
Abstract
Background:
There have been significant advances in the treatment of patients with cardiomyopathy with reduced ejection fraction (EF < 40%). However, there is a dearth of information in the treatment of patients with cardiomyopathy and midrange EF (40–50%). Current guidelines state to treat these patients similarly to patients with cardiomyopathy and preserved EF. Data from the Prevention of Events with Angiotensin-Converting Enzyme Inhibition (PEACE) trial were used to elucidate whether angiotensin-converting enzyme (ACE) inhibitors improve clinical outcomes in patients with ischemic cardiomyopathy and midrange EF.
Methods:
A post hoc subgroup analysis of the PEACE trial was conducted to evaluate the effect of ACE inhibitors in a subgroup of patients with ischemic cardiomyopathy and midrange EF (40–50%). A Chi-square test and a Student‘s t-test were used to examine and compare the binary and continuous variables of baseline characteristics and outcomes between experimental and comparison groups.
Results:
We studied a subgroup of patients from the PEACE trial with ischemic cardiomyopathy and midrange EF (n = 2512 of 8290 total patients). Patients were assigned to either the interventional group (n = 1247) or the placebo group (n = 1265). There were no significant differences in baseline demographic and health characteristics between the two groups. During a total of 7 years (mean 4.7 years) of follow up, the risk of composite outcomes [all-cause mortality, nonfatal myocardial infarction, and stroke; relative risk (RR) 0.79, 95% confidence interval (CI) 0.63–0.98; p = 0.03] and all-cause mortality (RR 0.85, 95% CI 0.73–0.99; p = 0.03) was reduced in patients treated with trandolapril.
Conclusion:
This study revealed the benefit of ACE inhibitors among patients with ischemic cardiomyopathy and midrange EF.
Introduction
Heart failure confers significant morbidity ranging from fatigue to dyspnea at rest, leading to a poor quality of life. The death rate attributable to heart failure was 84 per 100,000 in 2014, and the 5-year case fatality rate was found to be at 42.3% after a hospitalization for heart failure. 1 Patients with heart failure are classified based on their ejection fraction (EF) as having either reduced EF (HFrEF), midrange EF (HFmrEF), or preserved EF (HFpEF). 2 There have been significant advances in the treatment of patients with HFrEF (EF < 40%), ranging from hydralazine plus isosorbide dinitrate to the combination of an angiotensin receptor blocker (ARB) and a neprilysin inhibitor which was approved by the United States Food and Drug Administration (US FDA) in 2015. 3 Unfortunately, there is a dearth of available therapies that have been shown to improve outcomes in the treatment of patients with heart failure and EF > 40%. 4
In the CHARM-Preserved and I-PRESERVE trials which looked at two different ARBs in the treatment of patients with heart failure and EF > 40%, both candesartan and irbesartan did not have any effect on cardiovascular outcomes.5,6 Other trials which looked at different therapies including digoxin in patients with heart failure and an EF > 45% also did not show any benefit. 7 More recently, the TOPCAT trial published in 2014 showed that spironolactone did not have any effect on cardiovascular death in patients with heart failure and an EF > 45%. 8 However, a subgroup analysis of this study showed that spironolactone might be of benefit in patients with heart failure and midrange EF. 9
There are currently differing opinions on how to treat a subset of HFpEF patients with HFmrEF, which is defined as having an EF between 40 and 50%. 10 While current guidelines state to treat these patients similarly to patients with HFpEF, more recent analyses show that it may be more appropriate to treat these patients similarly to patients with HFrEF.9,10 Bhambhani and colleagues revealed that the mortality risk associated with HFmrEF was worse than HFpEF, and almost similar to HFrEF. 11 In addition, a recent analysis of two prospective, longitudinal, multicenter cohorts of ambulatory patients with chronic heart failure, MUerte Subita en Insuficiencia Cardiaca and Red Española de Insuficiencia Cardiaca (REDINSCOR), showed that patients with HFmrEF have an intermediate phenotype between HFrEF and HFpEF. 12
The Prevention of Events with Angiotensin-Converting Enzyme Inhibition (PEACE) trial was a large double-blind, placebo-controlled study which showed that patients with preserved EF and stable coronary artery disease who were receiving current standard therapy did not derive additional benefit from taking an angiotensin-converting enzyme (ACE) inhibitor. 13 From these trial data, we sought to determine whether ACE inhibitors conferred any benefit in the subset of patients with midrange EF.
Methods
Study population
Data from PEACE trial were used to conduct a post hoc subgroup analysis. The PEACE trial was a phase III therapeutic, multicenter, placebo-controlled, double-blind, randomized clinical trial of trandolapril. The PEACE trial included patients aged 50 years and older with coronary artery disease and left ventricular EF > 40%. 13
Patients with a left ventricular EF between 40 and 50% were extracted from this trial to evaluate the therapeutic effect of adding an ACE inhibitor, trandolapril, to patients with stable coronary artery disease and midrange EF (40–50%). Our analysis included a total of 2512 patients (30% of the 8290 enrolled in the trial). A total of 1247 patients received trandolapril, and 1265 received placebo.
Definitions and measurement of key variables
Intention-to-treat analysis was used to compare the primary and secondary outcomes of the two groups (trandolapril and placebo). A Chi-square test was used to test for differences between the two treatment groups. A Kaplan–Meier curve was also used to illustrate the differences in cardiac outcomes between the two groups. The statistical analyses were performed using SAS version 9.4. All tests were conducted using an α = 0.05 as the probability for a type I error.
Results
In total there were 2512 patients in the analysis, with 1247 assigned to the trandolapril group and 1265 assigned to the placebo group. Table 1 displays their descriptive baseline demographic and health characteristics. There were no statistically significant differences between the baseline characteristics of the two groups in Table 1 except for rate of diabetes (19.18% versus 15.89%).
Baseline characteristics of the patients.*

Values are means ± SD.
p < 0.05 for the comparison with placebo.
CABG, coronary artery bypass grafting; CCS, Canadian Cardiovascular Society; DBP, diastolic blood pressure; DM, diabetes mellitus; GFR, glomerular filtration rate; HTN, hypertension; PCI, percutaneous coronary intervention; SBP, systolic blood pressure; SD, standard deviation
Outcome
Table 2 presents the comparisons in the incidence of cardiovascular disease and death between the two treatment groups. During a total of 7 years (mean 4.7 years) of follow up, the risk of the composite outcome (all-cause mortality, nonfatal MI and stroke) was lower in trandolapril-treated patients [relative risk (RR) 0.79, 95% confidence interval (CI) 0.63–0.98; p = 0.03]. All-cause mortality was also lower in trandolapril-treated patients (RR 0.85, 95% CI 0.73–0.99; p = 0.03). However, there was no statistical difference between trandolapril and placebo-treated patients with regard to cardiovascular mortality, noncardiovascular mortality, MI or stroke.
Incidence of cardiovascular disease and death.

CI, confidence interval; MI, myocardial infarction.
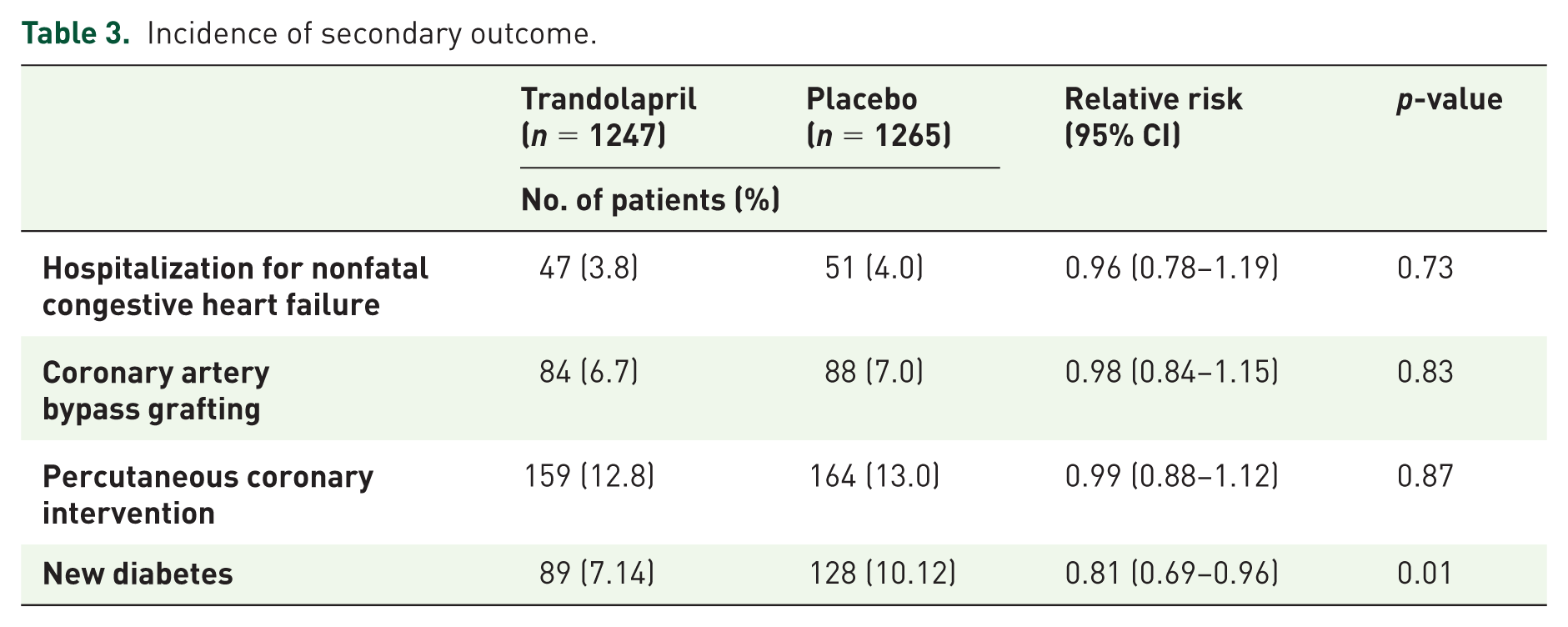
Table 3 displays the comparisons in the incidence of the secondary outcomes between the two treatment groups. None of the comparisons were statistically significant except for the incidence of diabetes. The risk of new diabetes was lower among patients who received trandolapril. Figure 1 shows the Kaplan–Meier survival curve for the incidence rate of the composite outcome (all-cause mortality, nonfatal MI and stroke) in the two treatment groups for 7 years (mean 4.7 years) of follow up. Patients who received trandolapril had a significantly lower rate of the composite outcome than patients who received placebo (p = 0.042). Lines started to separate after approximately 1.5 years from randomization. Figure 2 shows the Kaplan–Meier survival curve for the incidence rate of all-cause mortality in the two treatment groups. Patients who received trandolapril had significantly longer survival than patients who received placebo (p = 0.047).
Incidence of secondary outcome.

Cumulative incidence of the composite outcome (all-cause mortality, nonfatal MI and stroke) according to treatment group.

Cumulative incidence of all-cause mortality (cardiovascular mortality and noncardiovascular mortality), according to treatment group.
Discussion
To our knowledge, this study is the first to examine the effect of ACE inhibitors on patients with ischemic cardiomyopathy and an EF of 40–50%. The current investigation demonstrates that ACE inhibitors reduced the risk of the composite outcome of all-cause mortality, nonfatal MI and stroke by 21% among patients with ischemic cardiomyopathy and an EF range between 40 and 50%. This study also showed that all-cause mortality was reduced by 15% among patients who were randomized to trandolapril compared with individuals who were randomized to placebo. The number needed to treat to prevent one of the combined outcomes and death were 31 and 40 patients, respectively.
The benefits of ACE inhibitors in patients with HFmrEF is driven by the fact that coronary artery disease is more common in patients with HFmrEF than patients with HFpEF, which was proven in two separate registries (the Swedish Heart Failure Registry and The European Society of Cardiology Heart Failure Long-Term Registry).14,15 ACE inhibitors have been shown to enhance cardiovascular outcomes in patients with coronary artery disease in two major clinical trials.16,17 ACE inhibitors improve cardiovascular outcomes by decreasing the production of angiotensin II and tumor necrosis factor alpha and by increasing the production of bradykinin and nitrate. The change in the level of these proteins leads to enhanced endothelial function. 18 This change also reduces endothelial apoptosis by minimizing oxidative stress, which is harmful to endothelial cells.18,19
In our study, there was no statistically significant difference between the two groups in regard to cardiovascular mortality, noncardiovascular mortality, nonfatal MI, or stroke when these outcomes were examined separately. These findings are likely because there was not enough power (sample size) to demonstrate significant differences between the two groups in regard to these outcomes. Interestingly, this study showed that patients who were randomized to trandolapril had a 19% lower risk of new diabetes compared with individuals who were randomized to placebo. The reduction in the risk of diabetes was demonstrated in the original study. 13
The effect of ACE inhibitors on the incidence of diabetes mellitus type II is a well-known phenomenon. Several clinical trials have shown that ACE inhibitors, as well as ARBs, reduce the risk of diabetes mellitus type II by 14–34% compared with placebo and other antihypertensive drugs.16,20–24 ACE inhibitors and ARBs reduce the risk of diabetes by increasing insulin secretion from the pancreas and by enhancing insulin sensitivity in the adipocytes and muscle fibers. The underlying mechanism of this protective effect is still not fully understood, but it is thought to be driven by the increase in the level of bradykinin.25–27
Previous clinical studies have shown that ACE inhibitors reduce mortality and hospitalization among patients with reduced left ventricular (LV) EF < 40%. 28 ACE inhibitors have also been shown to reduce the rates of cardiovascular events and mortality in patients with coronary artery disease and a history of diabetes or hypertension.16,29 Therefore, the American College of Cardiology guidelines state that ACE inhibitors should be prescribed to all patients with stable coronary artery disease with a history of hypertension, diabetes mellitus, a LV EF < 40%, or chronic kidney disease (class I). 30 However, ACE inhibitors have not previously been shown to be beneficial in patients who have an LV EF > 40% with low cardiovascular risk factors.13,31
Our study revealed that ACE inhibitors may reduce the risk of combined cardiovascular disease and death in patients with ischemic cardiomyopathy and midrange EF (40–50%). This is the first study to examine the effect of ACE inhibitors in patients with coronary artery disease and midrange EF. ACE inhibitors reduced the combined outcome by 21% and reduced death by 15%. The major limitation of this study is that it was a subset analysis that was not prespecified. In light of this, the results should be seen as hypothesis-generating only. Moreover, the patients were predominantly male (85%), which makes it difficult to generalize the results to female patients. Finally, the results of this study may not represent current data because the original study was conducted more than two decades ago. However, there is still no significant change in the guidelines in treating patients with midrange EF or patients with coronary artery disease.
Conclusion
This study unveiled the benefit of an ACE inhibitor, trandolapril, in reducing the risk of cardiovascular disease events and death among patients with ischemic cardiomyopathy and midrange EF.
Footnotes
Acknowledgements
This research would not have been possible without the support of the National Heart, Lung, and Blood Institute (NHLBI) Biologic Specimen and Data Repository Information Coordinating Center. This manuscript was prepared using PEACE research materials obtained from the NHLBI Biologic Specimen and Data Repository Information Coordinating Center and does not necessarily reflect the opinions or views of the PEACE study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.