
Abstract
Premature ovarian insufficiency (POI) can have significant health implications for the affected patient population, but remains a largely under researched area. There is lack of evidence from randomised controlled trials to guide clinical practice, regarding the optimal hormone replacement therapy regimens, dose and route of administration. Furthermore, little research has addressed the effect of the various progestogens used on health parameters in women with POI. Here we describe an ongoing randomised clinical trial looking at the effects of micronized progesterone and medroxyprogesterone acetate, both used in combination with transdermal oestradiol on the cardiovascular system, lipid profile and coagulation cascade in women with POI as a step towards better understanding of the implications of hormone treatment in this cohort of women.
Background
Premature ovarian insufficiency (POI) describes a condition characterised by primary or secondary amenorrhoea, hypoestrogenism and elevated gonadotrophin levels. The British Menopause Society Consensus Statement in 2007 acknowledged that large variations existed in the age limits used to define premature menopause but recommended that an age cut-off of 45 years should be used to define premature menopause. 1 It is estimated to affect 5% of women under 45 years of age, 5 1% of women under 40, 0.1% of women under 30 and 0.01% of women under 20.1–5
The syndrome can have both devastating short- and long-term effects on the affected patient population secondary to the deficiency of sex steroids, namely climacteric symptoms,5–7 subfertility,1,5–8 osteoporosis1,5–7,9 and cardiovascular disease.1,5,7–9
Hormone replacement therapy (HRT) in women with POI
Studies have shown that women with POI have a higher incidence of ischaemic heart disease including an increased overall mortality risk, and estrogen replacement has been shown in observational studies to lower the risks of cardiovascular disease and its related morbidity and mortality.10–12 Most international guidance documents recommend hormone replacement in women with POI until the average age of the menopause. 13 However, there is a lack of data from randomised controlled trials regarding the optimal regimen for use in this context, and more research is required to further assess this and guide clinical practice.11,12 A UK national POI registry is currently underway (www.poiregistry.net), which will allow assessment of clinical practice at a national level and will help guide clinical practice in this area until further data from randomised trials become available.
Estrogen is commonly given as HRT or synthetic ethinyl oestradiol in the form of the combined oral contraceptive pill (COCP). There is limited evidence comparing these regimens and subsequently there remains considerable variation in practices amongst clinicians. A recently completed randomised controlled trial assessed the effects of active treatment with HRT or ethinyl oestradiol within the COCP in women with POI. The study outcomes included changes in bone mineral density, serum markers of bone metabolism, markers for cardiovascular disease, menopausal symptom scores and quality of life. It also assessed these outcomes for patients who chose no hormonal treatment. The results of this trial are awaited and should provide useful guidance to clinicians regarding the effects of these regimens. 5
All routes of estrogen administration can effectively treat menopausal symptoms and provide cardiovascular and bone protection in women with POI. The different routes of administration follow different metabolic pathways and as a result can have different advantages and disadvantages. Two large nested case-controlled studies that reviewed the United Kingdom's General Practice Research Database have shown a lower risk of stroke and venous thrombosis in naturally menopausal women between the ages of 50 and 79 receiving transdermal oestradiol (t-E2) compared to those receiving oral oestradiol. 14 These findings however, cannot be extrapolated to women with POI and further research is needed to assess this in women with POI.
Progestogens in HRT
There is also a lack of evidence on the effect and role of various progestogen preparations used within HRT in women with POI. The ability of synthetic progestogens to co-interact with a number of different steroid receptors, can negatively impact on cardiovascular risk factors, through their effects on lipid profiles, vasomotion 15 and carbohydrate metabolism. 16 The androgenic properties of some of the progestogens may counteract the beneficial effect of estrogens on high density lipoproteins (HDLs),15,17,18 as well as increase insulin resistance and impair glucose tolerance.10,17 Micronized progesterone, in contrast, is thought to reduce the incidence of new onset diabetes when combined with transdermal estrogen, and have a neutral or beneficial effect on blood pressure in postmenopausal women. 19
The Women’s Health Initiative (WHI) study showed an increased risk of cardiovascular disease in women who received combined therapy with conjugated equine estrogens (CEEs 0.625 mg/day) and medroxyprogesterone acetate (MPA 2.5 mg/day), compared with placebo. 20
The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial looked at the effects of estrogen or estrogen/progestin regimens (CEE 0.625 mg daily, alone or in combination with one of the three regimens of progestational agents: MPA at 2.5 mg daily, MPA at 10 mg on days 1–12 and micronized progesterone at 200 mg on days 1–12) on heart disease risk factors in postmenopausal women aged between 45 and 64 years. It showed that unopposed estrogen produced the most beneficial effects, but the high rate of endometrial hyperplasia restricted its use to women without a uterus. For women with a uterus, the cyclic use of micronized progesterone produced the most favourable cardiovascular effects. 21 Furthermore, micronized progesterone in combination with estrogen did not affect blood pressure 19 or insulin levels, both surrogate markers of cardiovascular risk and had the most favourable impact on HDL. 13
More recently, the Kronos Early Estrogen Prevention Study (KEEPS) reported on the cardiovascular effects of HRT taken in the early menopause. In total 728 participants were randomised into three groups. One group received 0.45 mg a day of oral CEE. The second group received 50 µg a day of t-E2, while the third group was given a placebo. Women prescribed active estrogens received 200 mg of micronized progesterone for 12 days each month, and women in the placebo arm were given identical placebo capsules during the same time period. 22 The study showed a neutral impact on cardiovascular risk markers such as coronary calcium scores and intima media thickness. There was no negative impact on blood pressure, lipid and insulin resistance, suggesting that micronized progesterone given with t-E2 or with CEE did not negate the beneficial effects of estrogen in this cohort. 23
In summary, the evidence suggests that body identical progesterone – micronized progesterone – appears to have a better safety profile when compared to its synthetic counterparts and may result in a different risk profile. Studies in women beyond the natural age of the menopause have suggested that androgenic progestogens appear to partly reverse the beneficial arterial effects of estrogens, while such effects were noted to be lower with micronized progesterone. These reports have demonstrated a neutral effect on vasculature with micronized progesterone and therefore, a lower risk of venous thromboembolic and cardiovascular disease compared with synthetic progestogens.24–26
However, little research has been carried out to assess the effect of the type of progesterone used on various health parameters in women with POI. Langrish et al. 27 reported an open-label, randomised, controlled crossover trial that compared physiological hormone replacement (t-E2 and vaginal progesterone) with oral ethinyl oestradiol and norethisterone therapy (standard group) in women with POI. The study included 34 women although only 18 completed the study. Women received the allocated treatment for 12 months, and after the first 12-month period, the participants received the alternative treatment following a two-month washout period, for a further 12 months. Both regimens were shown to provide similar symptom relief, however, physiological sex steroid replacement caused lower mean systolic and diastolic blood pressures, reduced plasma angiotensin II and serum creatinine concentrations throughout the 12-month treatment period. No differences in arterial stiffness or plasma aldosterone concentrations were noted between the two groups. The authors concluded that physiological sex steroid replacement in women with POI results in lower blood pressure, better renal function and less activation of the renin-angiotensin system. The study sample size however, was small and the study assessed two variables (t-E2 and progesterone in the intervention arm, and ethinyl oestradiol and norethisterone in the control arm). More research is, therefore, needed to further evaluate these findings.
Our study aims to assess the effect of micronized progesterone and MPA, both used in combination with t-E2 on the cardiovascular system, lipid profile and coagulation cascade of women with POI.
Trial design
Randomised, controlled, open label, two-arm trial, comparing the effects of micronized progesterone, Utrogestan®, to MPA, both used in combination with t-E2 patches (Evorel®) on the cardiovascular system and coagulation cascade of women diagnosed with POI.
Objectives
Primary
To assess the effect of micronized progesterone and MPA on vascular elasticity assessed by examining changes in the pulse wave form.
Secondary
To assess the effect of micronized progesterone and MPA on: pulse wave velocity; lipid profiles; the coagulation cascade; and women’s satisfaction and the side-effect profile with their HRT regimen.
Study outline
Inclusion and exclusion criteria for participation in the trial.

The participants will be randomised to one of the two treatment arms using a web-based computer randomisation software, Graph Pad, where they will be prescribed 50 mcg/day of oestradiol (Evorel 50 patch 2/week) with either Utrogestan 200 mg/day for 12/28 days (group A) or Provera 10 mg/day for 12/28 days (group B).
Flow chart of patients through the study. a
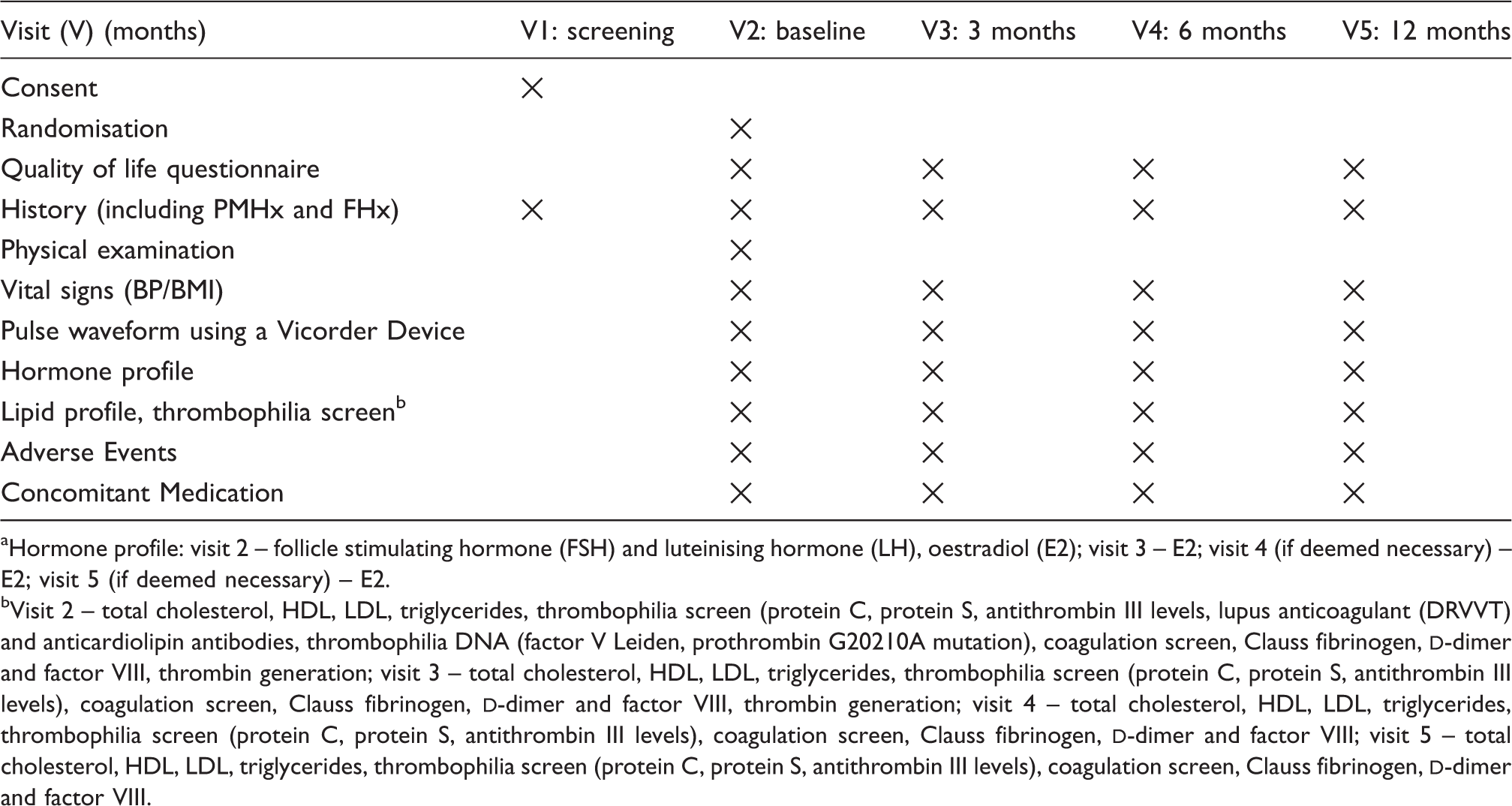
Hormone profile: visit 2 – follicle stimulating hormone (FSH) and luteinising hormone (LH), oestradiol (E2); visit 3 – E2; visit 4 (if deemed necessary) – E2; visit 5 (if deemed necessary) – E2.
Visit 2 – total cholesterol, HDL, LDL, triglycerides, thrombophilia screen (protein C, protein S, antithrombin III levels, lupus anticoagulant (DRVVT) and anticardiolipin antibodies, thrombophilia DNA (factor V Leiden, prothrombin G20210A mutation), coagulation screen, Clauss fibrinogen,
The effect of the two regimens on the cardiovascular health of this cohort of women will be assessed by performing their pulse wave form using the Vicorder Device manufactured by Skidmore Medical Limited, which has been calibrated to investigate vascular disorders.
Lipid metabolism will be assessed by analysing the total cholesterol, HDL, low density lipoprotein (LDL) and triglyceride levels at the stated intervals.
The effect on the coagulation cascade will be assessed by assessing the following parameters: thrombophilia screen (protein C, protein S, antithrombin III levels, lupus anticoagulant (DRVVT) and anticardiolipin antibodies), thrombophilia DNA (factor V Leiden, prothrombin G20210A mutation), coagulation screen, Clauss fibrinogen,
The serum samples will be analysed on an ongoing basis except for the thrombin generation samples which will be stored at −40℃ and analysed in batches.
The trial has received ethical approval from the West London and GTAC Ethics Committee. The trial will be conducted in compliance with the principles of the Declaration of Helsinki (1996), the principles of Good Clinical Practice and in accordance with all applicable regulatory requirements including but not limited to the Research Governance Framework and the Medicines for Human Use (Clinical Trial) Regulations 2004, as amended in 2006 and any subsequent amendments.
Sample size and statistical analysis
We aim to recruit 90 women in total to allow for a 10% drop out and loss to follow up. The sample size was calculated using the Altman nomogram 28 and based on changes in the Augmentation Index (AI) in response to exposure to the two different progesterones assessed in the study. Baseline data were obtained from reference population pulse wave analysis and AI data as reported by McEniery et al. 29 Based on the reported findings, we considered a change of 8% with standard deviation of 12 to be a clinically significant difference to detect. Using the Altman nomogram, this would give a standardised difference of 0.80. A sample of 80 women in two groups would detect a standardised difference of 0.80 with 80% power at the 5% level of significance.
Statistical analysis will be by intention to treat. Variables that are normally distributed will be presented as means and standard deviations and analysed using the independent and paired t test while data not normally distributed will be presented as medians and range and analysed using the Mann Whitney U test. The chi square or Fisher’s exact will be used as appropriate for independent nominal data. Confidence intervals will be used where appropriate and statistical significance will be defined as a p value of less than 0.05. Regression analysis will be carried out to adjust for the effect of women’s age on the study outcomes.
Discussion
The objective of this trial is to assess the effect of micronized progesterone and MPA, both used in combination with t-E2 on the cardiovascular system, lipid profile and coagulation cascade in women with POI. While the benefits of hormone replacement in women with POI have been shown in a number of observational studies, there is lack of evidence from randomised controlled trials to guide clinical practice regarding the optimal regimen of hormone replacement in this group of women, be it regarding the dose or route of oestradiol administration or the type of progesterone replacement and there remains large variation in the regimens used in clinical practice. 30
Large variations exist in the age limits used to define premature menopause with many studies using an age limit of 40 years. Women who become menopausal between the age of 40 and up to the age of 45 are exposed to the effects of estrogen deficiency for a significant number of years compared to those who become menopausal at the age of 52 or beyond. In this study, we, therefore, used an upper age limit of 45 years in our inclusion criteria and we plan to carry out statistical regression analysis on completion of the study to adjust for the effect of age on the study outcomes. The age limit of 45 years was used based on the recommended age cut-off used in the British Menopause Society Consensus Statement on the management of premature menopause of 2007, and as used in previous studies.1,5
We chose the transdermal route of oestradiol administration as this has been noted in laboratory studies to have no adverse effect on the coagulation cascade, and has also been shown in large observational cohort studies in naturally menopausal women to be associated with a lower risk of venous and arterial disease compared with oral oestradiol administration. Studies in naturally menopausal women have suggested a lower risk cardiovascular disease, venous thrombosis as well as a lower risk of breast cancer with micronized progesterone compared to that with synthetic progestogens. 31 The overarching aim of this study is to address the effects these regimens may have on the cardiovascular system, lipid profile and coagulation cascade in women with POI as this could have significant implications for the future cardiovascular health of this young group of women who require long-term HRT.
Footnotes
Ethical approval
London and GTAC Ethics Committee; EudraCT Number: 2012-004511-30; REC Number: 12/LO/1957.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.