
Abstract
Objective
The results of the Women’s Health Initiative studies dramatically altered hormone therapy use around the world. In countries outside the United States, self-use in physicians remained unaltered while prescription use declined, implying that physicians may not concur with the findings. We wished to explore prevailing attitudes among American physicians by examining New York City obstetrician-gynaecologists’ self-use and prescription use of hormone therapy.
Study design
All board-certified obstetrician-gynaecologists in New York City were invited to complete and return a detailed, previously validated questionnaire concerning hormone therapy use.
Results
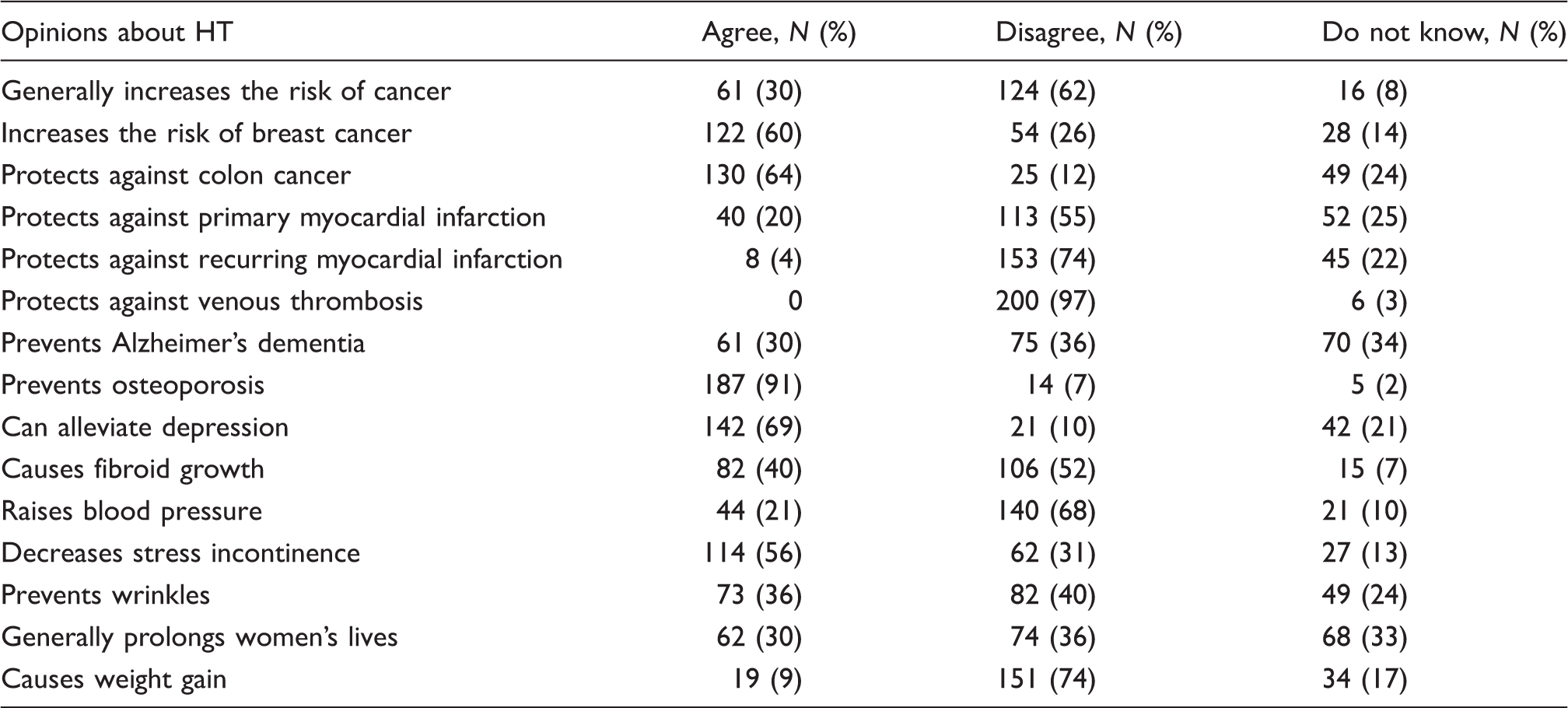
Two hundred and nine questionnaires were returned, for a response rate of 12% (209/1797). Gynaecologists agreed with the findings from the Women’s Health Initiative studies regarding indications and contraindications to hormone therapy use. Even so, three-quarters of female gynaecologists and female partners of male gynaecologists (74%; 67/91) use or have previously used hormone therapy. However, only 27.3% (21/77) of male gynaecologists and 12.3% (14/114) of female gynaecologists recommend hormone therapy to all menopausal women regardless of contraindications. Gynaecologists remain divided in their attitude toward hormone therapy; 30% of gynaecologists felt that hormone therapy use generally prolonged women’s lives, 36% felt it was not useful in prolonging women’s lives, and 33% were unsure.
Conclusion
Since the publication of the Women’s Health Initiative findings, New York City gynaecologists prescribe hormone therapy to fewer patients. However, they continue to self-use hormone therapy at much higher rates, even as they seem to concur with Women’s Health Initiative recommendations, contributing to the ongoing controversy surrounding the validity of the Women’s Health Initiative findings.
Introduction
Decades of observational data have suggested that hormone therapy (HT) is helpful in preventing heart disease, osteoporosis, and dementia in postmenopausal women.1–4 However, recent randomized controlled studies have yielded conflicting results on the benefits of HT use5–8 and so the preventative efficacy of HT continues to be debated.
In particular, the large Women’s Health Initiative (WHI) study of 2002 failed to demonstrate benefits for women randomized to conjugated equine estrogen and medroxyprogesterone acetate9,10 and led to a dramatic, world-wide decline in the number of hormone therapy (HT) prescriptions.9,10 The study was prematurely halted due to adverse effects in the treatment arm reaching the pre-determined set-point.11,12 On average, the women in this study were nearly a decade older than the typical woman beginning HT. Since HT use may alter disease course prior to onset rather than in those with established disease, use of HT in older women may not be as efficacious as use in young women. It is unclear if the adverse events reported by the WHI study would be applicable to the average HT user, a generally younger, healthier woman.4,13 In addition, a recent analysis of the data from the WHI study has found reduced risk for breast cancer in the estrogen-alone arm of the study. 14
Due to these controversies, physicians continue to debate the conclusions drawn from the WHI study. Several studies conducted in other countries have shown that while HT prescription rates have decreased since the publication of the WHI study in conformance with this study’s recommendation, self-use of HT in obstetrician-gynaecologists has remained essentially unchanged.15–17 Post-WHI, the rates of HT prescriptions in the United States dropped by 66% for conjugated estrogen and progestin combinations, by 33% for estrogen alone and by 50% for total HT prescriptions. 9 However, self-use of HT among American physicians as well as prevailing attitudes to the WHI recommendations are not known.
We therefore wished to explore changes in personal use of and attitudes toward HT among board-certified obstetrician-gynaecologists in the United States. We chose New York City (NYC) and the surrounding metropolitan area as our sample population and surveyed physicians in this region.
Methods
A previously validated approved questionnaire concerning attitudes, management strategies and use of HT depending on indications and contradictions was mailed out to eligible physicians in NYC. 17 The study protocol was approved by the Lenox Hill Hospital Institutional Review Board in New York, NY. All 1797 board-certified obstetrician-gynaecologists in NYC and the surrounding metropolitan area, including Long Island and Westchester County, were invited to complete and return the questionnaire. This list was obtained from the American College of Obstetricians and Gynaecologists (ACOG). Female gynaecologists were asked about their current use of HT, while male gynaecologists were asked about their spouses’ use of HT. The statistical software package SPSS 11.0 (SPSS Inc., Chicago, IL) was used for all data analyses. Frequencies were tallied and relationships between demographic variables were determined using the chi-square test.
Results
Response rates
We received 209 questionnaires, yielding a response rate of 12% (209/1797). About 60% of gynaecologists surveyed were women (124/209). The average age was 51 years (SD ± 11 years; range 30–83 years), with 25% (49/194) under age 41, 49% (95/194) under age 50, and 74% (143/194) under age 59. Of gynaecologists, 68% (139/204) were in private practice, 28% (58/204) were hospital employees, and 3% (7/204) were retired.
Counseling on HT
The age and opinion of New York City (NYC) gynaecologists concerning the question ‘Which women should be offered postmenopausal hormone therapy?’.
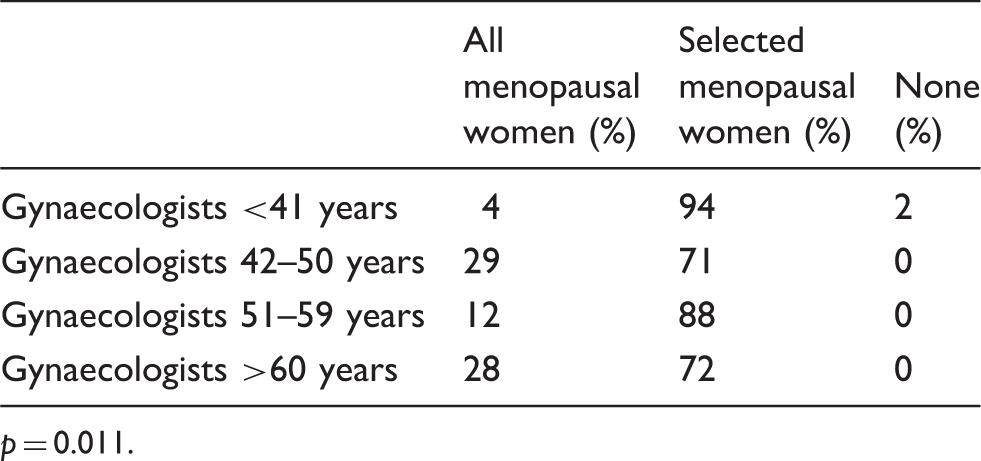
p = 0.011.
The gender and opinion of New York City (NYC) gynaecologists concerning the question ‘Which women should be offered postmenopausal hormone therapy?’.
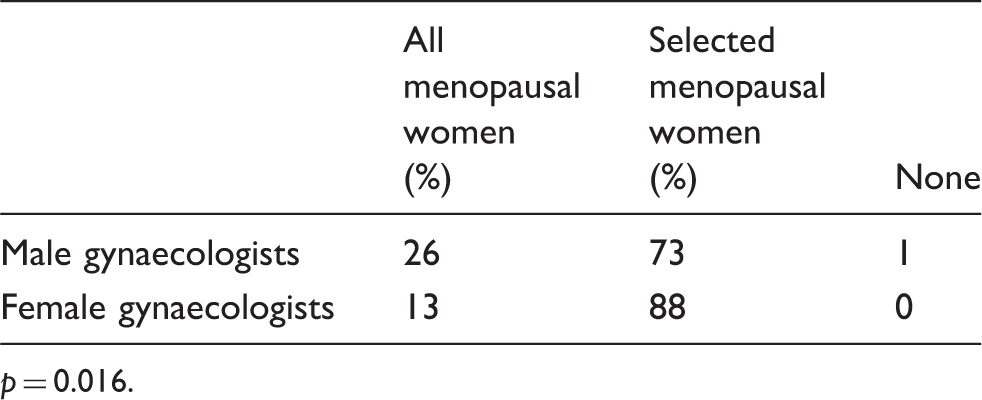
p = 0.016.
Indications and contraindications
New York gynaecologists’ self-report of prescription practices for indications and contraindications of hormone therapy (HT). a
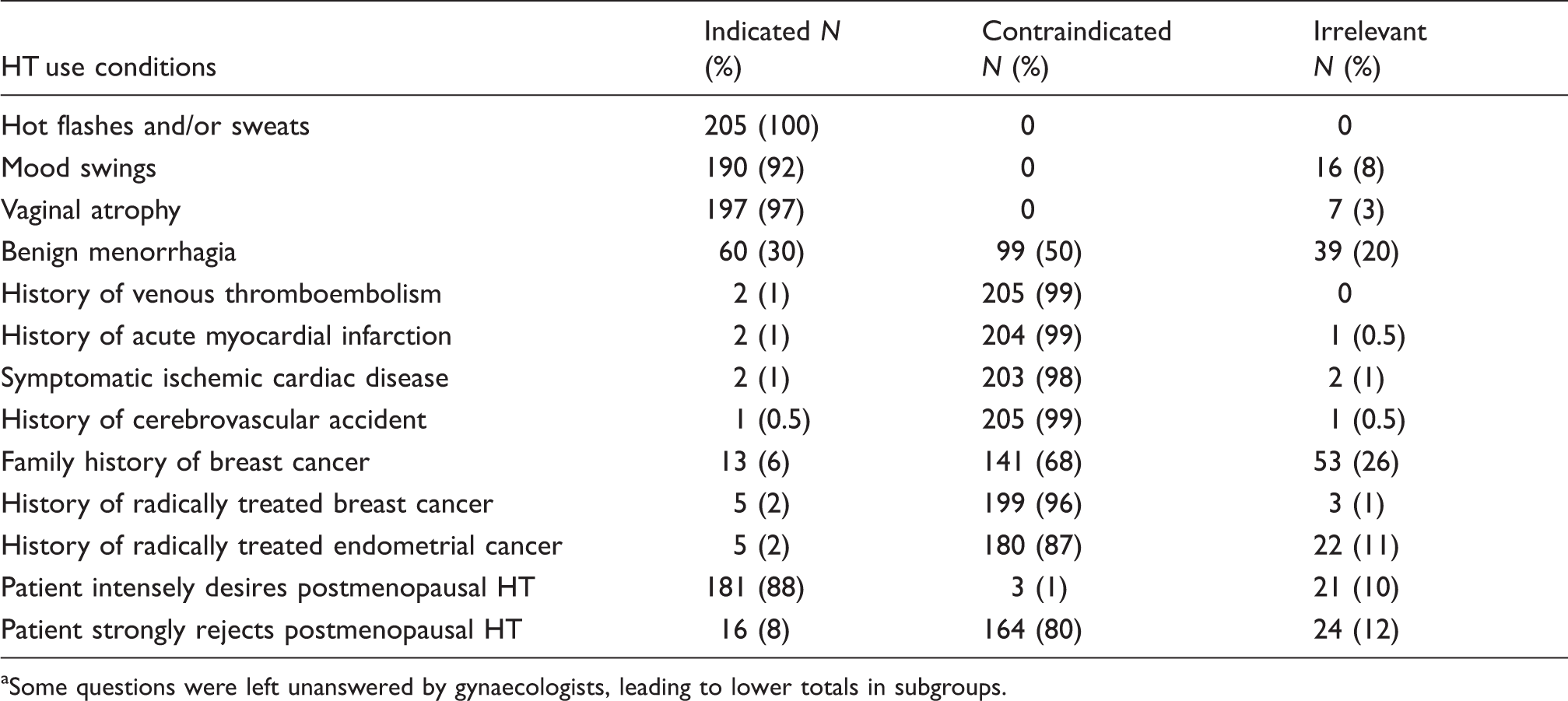
Some questions were left unanswered by gynaecologists, leading to lower totals in subgroups.
Personal use of HT
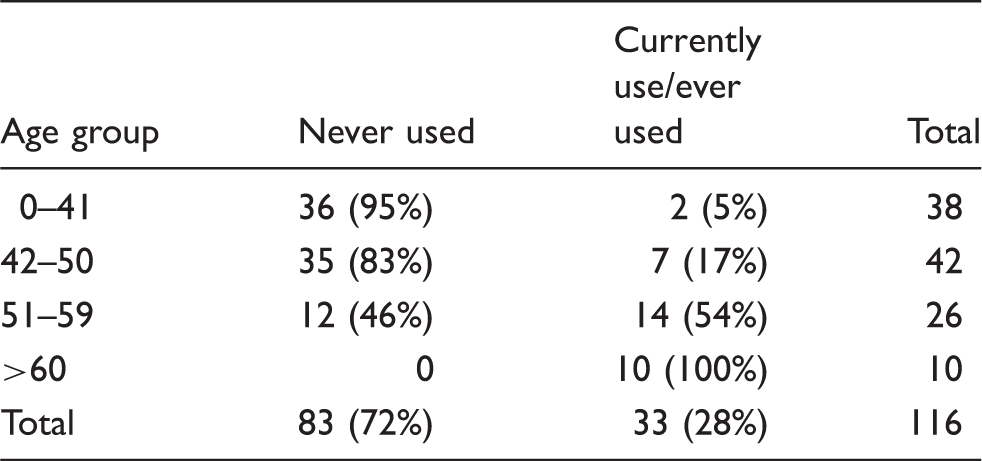
Current use of hormone therapy among New York City (NYC) female gynaecologists.
Opinions expressed about HT treatment
The opinion of New York City (gynaecologists concerning the expressed opinions about hormone therapy at menopause.
Discussion
The findings of this study highlight the discrepancy between American physician opinions on prescribing and personal use of HT. Nearly three-quarters (74%) of eligible gynaecologists and their female partners use or have used HT, while only 18% prescribe HT to eligible patients.
Our findings complement a global trend in gynaecologists prescribing and self-use of HT across the globe. In a large Scandinavian study of 1591 gynaecologists, there was no change in personal use of HT (74%) post-WHI, although only 13% offered HT to all eligible patients, 17 results nearly identical to ours. Similarly, 74% of Israeli gynaecologists had a positive opinion about HT, with 70% of the menopausal group either using it or have used it and 93% of those who were perimenopausal planning to use it. 18 In Italy, 64% of female doctors and 58% of male doctors’ wives were current users of HT, far higher rates than in the general postmenopausal population. A mere 8% of Italian women doctors and 4% of doctors’ wives discontinued HT use after the publication of the WHI data. 15 Interestingly, Italian female gynaecologists and their wives were far more likely than physicians of other specialties to use HT. 15 In Brazil, nearly a quarter (23%) of gynaecologists discontinued prescribing HT to patients, and of those gynaecologists who are still prescribing HT, 64% have reduced the doses. 19
Among those American gynaecologists who do recommend and prescribe HT for climacteric complaints, the majority recommended duration of less than 5 years. Studies conducted in various countries have indicated a trend among gynaecologists in which lower doses of HT and shorter durations of HT use are being prescribed in response to the WHI study.20,21 Interestingly, the WHI study was designed so that when the number of new cases of certain pre-specified diseases in the treatment arm reached a designated endpoint, the study would be stopped. When the study was prematurely halted 5 years into inception, there was no statistically significant difference in disease occurrence between the treatment and placebo arm.2,4,22 However, many women experience climacteric symptoms for durations greater than 5 years and it may be necessary to critically evaluate the risks and benefits of each patient’s case. 19
Our data suggest that American gynaecologists currently agree with the recommendations of the WHI. Most agreed with the earlier published analysis of WHI data that HT increases the risk of breast cancer and that myocardial infarction, cerebrovascular accidents, angina, history of breast cancer, and radically treated breast cancer were contraindications for HT (Tables 3 and 5).23,24 Scandinavian gynaecologists are also of this mindset with only 7% in 2002–2003 believing ischemic heart disease to be an indication for HT. 17 However, in 1995–1997, 56% of Scandinavian gynaecologists considered ischemic heart disease to be an indication, connoting more caution in their recommendations of postmenopausal HT following publication of the WHI guidelines.
The higher rate of HT use among American gynaecologists as compared to their prescribing practice may be explained in several ways. Perhaps the foremost explanation is conflicted information surrounding scientific conclusions about the harms and benefits of HT. The WHI study contains its own limitations including lack of statistical significance, older age and conjugated HT use, while several other independent studies show robust biological benefits from HT use, particularly when introduced earlier in the menopausal transition. 25 A further factor influencing HT prescription use may be fear of litigation, a relatively recent, but influential factor to surface in the field of medicine. For example, Schumacher et al. 26 conducted a survey revealing that younger, female physicians were much more fearful of litigation than their older, male counterparts, and this fear may lead to avoidance of therapies with conflicting data on safety and efficacy, such as HT. Finally, gynaecologists may face a patient population with concerns about HT use from public media and perception. Buhling et al. 27 found that nearly half of German gynaecological patients were badly informed by media about HT. These concerns may either not be addressed or patients may choose to refuse treatment.
There are several limitations to our study. Although there was a 12% response rate to the survey, we did not have the demographic data on those gynaecologists who did not respond. Those responding may have had inherently different practices from those who did not, although we have no reason to believe this to be the case. In fact, several studies have shown that a lower response rate does not necessarily compromise the validity of the findings.28,29 A survey with low response rates – as low as 5% – is accurate given no significant differences among respondents and non-respondents. 30 Because study participants were limited to the NYC area, the results may not necessarily reflect the views of the larger cross-section of American gynaecologists. Additionally, the study may not necessarily be an accurate reflection of the true clinical practices of gynaecologists but rather their perceptions of their practices.
Conclusion
The results of the WHI study caused world-wide ramifications, altering clinical practice but concomitantly fueling debate about the soundness of the conclusions. This is reflected in the continued high rates of self-use of HT by NYC gynaecologists even as their prescription use of HT has plummeted. Even the recommendations regarding when and how to use HT have largely been adopted by the gynaecologists surveyed, as the WHI study remains the largest study to date on this issue. It will be interesting to observe continued changes in prescription practices of HT as further analysis of the data from WHI emerges, including the recent statement that estrogen alone reduces risk of breast cancer.
Footnotes
Ethics Approval
The study protocol was approved by the Lenox Hill Hospital Institutional Review Board in New York, NY.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of Interests
None