, and mean duration of therapy was 3.5 weeks. Treatment was commenced at three doses of rhEPO 10 000 U intravenously over a 14-day period, with the dose subsequently increased to 20 000 U where the initial increment in Hb was poor. All the women demonstrated an increase in Hb. Requirement for increased dose because of poor initial response was seen in five women with β-thalassemia minor originally from the Mediterranean region. Larger studies investigating the efficacy of erythropoietin-stimulating agents in heterozygous haemoglobinopathies complicated by anaemia in pregnancy would be valuable.
Breymann et al. demonstrated that rhEPO therapy caused an Increase in F reticulocytes (1.5 to 10.5 fold), F cells (5 to 7.7 fold), HbF (1.4–2.2 fold), young immature reticulocytes and Hb in four pregnant patients with β-thalassemia minor and anaemia. 14
Three case reports describing e the use of rhEPO in women with symptomatic anaemia in the setting of β-thalassemia minor and intermedia in pregnancy are summarised in Table 1.
Previous case reports of symptomatic anaemia in β -thalassemia responsive to rhEPO in pregnancy.
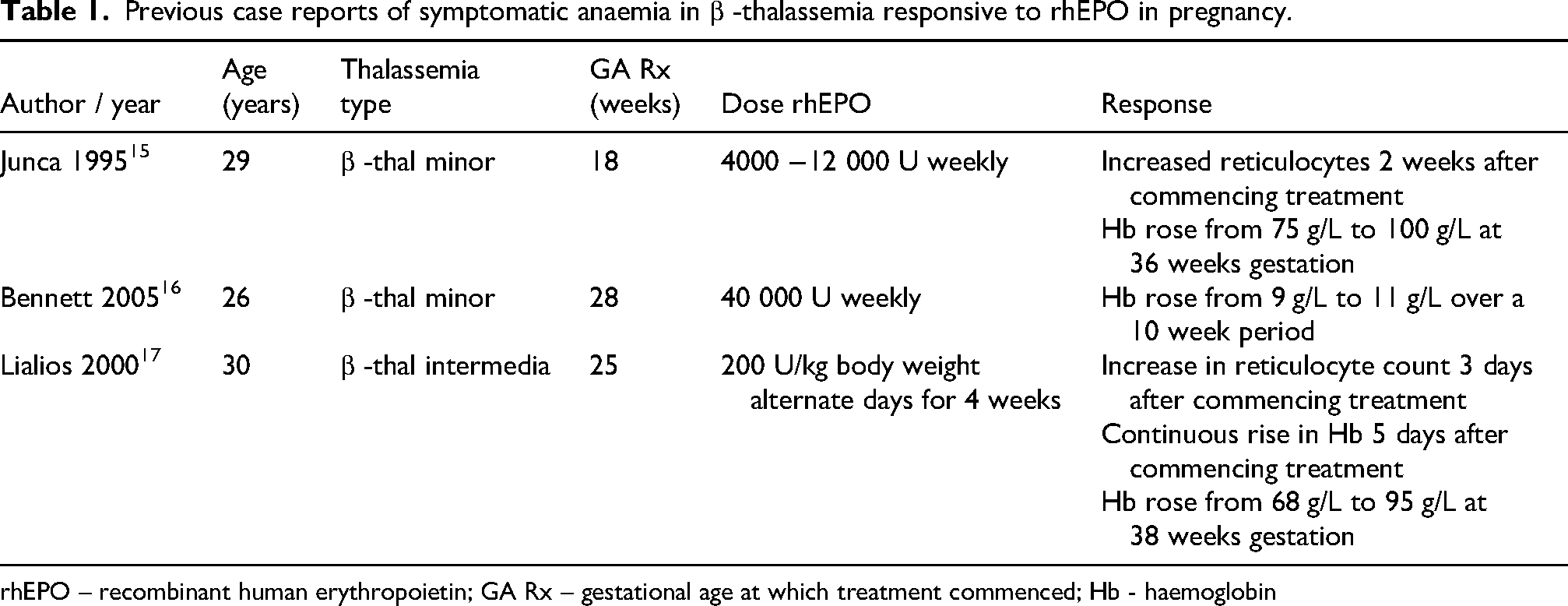
rhEPO – recombinant human erythropoietin; GA Rx – gestational age at which treatment commenced; Hb - haemoglobin
An additional factor in the anaemia and blunted EPO response in the case presented may have been pregnancy prompting the onset of postural orthostatic tachycardia syndrome (POTS) in the setting of a hypermobility spectrum disorder. A large cross-sectional online community-based survey of individuals developing POTS after 18 years of age reported symptoms occurring initially in pregnancy in 9%. 18 There is an association between POTS and joint hypermobility, the overlapping prevalence dependent on the criteria used in the diagnosis of each disorder. Yao et al. found the frequency of joint hypermobility disorders in individuals with POTS to be 13% using strict criteria of hypermobile Ehlers Danlos syndrome and 34% using hypermobile spectrum disorder criteria. 19 A study of 24 adolescents with POTS found a high prevalence of low iron storage and mild anaemia compared with the general adolescent population. 20 A study of non-pregnant POTS patients refractory to other medications found 71% demonstrated symptomatic improvement with erythropoietin therapy. 21 A blunted EPO response to anaemia in the absence of renal impairment has also been demonstrated in dysautonomia secondary to diabetes mellitus, multisystem atrophy and familial amyloidosis, with improvement in orthostatic symptoms and anaemia with erythropoiesis-stimulating therapy.4–6,22–25 In the author's personal experience of treating severe cardiovascular autonomic neuropathy refractory to physical and other pharmacological interventions in anaemic individuals with type 1 diabetes mellitus and normal renal function, the improvement in orthostatic symptoms typically occurs within days of commencement of therapy, preceding any rise in Hb. Erythropoietin administration results in a vasoconstrictive pressor effect, likely mediated by increased release of endothelin-1 by endothelial cells, increase in noradrenaline and free dopamine levels, and elevated resting and agonist stimulated cytoplasmic calcium concentration, which have been demonstrated in tissue, animal and human studies within hours of initial administration.26–29 The pressor effect of erythropoietin occurs independent of anaemia. 26 A similar rise in blood pressure occurs despite persistent anaemia in erythropoietin-treated iron deficient animals and humans. 26 Treatment of anaemia by blood transfusion or iron repletion in severely anaemic iron-deficient patients maintained on constant erythropoietin doses however do not raise blood pressure.
Erythropoiesis stimulating agents do not cross the placenta and have been shown to be safe for mother and fetus in pregnancy.30–34
Conclusion
Blunted erythropoietin response may be a factor in anaemia in pregnant women with thalassemia minor. Anaemia with blunted erythropoietin response has also been described in non-pregnant individuals with autonomic dysfunction. Erythropoiesis-stimulating agents may be useful in cases of symptomatic anaemia refractory to other therapies in iron-replete pregnant women with thalassemia minor and/or dysautonomias, improving symptoms and avoiding the need for transfusion of blood products. Larger studies examining the potential role of erythropoiesis-stimulating agents in the management of symptomatic anaemia with thalassemia minor and/or dysautonomias would be of value.
Footnotes
Ethical approval
Was waived by Mater Health Human Research and Ethics Committee.
Informed consent
Written informed consent was provided by the patient for publication of this article.
Author contributions
AM cared for the patient, performed a literature review, and wrote the manuscript.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Adam Morton