
Abstract
Objectives
Little is known about the impact of premature delivery on maternal renal complications. This systematic review aimed to evaluate the association between earlier delivery and long-term renal health in the pregnant population.
Methods
A comprehensive database search was performed. Eligible studies included cross-sectional and cohort studies that reported preterm and full-term deliveries and subsequent maternal chronic kidney disease. A random-effects meta-analysis was used to calculate the pooled effect estimates. The Newcastle–Ottawa scale was used to assess the risk of bias.
Results
Nine studies met the inclusion criteria. Preterm delivery was associated with long-term maternal renal disease with a pooled odds ratio (OR = 1.82, 95% CI: 1.17–2.85, p = 0.01). A sensitivity analysis identifying outlier study, and the pooled OR excluding it (OR = 2.16, 95% CI, 2.06–2.62; p < 0. 001, I 2 = 0.0%).
Conclusion
Preterm delivery is associated with a significant risk of long-term maternal renal disease. This suggests the need for careful postnatal risk management in this population.
Précis
Preterm delivery is associated with higher risk of long-term maternal renal disease, warranting targeted postnatal care and further research into underlying biological mechanisms and preventive strategies.
Introduction
Background
Premature birth remains a major global health concern due to its association with neonatal mortality, morbidity, and long-term outcomes. According to the World Health Organization (WHO), over 13 million babies were born prematurely in 2020, 1 representing over 13 million pregnant individuals at risk. While the association between prematurity and neonatal morbidity, such as long-term kidney disease in neonates, is well established in the literature, 2 long-term maternal complications associated with preterm delivery are less well understood. 3
In recent years, research evidence has expanded to investigate the long-term maternal health impacts following delivering preterm, shifting our understanding of preterm delivery from solely a neonatal outcome to a marker of future maternal health risk. Delivery before 37 weeks has been found to be associated with long-term maternal cardiovascular disease (CVD). 4 For instance, Kessous et al. found that women who delivered prematurely had higher rates of cardiovascular events, with a linear association between the number of early deliveries and future CVD. 5 Similarly, an observational study by Theilen et al. 6 linked preterm delivery to all-cause and some cause-specific mortality. Beyond cardiovascular disease, Catove et al. reported that women with a history of preterm delivery are at an increased risk of developing metabolic syndrome, and the risk remained elevated, independent of the metabolic risk pre-pregnancy. 7 Collectively, these data suggest that preterm delivery may pose a broader risk to long-term health.
Pregnancy and its events place substantial physiological demands on the maternal kidney due to marked hemodynamic changes and an enhanced glomerular filtration rate. 8 Pre-existing maternal conditions or adverse pregnancy outcomes, particularly preeclampsia, have been linked to long-term maternal kidney disease,9,10 likely due to the loss of the adaptation mechanism, dysregulation of the renin-angiotensin-aldosterone system, and endothelial damage at the nephron level. 11 Whether preterm delivery contributes to similar renal pathophysiological mechanisms is yet to be established. Inflammation may be a potential mechanism underlying this association. Both CKD 12 and preterm delivery have been hypothesized to involve pro-inflammatory pathways, 13 and since pregnancy often shows a significant increase in pro-inflammatory cytokines and C-reactive protein (CRP), this could be a mechanism. 14
The association between preterm delivery and chronic kidney disease has been linked in recent population-based observational studies.9,15,16 17 They demonstrated that women who experience preterm delivery (mainly spontaneous and after accounting for preeclampsia) may be at an increased risk of CKD and ESRD later in life.
This systematic review aims to evaluate the most up-to-date evidence on the association between preterm delivery and long-term maternal renal health outcomes by synthesizing raw data to provide more accurate clinically relevant risk estimates.
Methods
Sources
This systematic review and meta-analysis were prospectively registered (PROSPERO: CRD420251040336), designed, and conducted using standard methods recommended by the Cochrane Collaboration, 18 and the findings are reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplement 1). This study did not require ethical approval.
A comprehensive systematic literature search of data across four electronic databases (EMBASE, Medline, ClinicalTrials.gov, and CIANHL) was conducted on April 30, 2025. The search was limited to English-language publications with no restrictions on publication date or type. The search strategy combined Medical Subject Headings (MeSH) terms and free-text keywords, combining maternal long-term kidney disease and preterm delivery as the search terms. The search strategy was conducted and refined with the consultation of a medical librarian to ensure comprehensive coverage and validated against pre-selected key articles to ensure sensitivity. Search terms were adapted according to each database's requirements and syntax, and additional studies were added through a manual review of the reference lists of relevant studies. Complete details of the full search strategies and review protocols are provided in Supplement 2.
Study selection
Studies were considered eligible if they reported mothers who delivered before term as an exposure and subsequent long-term maternal renal outcomes (CKD or ESRD) as the outcome. Studies were required to report comparison groups of birthing at term (≥37 weeks of gestation) and preterm delivery (<37 weeks) with subsequent kidney disease assessment. Studies were included if they reported postpartum follow-up for any duration. Singleton or multiple pregnancies were included in the study. Studies involving populations without preexisting kidney disease were included to accurately measure the association between earlier delivery and maternal renal outcomes and to assess the impact of pregnancy complications. For the quantitative meta-analysis, studies were eligible if they provided raw data (event counts) for women who delivered prematurely, whether spontaneous or iatrogenic vs full term deliveries and subsequent development of kidney disease. All types of observational studies were included: cohort studies, case-control studies, and randomized controlled trials published in English. There were no restrictions on the publication dates of the articles.
Studies were excluded if they did not report a comparison group, did not report long-term maternal outcomes, or only illustrated neonatal or infant outcomes without maternal outcomes. Case reports, systematic reviews, meta-analyses, editorials, conference abstracts, and study protocols were also excluded.
After duplicates were removed, blinded abstract and title screenings were conducted independently by two reviewers (ES and MH) according to the inclusion and exclusion criteria. Studies that were deemed eligible were retrieved and compared, with any discrepancies discussed and resolved. Following the confirmation of eligible studies, full-text review and data extraction were performed by two reviewers (ES, MA). A bespoke spreadsheet was created to extract data.
For each study, the following information was extracted: study characteristics (author, year, country, design), sample size, population characteristics (age, parity, ethnicity, and comorbidities), exposure definition (categorization of preterm birth), outcomes (CKD-ESRD), follow-up duration, effect estimates [e.g., hazard ratios, odds ratios (OR), risk ratios], and adjustment variables. Raw data was extracted where available. The data extraction sheet is presented in Supplement 3.
Quality assessment
The methodological quality and risk of bias were assessed independently using the Newcastle–Ottawa Scale (NOS) for cohort and case-controlled studies. A score was assigned based on these three domains: selection (maximum 4 points), comparability (maximum 2 points), and exposure (maximum 3 points), with a total possible score of 9. Studies scoring 7–9 points were considered high quality, 5–6 points moderate quality, and 0–4 points low quality. 19 .
Data analysis
The descriptive study characteristics, including country, sample size, and follow-up duration, were summarized. The prevalence of preterm delivery and CKD rates was reported across studies. For studies reporting raw data (event counts), unadjusted ORs with 95% confidence intervals (CIs) were calculated. Studies reporting adjusted effect estimates and raw data that could not be extracted were reported separately in the narrative synthesis.
A meta-analysis of the included studies with raw data and controls was performed using a random-effects model with STATA SE 18 (Stata Corp LLC, Collage Station, TX, USA) to calculate pooled estimates of the association between preterm delivery and maternal renal insufficiency. A random effect model was selected a priori due to anticipated clinical and methodological heterogeneity across the studies. A forest plot was generated to display the individual study results and pooled estimates with a 95% CI. Heterogeneity was assessed based on I-squared and Tau-squared statistics. I2 values of 0–25%, 26–50%, 51–75%, and >75% indicated low, moderate, substantial, and considerable heterogeneity, respectively.
We selected to report effect measures as OR with 95% CI calculated from raw data. OR was preferred to hazard ratio (HR) as it provides a direct estimate of risk with unadjusted data and compares the events of kidney outcomes in women who delivered preterm versus those who delivered at term. While in the HR assumption, the risk is constant over time, this is not likely plausible for the onset of CKD, which can occur at varying time points over decades. 20
Pooling hazard ratios using meta-analysis may lead to invalid results, especially when individual patient data is not available. 21 Instead, studies that included only HR, not raw data, will be evaluated qualitatively to strengthen the overall analysis of the systematic review.
Sensitivity analysis was conducted to explore potential sources of heterogeneity, and the “leave-one-out” method was used to identify potential outliers.
Publication bias was assessed using funnel plots; however, because of the limited number of studies included in the meta-analysis, the power of the tests was too low to reliably detect asymmetry. Funnel plots and formal tests (such as Egger's test) require a minimum of ten studies to have adequate statistical power. 17
Results
The initial database search across Embase, Medline, CINAHL, and ClinicalTrials.gov identified unique 3280 records. After the removal of duplicates, 3023 records were screened based on their titles and abstracts, and 3003 records were excluded. The remaining 20 articles were retrieved for full-text review. Nine studies met the inclusion criteria for qualitative synthesis,10,15,16,22–28 with six providing raw data suitable for meta-analysis. One study (Sandvik et al., 2010) 24 was excluded from the meta-analysis as it reported the same dataset over a similar time period as Viske et al. (2008) 16 to avoid duplication of cases. The complete selection process is detailed in the PRISMA flow diagram (Figure 1).
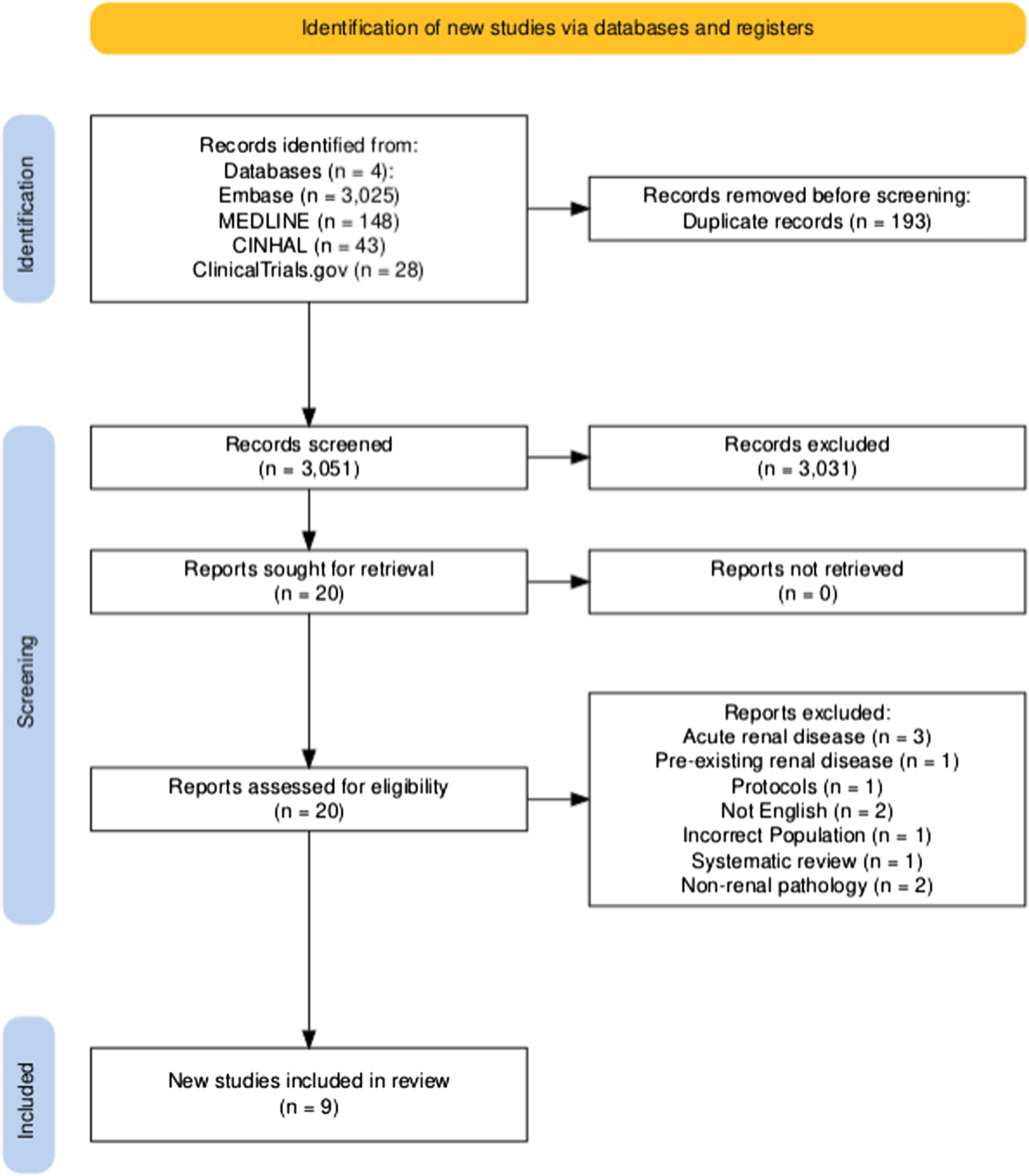
PRISMA flow diagram of study selection.
Study characteristics
Table 1 presents a summary of the nine included studies. Eight were cohort studies, and one was a cross-sectional study. The studies included were published between 2006 and 2024. The sample included over 8.3 million participants from seven countries (Norway, Sweden, Germany, Canada, the Netherlands, Iran, and Israel). The studies ranged from cross-sectional to longitudinal population-based cohorts, with follow-up extending up to 46 years.
Summary table and overview of included studies examining maternal kidney disease following preterm birth.
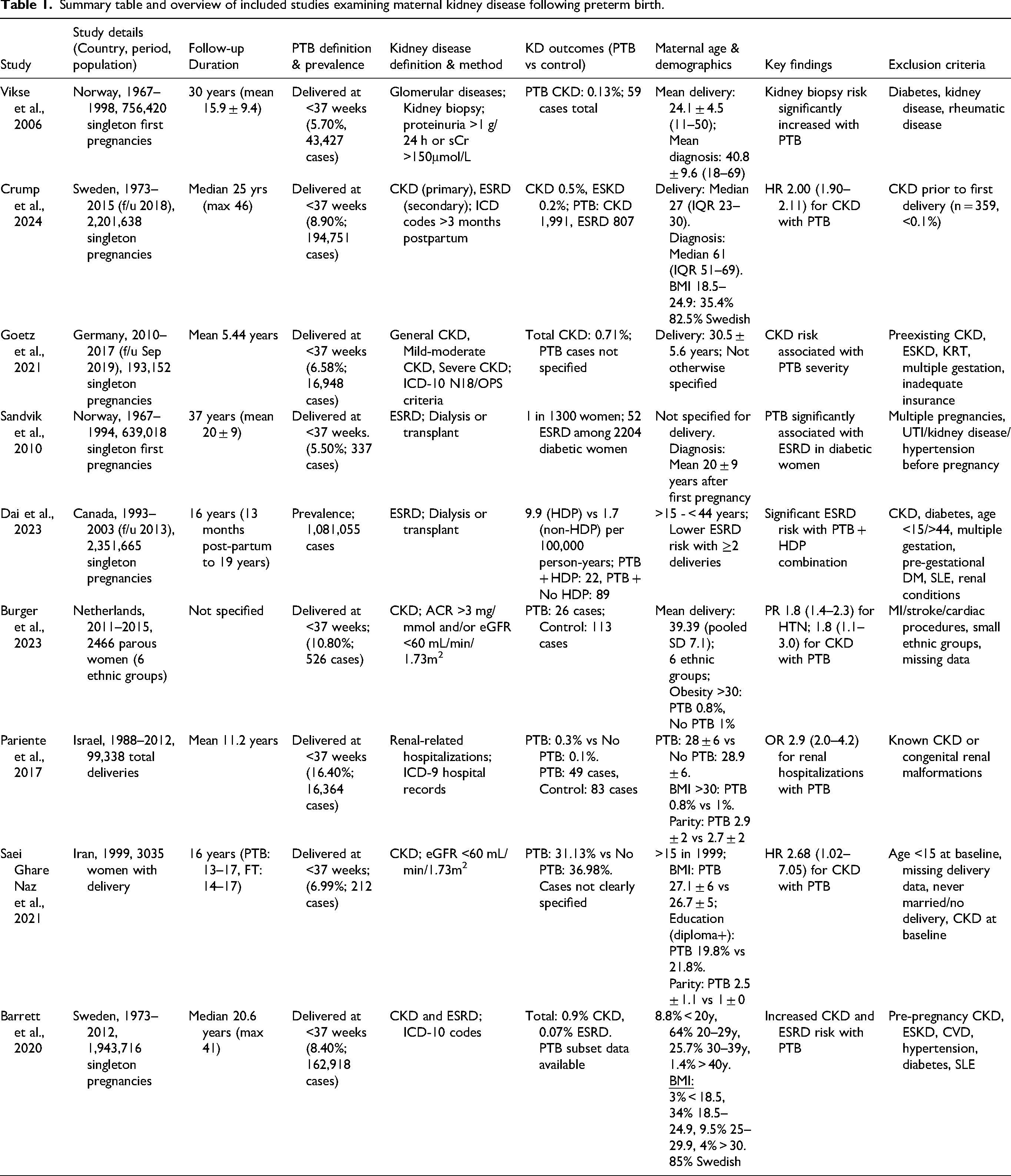
The three largest studies were population-based cohorts, two from Sweden (Crump et al., 2024 and Barret et al., 2020)9,28 examining 4 million participants, and one from Canada (Dai et al., 2023) 25 with 2.4 million participants. The sample size ranged from 2466 women in the Netherlands multi-ethnic cohort (Burger et al., 2023) to over 2 million in the Swedish national cohorts.
Follow-up duration (time from delivery to maternal chronic kidney disease development) also varied among the studies, from 5.44 years (Goetz et al., 2021) 23 to a maximum of 46 years reported from Crump et at. 22 Postpartum follow-up commenced as early as 3 months after delivery; two studies reported waiting for 13 months postpartum to exclude any residual effects of pregnancy on kidney function. Some studies reported durations as mean and standard deviation (SD), while others reported them as a range; therefore, direct comparisons between studies were not possible.
The eligible studies utilized population-based registries and administrative datasets as data sources. The Swedish Medical Birth Register and Medical Registry of Norway were used in two separate studies. Additional sources used were the Norwegian Kidney Biopsy Registry, AOK Baden-Wurttemberg (Germany), Norwegian Renal Registry, Norwegian Cause of Death Registry, Canadian Institute for Health Information, Dutch perinatal registry (Perined), Hospitalization database of Soroka University Medical Centre (Israel), and Tehran Lipid and Glucose Study (Iran).
Demographic
Demographic characteristics, such as maternal age, ethnicity, socioeconomic status, and comorbidities, were reported in the majority of studies. Maternal age at delivery or diagnosis of CKD was reported as the mean ± (SD), median, age range, or stratification by age groups. Ethnicity information was not consistently provided, and when it was, it was reported at the cohort level across the entire population. Burger et al., 2023 10 reported a multiethnic Dutch cohort and found no strong evidence that ethnicity changed the relationship between PTB and CKD. Ethnicity data were insufficient for statistical analysis. Maternal body mass index (BMI) was reported in four studies for the entire cohort, and two studies reported the prevalence of obesity (BMI ≥ 30 kg/m2) among the population of mothers who birthed preterm as 0.8% and 4%. The majority of participants who delivered prematurely had a normal BMI. Smoking status data were available in three studies, showing 51–54% non-smokers.
Preterm delivery definition and prevalence
Preterm delivery was consistently defined across all studies as delivery before 37 weeks of gestation. The pooled prevalence of preterm delivery was 8.5% (95% CI: 6.3–10.7%), ranging from 5.5% (Sandvik et al. 2010) to 16.4% (Pariente et al. 2017).
Subcategorization by gestational age at birth varied between reports; only four studies9,16,26,28 reported the subcategories in their analysis, but the gestational age cutoff was different, which did not allow subgroup analysis. Three of the included studies (Crump 2024, Burger 2023, and Saei Ghare Naz 20219,10,27) differentiated spontaneous from iatrogenic preterm delivery.
Gestational age assessment was documented in six of the nine included reports via the last menstrual period (n = 4) or ultrasonography (n = 2). The remaining three studies did not mention this. Eight of the nine studies reported only singleton pregnancies. Parity varied between studies, with most data including parous women.
Long-term renal outcome
The prevalence of chronic kidney disease varied across studies (0.14%–1.02% in the PTB groups and 0.07%–0.48% in the term groups). The majority of studies identified CKD cases using International Classification of Disease Codes (ICD-9/ ICD-10) diagnostic codes supplemented with laboratory data of (eGFR, albumin-to-creatinine ratio) or by reviewing clinical records documenting renal replacement therapy. One study uniquely examined kidney disease requiring renal biopsy as an indicator of glomerular pathology. 16 Despite this, all studies assessed the effect of giving birth preterm on subsequent maternal renal pathologies, which allowed for comparison across the study participants.
Meta-analysis
Five studies provided raw data extractable for quantitative meta-analysis included 3,800,067 participants (Vikse et al., 2006; Crump et al. 2024, Burger et al. 2023, Pariente 2017, Sai Naz et al. 2021). As noted above, Sandvik et al. (2010) was excluded from the quantitative analysis as it reported the same Norwegian dataset as Vikse et al. (2006) with an overlapping time period.
The pooled analysis using a random-effects model demonstrated that a history of giving birth preterm was significantly associated with an increased risk of subsequent maternal kidney disease compared with giving birth at full-term (pooled OR = 1.82; 95% CI: 1.17–2.85; p = 0.01; Figure 2). Four of the five studies showed a positive association between preterm delivery and CKD, while one study by SaiNaz et al. (2021) reported a non-significant inverse association. Heterogeneity was observed across the studies (I
2
= 94.09%, τ2 = 0.23). To identify the source of heterogeneity, a “leave-one-out” sensitivity analysis was conducted by systematically excluding each study and recalculating the pooled effect estimate. The analysis identified SaeiNaz et al. 2021 as a potential source of heterogeneity. When this study was excluded, the pooled OR increased to 2.16 (95% CI 2.06- 2.26, p < 0.001, Figure 3). Exclusion demonstrated shorter and more precise CI (2.06–2.26) vs (1.17–2.85). Heterogeneity also decreased (I
2
= 0.00)
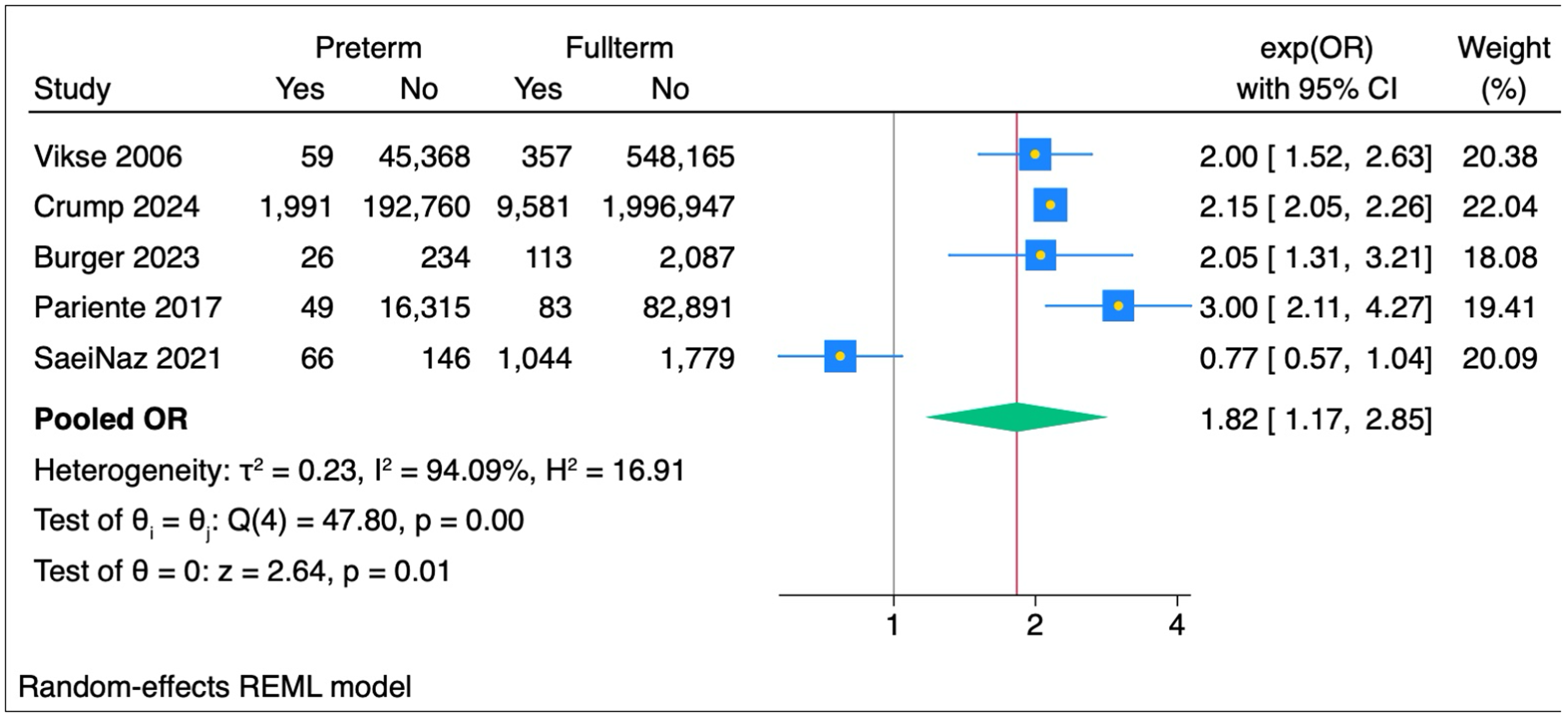
Forest plot showing the five studies included in the meta-analysis, assessing the statistical significance between preterm delivery and long-term maternal kidney disease.
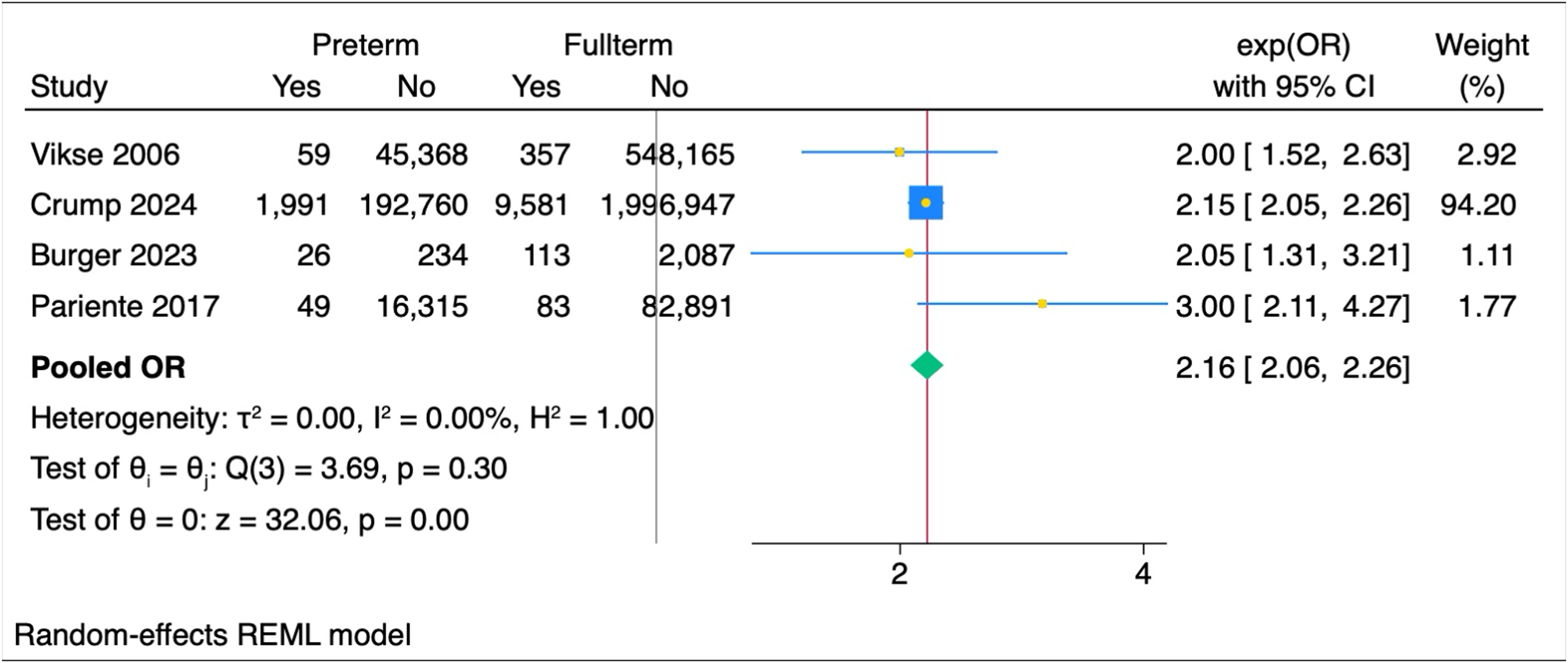
Meta-analysis of studies (after excluding Saei Ghare Naz 2021) investigating the association between preterm delivery and maternal kidney disease. Forest plots display individual and pooled estimates of the OR of Preterm and Full-term.
Studies reporting hazard ratios
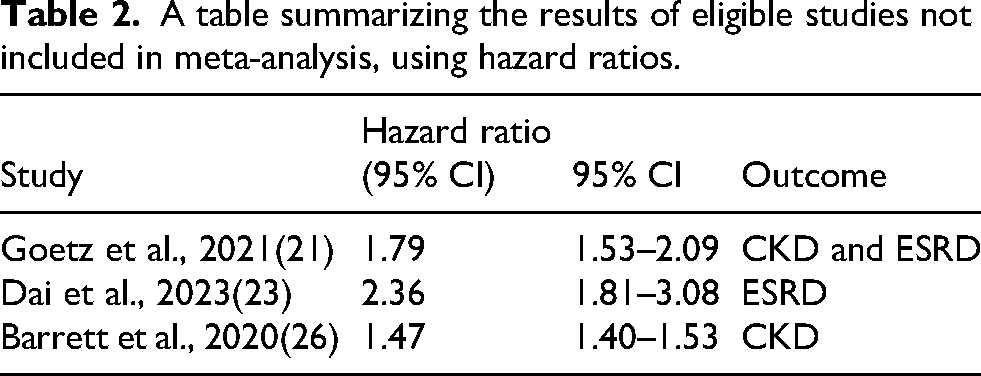
The three remaining eligible studies (Goetz et al., 2021; Dai et al., 2023; Barrett et al., 2020) were not suitable for meta-analysis, as they did not report raw data but hazard ratios. The hazard ratios in these studies compared the likelihood of poor long-term renal outcomes in mothers who delivered preterm against those who delivered full-term. All studies reported a hazard ratio greater than one, and the 95% CIs did not include one. These findings are consistent with the results of the meta-analysis presented in Table 2. Barret et al. reported adjusted HR
A table summarizing the results of eligible studies not included in meta-analysis, using hazard ratios.
Quality assessment
The included studies generally demonstrated high methodological quality, highlighting large population-based samples, longer follow-up durations, and adjustment for confounders. The Newcastle-Ottawa scale was used to assess bias. All nine eligible studies scored between seven and nine showing a low risk of bias (Figure 4). The diversity in the definition and measurement of kidney disease, as well as inconsistent reporting of age, parity, or preterm stratification, contributed to the heterogeneity in the score. Full quality assessment details are provided in Supplement 3.
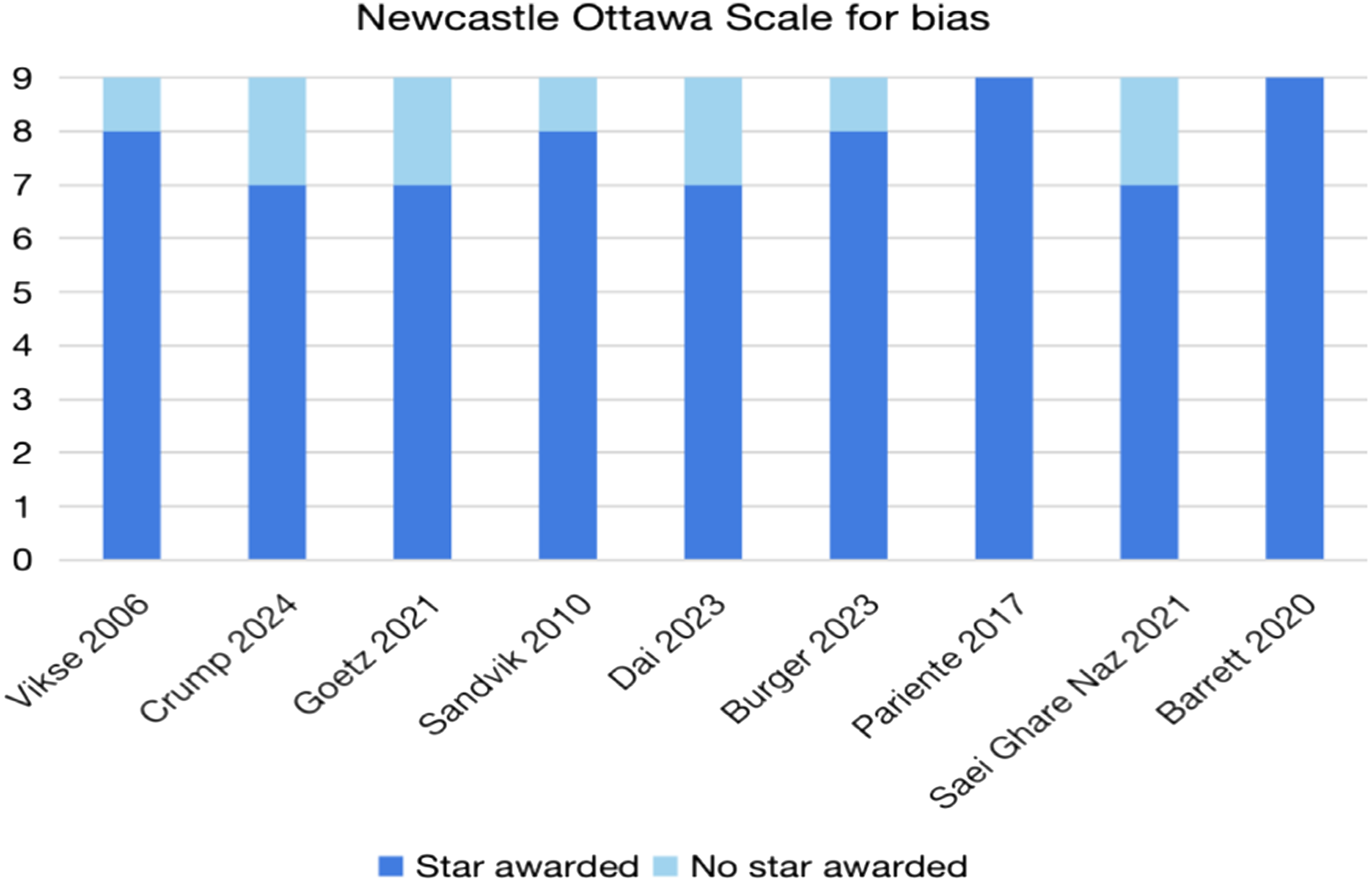
A bar chart displaying the Newcastle Ottawa scale for bias for all the included studies.
Discussion
This review challenges the traditional concept of preterm delivery as primarily a neonatal outcome. The data from nine studies involving over 8 million women from eight countries revealed that earlier delivery emerges as a condition that is associated with long-term maternal health impacts even decades after delivery. Our data shows association of developing kidney disease in women with a history of preterm delivery compared to those who delivered at term with OR 1.82 (95% CI: 1.17–2.85).This finding is remarkably consistent across geographically diverse populations, different healthcare systems, and varying study periods, with follow-up durations of up to 46 years, which provides a substantial opportunity to capture long-term kidney disease outcomes among the population of women who gave birth to preterm. The findings of studies not included in the meta-analysis23,25,28 further support the meta-analysis findings, demonstrating a higher risk of adverse long-term renal outcomes associated with preterm delivery even after adjusting for other factors such as preeclampsia or other hypertensive disorders (Figure 2).
Temporal trends in risk
The current review included studies with extended follow-up durations (over 40 years), which showed that the risk of kidney disease associated with preterm delivery persists across decades. In Crump et al. (2024), although the risk was highest in the first 10 years after delivery, the significant associations remained even 30–46 years later. To further support this, Norwegian population-based studies by Vikse et al. (2006) and Sandvik et al. (2010) demonstrated sustained risk over 20–30-year follow-up periods, with stronger associations observed in early postpartum years but persistent elevation extending throughout the observation period.
Gestational age at delivery
Some of the included studies examined dose-response relationships (gestational age at delivery and subsequent CKD). Vikse et al. (2006) found increasing kidney disease incidence with decreasing gestational age at delivery: 0.4% for deliveries <34 weeks versus 0.2% for 34–36 weeks compared to 0.1% in term deliveries. This pattern was consistent across multiple studies,26,28 suggesting that earlier delivery might be linked to a higher potential risk. Crump et al. (2024) interestingly demonstrated that women with multiple adverse pregnancy outcomes, including delivering preterm, had progressively higher CKD risk, with hazard ratios increasing from 1.52 for one adverse outcome to 3.67 for three or more adverse outcomes.
Link between preterm delivery and long-term kidney disease
The biological mechanisms underlying the association between giving birth preterm and long-term maternal kidney disease are likely multifactorial and remain incompletely understood. The marked hemodynamic demands of pregnancy, including the physiological increase in glomerular filtration rate, 8 may function as a stress test that unmasks subclinical renal susceptibility in women with pre-existing, yet not apparent, endothelial or microvascular compromise, with preterm delivery representing an early clinical signal of this underlying vulnerability rather than its cause. In addition, chronic low-grade inflammation represents a plausible common pathway: pro-inflammatory cytokines and elevated C-reactive protein, which have been implicated in the pathogenesis of spontaneous preterm delivery,14,29 are also recognized drivers of glomerular injury, interstitial fibrosis, and CKD progression. 12
Beyond these vascular mechanisms, insulin resistance and the metabolic syndrome constitute a possible shared link: both independently predispose women to giving birth preterm 7 and to developing CKD30,31 and some of our included studies reported higher prevalence of gestational diabetes among women who gave birth preterm, suggesting metabolic vulnerability as a potential shared foundation. Of note, broader environmental and social factors, including socioeconomic disadvantage, poverty, and associated health inequalities, may independently impact both the risk of giving birth preterm and the development of long-term kidney disease. In a nationwide population-based study in the Netherlands, disadvantaged neighborhood trajectories showed higher odds of adverse birth outcomes mainly preterm delivery. Multiple reports also showed that socioeconomic deprivation is independent risk associated with an increased hazard of CKD.32–34
A critical consideration when interpreting the association between preterm delivery and subsequent maternal kidney disease is whether this relationship is independent of hypertensive disorders of pregnancy, particularly preeclampsia. While our pooled raw data did not fully separate type of preterm delivery whether spontaneous or iatrogenic, the studies included within the meta-analysis reported their findings separately for preterm delivery without hypertensive disorders. Moreover, the individual studies reported the HRs included adjusted effect estimates for different pregnancy factors, including preeclampsia, and still reported significant results, providing supportive evidence for the independence of this association. Hypertensive disorders of pregnancy, particularly preeclampsia, share several pathophysiological mechanisms with both preterm delivery and long-term renal disease, and their co-occurrence warrants specific consideration9,23 . Preeclampsia is characterized by systemic endothelial dysfunction, placental insufficiency, glomerular endotheliosis, and dysregulation of angiogenic factors, 35 all of which cause direct renal injury during pregnancy and may result in persistent microvascular damage that predisposes to CKD years later. 36 These same pathways—endothelial activation, RAAS dysregulation, and pro-inflammatory signaling—are implicated in the pathogenesis of spontaneous preterm delivery, creating a biologically plausible overlap between these conditions. 37
Whilst this biological overlap is acknowledged, the evidence synthesized in this review supports that the association between giving birth preterm and long-term maternal kidney disease is not entirely dependent on this shared pathway. Across multiple included studies, the association remained significant after adjustment for preeclampsia in women who gave birth spontaneously preterm without any hypertensive disorder. The largest study included in this review by Crump et al., 9 which examined over 2.2 million women, demonstrated an association between maternal CKD and preterm delivery which remained significant after adjusting for preeclampsia and other pregnancy complications. Similarly, Vikse et al. (2008) found a persistent association between earlier delivery and the development of biopsy-confirmed kidney disease after excluding those who developed pre-eclampsia. Likewise, the results were reported by Barret et al. (2020) from their Swedish national cohort study showed that preterm delivery was significantly associated with end-stage kidney disease, even when preeclampsia was excluded from the analysis. Although the RR was higher when associated with preeclampsia, participants who had spontaneous preterm delivery (before 37 weeks) without preeclampsia maintained an adjusted significant relative risk of 2.09 (95% CI: 1.64–2.66) for end-stage kidney disease. Collectively, this evidence supports the interpretation that preterm delivery itself may play an independent role in the development of long-term renal disease.
Another argument which could support the independent association of preterm delivery and CKD is the data by Burger et al. (2023) 10 which examined a multi-ethnic Dutch cohort and demonstrated no significant impact of ethnicity on the risk of long-term kidney disease among the population of women who delivered preterm. This suggests that the association is not due to ethnic predisposition and can be explained by exposure to the risk of birthing prematurely. Interestingly, the study noted that the rates of preterm delivery and absolute numbers of both preterm delivery and kidney disease differed between ethnic groups, and higher rates were observed in South Asian Surinamese, African Surinamese, and Ghanaian populations, which might reflect the existing disparities.
Four of the five included studies showed a significant positive association between preterm delivery and maternal CKD, except for one. Further assessment of the outlier study by SaeiNaz et al. 27 showed it to have a smaller sample size of 3035 participants and assessed a predominantly Asian cohort in comparison to the other studies, which assessed predominantly western cohorts. This might explain the difference in ORs due to other health impacts within the population with a higher causative risk. Despite this, the study reported a significant association between preterm delivery and CKD when adjusted for age at delivery (term or preterm) and other predictive risks, including BMI and smoking status.
Comparison with previous research
Previous systematic reviews comparing adverse pregnancy outcomes and long-term maternal renal disease have identified delivering preterm as an independent risk factor for CKD. The most recent Wu et al., 17 demonstrated a significant risk of renal disease with HR: 1.98 (95% CI: 1.57, 2.50). They found a similar significant HR for ESRD cases. A major difference between our data and Wu et al. is that our data included the most recent population-based study by Burger et al. 10 and Crump et al., 9 which examined data for more than 2.2 million women. This review also uniquely used raw data, which allowed for more accurate comparisons between studies, as it was not impacted by differences in the adjustments undertaken within individual studies.
Strengths and limitations
This review has several strengths. A major strength of this meta-analysis is its large sample size of >8 million participants. This enhances the generalizability of the results and reliability of the findings, as almost all studies showed a positive association between preterm delivery and long-term kidney sequelae. Second, we used raw event counts from the included studies to calculate effect estimates (pooled OR). This approach allowed for the direct analysis of the risk of CKD in women who delivered early versus those who delivered at term. In addition, this methodological approach helped minimize the dependence on variably adjusted estimates drawn from individual studies. Importantly, adding more raw data from two large population-based studies and not relying on HR as an effect estimate, as previous studies did, allowed conveying absolute risk estimates across the dataset. Thirdly, almost all studies included in the meta-analysis showed a significant link between delivering preterm and adverse maternal renal outcomes. Even in studies where raw data could not be extracted, the effect estimates (HR) in those studies demonstrated the same positive significant association.
This review also highlights a critical gap in women's health care. Currently, people with reproductive potential, transition from close perinatal care to ad-hoc gynecological or primary care follow-up, with little focus on pregnancy complications as predictors of future health outcomes. This represents a missed opportunity for early intervention and prevention. Our data suggest that the 8–15% of women who deliver preterm could be targeted for long-term health interventions. Despite this, current clinical practice largely ignores data such as these, which provide a valuable prognostic indicator that may guide long-term follow-up. Notably, heterogeneity was initially encountered in the meta-analysis, indicating variability between the studies. To further investigate this, a sensitivity analysis was conducted to identify the source of variability.
One limitation of our review is that raw data could not be extracted from all the included studies to add to the meta-analysis after contacting the authors. However, a meta-analysis was conducted from event counts of the majority of the studies (five out of nine) and complemented the review with a narrative synthesis of the remaining studies. A further limitation of this review is the inability to fully disentangle the independent contribution of preterm delivery from that of co-occurring hypertensive disorders of pregnancy in all included studies, as not all studies stratified preterm deliveries by whether spontaneous or iatrogenic or completely separate raw numbers with hypertensive disorders despite adjusting for confounding in estimating the risk. Whilst the dose-response relationship between earlier gestational age and increasing renal risk observed across multiple studies provides evidence of a biological signal independent of hypertensive status, residual confounding by hypertensive disorders cannot be entirely excluded from the pooled unadjusted analysis.
Future work
Future studies should aim for more standardized reporting of populations and definitions of renal disease, with clear and consistent methodologies to enable reliable comparisons. In addition, the biological link, so far in the literature, between preterm delivery and renal disease is less understood. Further mechanistic and translational research is needed to clarify the biological pathways linking mothers who deliver preterm and long-term maternal kidney disease.
Conclusion
This meta-analysis and narrative synthesis showed an association between preterm delivery and the long-term risk of maternal renal disease. The findings suggest that preterm delivery could be an early indicator of susceptibility to this disease, allowing for an increase in screening for mothers affected by preterm delivery. This would ultimately enable better prediction and medical management of these patients instead of waiting for CKD to evolve before acting on it.
Supplemental Material
sj-docx-1-obm-10.1177_1753495X261445504 - Supplemental material for Preterm delivery and long-term maternal renal disease: A systematic review and meta-analysis
Supplemental material, sj-docx-1-obm-10.1177_1753495X261445504 for Preterm delivery and long-term maternal renal disease: A systematic review and meta-analysis by Emily Stocks, Maryam Abdelkarim, Megan Holness, Siobhan Quenby and Joshua Odendaal in Obstetric Medicine
Supplemental Material
sj-docx-2-obm-10.1177_1753495X261445504 - Supplemental material for Preterm delivery and long-term maternal renal disease: A systematic review and meta-analysis
Supplemental material, sj-docx-2-obm-10.1177_1753495X261445504 for Preterm delivery and long-term maternal renal disease: A systematic review and meta-analysis by Emily Stocks, Maryam Abdelkarim, Megan Holness, Siobhan Quenby and Joshua Odendaal in Obstetric Medicine
Supplemental Material
sj-docx-3-obm-10.1177_1753495X261445504 - Supplemental material for Preterm delivery and long-term maternal renal disease: A systematic review and meta-analysis
Supplemental material, sj-docx-3-obm-10.1177_1753495X261445504 for Preterm delivery and long-term maternal renal disease: A systematic review and meta-analysis by Emily Stocks, Maryam Abdelkarim, Megan Holness, Siobhan Quenby and Joshua Odendaal in Obstetric Medicine
Footnotes
Acknowledgements
The authors have no acknowledgements to declare.
Ethical approval
This study did not require ethical approval as it involved analysis of previously published data.
Authorship
ES, MH: conducted systematic search, performed screening and data extraction, conducted statistical analysis, Writing - Original Draft, approved final version. MA: Performed data extraction and quality assessment, methodology, statistical analysis, Writing – Review & Editing, approved final version. JO: Conceived the study, developed methodology, critically reviewed and edited the manuscript, approved final version. SQ: Conceived the study, critically reviewed and edited the manuscript, provided supervision throughout, approved final version. All authors meet ICMJE criteria for authorship and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Maryam ABDELKARIM, Obstetrics and Gynaecology NIHR Academic Clinical Fellow
Patient consent
No patient consent was not required for this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.