
Abstract
We report the case of a 32-year-old pregnant woman who presented at 9 weeks of gestation with severe hyperemesis gravidarum (HG) and metabolic disturbances. Biochemical testing revealed hypercalcemia with an inappropriately elevated parathyroid hormone (PTH) level. Subsequent imaging identified a parathyroid adenoma. This case highlights primary hyperparathyroidism as a rare but important differential diagnosis in refractory HG and underscores the diagnostic challenges of interpreting calcium and PTH values during pregnancy.
Keywords
Case report
A 32-year-old woman pregnant with twins, conceived via in vitro fertilization, was admitted at 7 weeks of gestation with severe nausea and vomiting of pregnancy (NVP) in the primary hospital. When she was transferred to the tertiary center, she reported weight loss of 10 kg since conception and was considering termination of pregnancy due to the severity of symptoms of hyperemesis gravidarum (HG). Clinical examination revealed dehydration, tachycardia and mild hypotension. The Pregnancy-Unique Quantification of Emesis and Nausea (PUQE) score indicated moderate to severe levels of HG. When she was first referred for a nephrology consultation, laboratory results showed a hypokalemic metabolic alkalosis (K 2.8 mmol/l, Na 133 mmol/l, pH 7.45, base excess +6, bicarbonate 30 mmol/l). The patient had normal kidney function for the first trimester (creatinine 0.4 mg/dL). Both urine chloride (103 mmol/l) and potassium/creatinine ratio in urine (9.6 mmol/mmol) were elevated. However, the patient was already receiving intravenous potassium chloride supplementation at this point, which rendered the urine values usable only to a limited extent. Recurrent vomiting was considered the most likely cause of metabolic alkalosis, leading to secondary renal potassium wasting. Moreover, both albumin-corrected serum calcium and ionized calcium were raised at 2.55 mmol/l and 1.38 mmol/l, respectively (see Table 1 for reference ranges). Parathyroid hormone (PTH) was within the lab reference range at 55 pg/ml in non-pregnant females and remained in this range in subsequent laboratory tests. Differential diagnoses included calcium-alkali-syndrome, familial hypocalciuric hypercalcemia (FHH), and primary hyperparathyroidism (pHPT). Calcium-alkali-syndrome was initially suspected due to ingestion of antacids and calcium-containing pregnancy vitamins; however, it was considered unlikely due to normal kidney function and the lack of PTH suppression. Urine analysis demonstrated increased fractional excretion of calcium (FECa), making a diagnosis of FHH unlikely. Based on normal pre-pregnancy potassium values and the elevated FECa, primary salt-wasting nephropathies such as Gitelman syndrome were deemed unlikely. The patient's previous calcium levels were not available. Repeated sonographic assessments of the thyroid and parathyroid gland did not show any adenomas or other focal lesions.
Patient values, local laboratory reference range and published reference ranges for total and ionized calcium and parathyroid hormone. Note that in the local hospital ionized calcium is not measured by the central local laboratory but by blood gas analyzers.
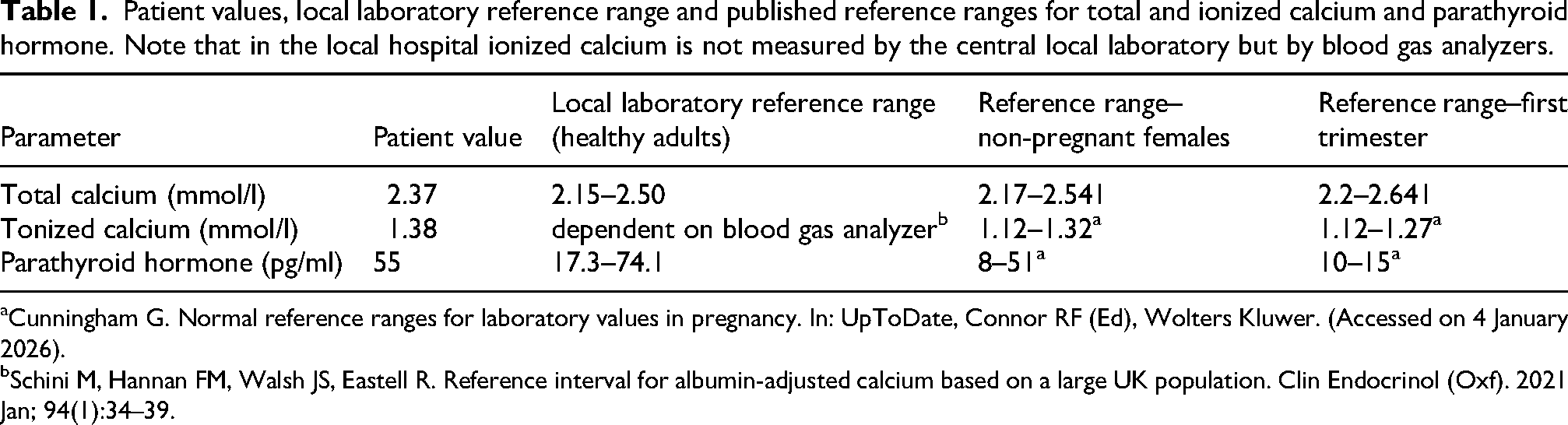
Cunningham G. Normal reference ranges for laboratory values in pregnancy. In: UpToDate, Connor RF (Ed), Wolters Kluwer. (Accessed on 4 January 2026).
Schini M, Hannan FM, Walsh JS, Eastell R. Reference interval for albumin-adjusted calcium based on a large UK population. Clin Endocrinol (Oxf). 2021 Jan; 94(1):34–39.
The patient received intravenous fluids, potassium replacement, antiemetic therapy, thiamine supplementation, and psychological support. Potassium and blood pH normalized; however, calcium levels remained elevated. Neurologic and gastrointestinal evaluations were performed, and no abnormalities were identified. Despite the resolution of symptoms, the patient opted to proceed with the termination of pregnancy. Following termination, serum calcium and PTH levels increased further.
The patient underwent a 99mTc-methoxyisobutylisonitrile (99mTc-MIBI) scintigraphy, which did not demonstrate any significant abnormalities. An 18F-Choline PET/CT identified a choline-positive lesion right, posterior to the trachea, indicative of a parathyroid adenoma (Figure 1). A second choline-positive area was detected in the right head of the humerus, considered suspicious for a Brown tumor, this finding was further evaluated with magnetic resonance imaging and subsequently managed conservatively. Genetic testing for mutations associated with multiple endocrine neoplasia, FHH, and salt-wasting nephropathies did not identify any pathogenic variants at the moment. The patient subsequently underwent successful parathyroidectomy and thereafter calcium and PTH levels returned to normal.
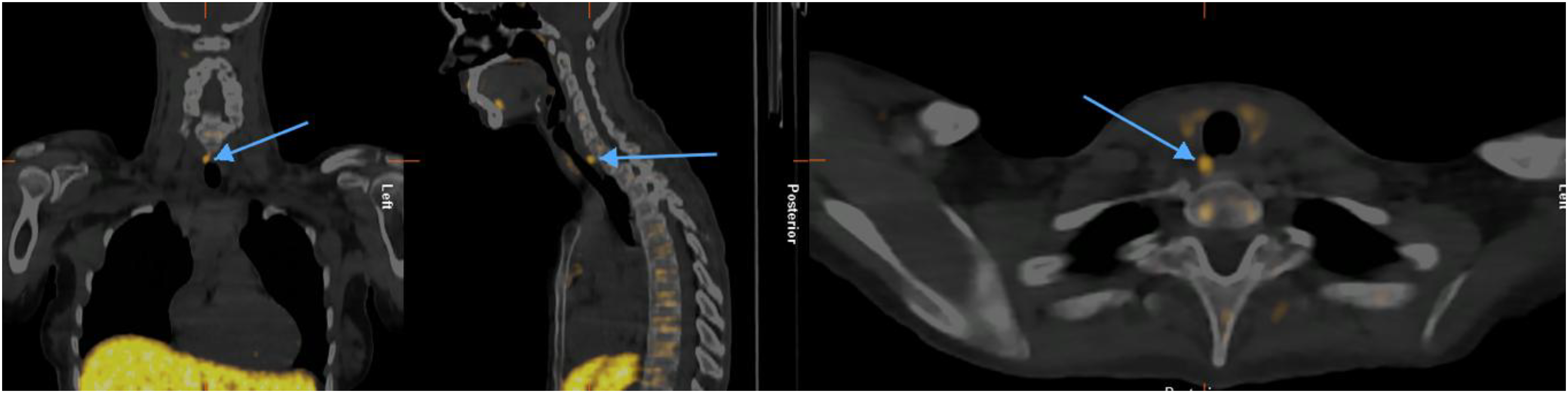
Coronal, sagittal and axial (from left to right) 18F-Choline PET/CT slices show right tracheoesophageal groove superior parathyroid adenoma (arrow), located posterior to the trachea.
Discussion
HG affects around 0.5–3.5% of pregnant individuals and is a severe form of NVP. By definition, HG starts in early pregnancy, typically before 16 weeks of gestation, causes symptoms severe enough to impact normal food and fluid intake significantly, and limits activities of daily life. The etiology of HG is multifactorial and not completely understood but likely involves endocrine and genetic causes. Diagnosis of HG does not require specific biochemical parameters. Initial investigations include medical history and physical examination to assess for signs of dehydration, the use of validated scores (PUQE score) to assess severity, urine investigations, complete blood count, glucose, urea and electrolytes. 1 For example, as demonstrated in the case above, the recurrent vomiting can lead to metabolic alkalosis with secondary renal potassium wasting. Refractory cases warrant further investigation, including thyroid function tests, liver function tests, calcium and phosphate levels, amylase and blood gases. Around 40–50% of women show elevated liver test abnormalities and only a marked increase of transaminases requires screening for primary liver diseases. An ultrasound should be carried out to assess for a viable intrauterine pregnancy. 2 Up to 25% of patients with HG are affected by mental health disorders, including depression, suicidal thoughts and post-traumatic stress disorder. Additionally, termination of pregnancy is performed in up to 5% of wanted pregnancies due to the severity of symptoms. Early mental health assessment and appropriate referrals to mental health services should take place. 1
Nausea and vomiting are frequent symptoms of hypercalcemia, which is frequently caused by pHPT. 3 Diagnosis of pHPT during pregnancy can be challenging due to its non-specific symptoms, which may be falsely attributed to pregnancy itself, physiological changes in pregnancy and pregnancy-specific reference ranges must be considered.
Pregnancy causes a physiologic lowering of total calcium concentrations due to plasma volume expansion, while albumin-corrected serum calcium and ionized (free) calcium remain within the normal range and can be used for diagnostic reasoning in pregnancy. 4 Initial investigation of hypercalcemia includes measuring PTH levels to distinguish between PTH-dependent and PTH-independent causes. PTH levels decrease in early pregnancy because PTH-related peptide levels, derived from the placenta and breasts, increase and act as the main regulatory hormone for calcium during pregnancy. The reference range for PTH in the first trimester is between 10–15 pg/ml according to literature, hence elevated or inappropriately normal PTH levels should raise concern for pHPT or FHH. 5 However, PTH measurement using immunoassays is vulnerable to interferences due to e.g. heterophile antibodies. This should be taken into account particularly in cases of isolated PTH elevation without abnormalities in kidney function, vitamin D, calcium, and phosphate levels. 6 Measuring FECa can be used to differentiate between FHH (<0.01) and pHPT (>0.02). However, maternal estrogen and 1,25-dihydroxyvitamin D stimulate increased intestinal absorption of calcium to support the demands of the growing fetal skeleton. This leads to elevated 24-h urinary calcium excretion during pregnancy making it a less reliable clinical test. 7
Differential diagnoses for hypercalcemia with suppressed PTH include granulomatous diseases, malignancies, vitamin D intoxication and calcium-alkali-syndrome. 3 The latter presents as a triad of hypercalcemia, alkalosis and acute kidney injury resulting from the ingestion of calcium supplements and absorbable alkali. Heartburn associated with NVP/HG may lead to increased antacid use and potentially trigger the calcium-alkali-syndrome. 8 Gitelman syndrome, a primary salt-wasting nephropathy, typically presents as chloride-insensitive hypokalemic metabolic alkalosis with hypomagnesemia and hypocalciuria. Physiologic increase in urinary calcium excretion may therefore mask this diagnosis. Pre-pregnancy electrolyte levels, evaluation of family members and genetic testing can help differentiate between FHH, pHPT and other tubular disorders during pregnancy. 7
Biochemical abnormalities suggestive of pHPT warrant neck ultrasonography as the first-line investigation to evaluate for a parathyroid adenoma. However, ultrasonography has significant limitations in preoperative localization. If surgery is planned, additional imaging, such as 99mTc-MIBI scintigraphy and/or 18F-Choline PET-CT, should be considered. The risk of radiation exposure with any imaging technique should be weighed against its potential benefits and guided by indication for surgery. 9 Mild hypercalcemia may represent an incidental finding and can be managed conservatively with oral or intravenous fluid replacement, reduced oral intake of calcium, and further evaluation after pregnancy. Observational data show an increased risk of fetal and maternal complications – including miscarriages, intrauterine growth restriction, preeclampsia, nephrolithiasis and pancreatitis – with rising serum calcium concentrations. Parathyroidectomy is recommended in the second trimester if corrected calcium levels remain above 2.85 mmol/l and/or ionized calcium is above 1.45 mmol/l. A systematic review including 382 women with pHPT demonstrated lower infant complication rates for surgery vs. conservative therapy, hence medical management should only be considered as a bridge to surgery. 10 There is evidence for the safety of the use of cinacalcet during pregnancy based on case reports; however, it is not licensed. Calcitonin and bisphosphonates are not recommended. 9
Conclusion
In severe and/or refractory cases of HG, secondary causes should be evaluated. Pregnancy-specific reference values for PTH must be considered when investigating hypercalcemia in pregnancy. Elevated or inappropriately high PTH levels should raise suspicion of pHPT. Diagnosis of pHPT via imaging can be difficult and may require 18F-Choline PET-CT.
Footnotes
Acknowledgment
The authors want to appreciate the contribution of NÖ Landesgesundheitsagentur, the legal entity of University Hospitals in Lower Austria, for providing the organizational framework to conduct this research. The authors also would like to acknowledge support by the Open Access Publishing Fund of Karl Landsteiner University of Health Sciences, Krems, Austria
Ethical approval
Ethical approval was not required for this case report, as it is based on a retrospective analysis of anonymized clinical data.
Informed consent to participate
Written informed consent was obtained from the patient for the publication of anonymized information and any related images in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data that support the findings of this case report are available from the corresponding author upon request.
Declarations
Birgit Pfaller guarantees the manuscript's accuracy and the contributorship of all co-authors.
Gurantor
Birgit Pfaller.