
Abstract
It has been argued that schizophrenic delusions are “behaviourally inert.” This is evidence for the phenomenon of “double bookkeeping,” according to which people are not consistent in their commitment to the content of their delusions. The traditional explanation for the phenomenon is that people do not genuinely believe the content of their delusions. In the article, we resist the traditional explanation and offer an alternative hypothesis: people with delusions often fail to acquire or to maintain the motivation to act on their delusional beliefs. This may be due to avolition, to emotional disturbances, or to the fact that, given the peculiar content of some delusions, the surrounding environment does not support the agent’s motivation to act.
People with delusions may believe that they are dead (Cotard delusion), that a celebrity is secretly in love with them (erotomania), or that some of their thoughts are being inserted into their heads by an ill-meaning third person (thought-insertion). According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV 2000, p. 765), delusions are false beliefs that resist counterevidence. However, there is a lively debate on whether delusions should be characterized as beliefs at all (Bayne & Pacherie, 2005; Bortolotti, 2009). As Campbell elegantly puts the problem,
You might propose that what we have here is not, strictly speaking, belief at all, but “empty speech” masquerading as belief. The trouble with this diagnosis is that these are perfectly sincere assertions made by people who seem to understand what they are saying, who may indeed act on the basis of what they are saying. (Campbell, 2001, p. 91)
The thesis that delusions are not beliefs is often justified on the basis of the view that beliefs have core features which delusions do not share. Possibly the most powerful of these arguments is that delusions are not beliefs because people with delusions fail to manifest commitment to the content of their delusions. This may be either because they fail to act on their delusions when the opportunity presents itself (inaction), or because they act in a way that is not consistent with believing the content of the delusion (attitude–behaviour inconsistency). The assumption underlying this antidoxastic argument is that typically people manifest commitment to the content of their beliefs, and their beliefs guide action in the relevant circumstances.
Bleuler (1950) first introduced the notion of “double awareness” in schizophrenia: people with schizophrenic delusions may fail to act in accordance with their delusions. Sass (1994, 2001, 2004) and Gallagher (2009) reelaborate Bleuler’s idea, and call the phenomenon “double bookkeeping.” They suggest that people with delusions are at least implicitly aware that their delusions are not about reality: “A patient can view doctors and nurses as poisoners (in delusional reality) but happily eats the food they give her (in everyday reality)” (Gallagher, 2009, p. 260). The appeal to double bookkeeping in schizophrenia is suggestive, but it should be accompanied by a review of the available evidence of people’s manifest commitment to the content of their delusions. There are some striking examples of delusions guiding action, both from the psychological and psychiatric literature and from clinical vignettes. Here are some of these examples.
A person with delusions of passivity wears a cap because he wants to prevent his neighbour from inserting thoughts into his head.
People with Cotard delusion stop bathing and eating (Weinstein, 1996).
People with persecutory delusions avoid specific situations or certain individuals because they perceive them as threatening (Freeman, Garety, & Kuipers, 2001).
Self-inflicted eye injury and self-mutilation are common in people who believe that they deserve punishment due to their delusions of guilt (Buchanan & Wessely, 1998).
Acts of violence are motivated by delusions, especially when people react to misperceived threats (Bourget & Whitehurst, 2004; Förstl, Almeida, Owen, Burns, & Howard, 1991; Junginger, Parks-Levy, & McGuire, 1998).
On the basis of these examples, we should refrain from considering double bookkeeping as a general feature of delusions and say instead that in some circumstances people with delusions fail to act in a way that signals commitment to the content of their delusions. A question remains: Why isn’t the commitment to the content of a delusion always manifested in behaviour? The traditional explanation for the phenomenon is that people do not genuinely believe the content of their delusions.
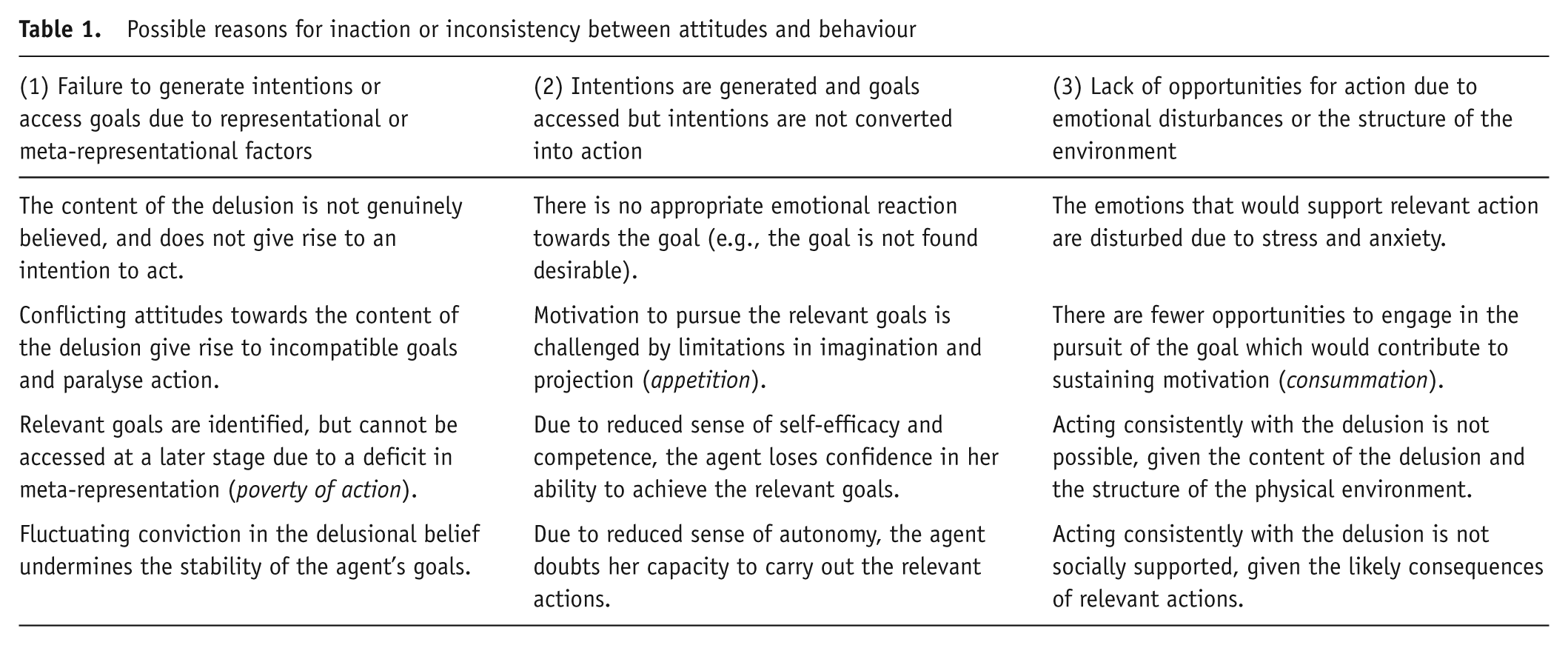
We want to resist the traditional explanation and suggest that there are a number of plausible explanations (see Table 1). In this article we shall not pursue the explanations in the first column. (For some attempt at defusing merely cognitive explanations, see Bortolotti (2010)). Instead, we shall explore some of the explanations in the second and third columns. We shall argue that people with delusions may fail to acquire or to sustain the motivation to act on their delusions. In the next section, we shall explore the plausibility of the view that lack of motivation is due to volitional or emotional deficits or disturbances. In the following section, we shall discuss the possibility that motivation is undermined when the content of the delusion is such that the person may not have the opportunity to act on it.
Possible reasons for inaction or inconsistency between attitudes and behaviour
Volitional and Emotional Factors Undermining Motivation
The hypothesis we wish to consider here is that people with schizophrenic delusions fail to manifest their commitment to the content of their delusions because of a breakdown of motivation. In cognitive psychology it is believed that one’s motivation to act is affected by (a) the desirability of the goal; (b) the perceived likelihood to achieve the goal; and (c) the support of the surrounding environmental and social context (see Allport, 1937; Armitage & Christian, 2004; Austin & Vancouver, 1996; Ford, 1992; Kuhl & Beckman, 1985).
The desirability of a goal is strictly related to the beliefs, desires and aspirations of the agent, and social pressure. The perceived likelihood to achieve the goal is affected by the agent’s sense of behavioural control, that is, whether the agent represents the goal as something that can be achieved given its intrinsic features; and the agent’s sense of self-efficacy, that is, whether the agent represents herself as able to perform successfully the actions leading to the achievement of the goal. Contextual factors play a crucial role too, and this idea will become central to our considerations in the next section: the surrounding physical and social environment can be either responsive or unresponsive to the agent’s newly formed intentions to act.
When an agent fails to act on her beliefs, or acts in a way that appears to be inconsistent with the beliefs she reports to have, a number of explanations for such failure are plausible, and some of them involve the failure to acquire or sustain the motivation to act in accordance with her beliefs. For instance, the agent may never acquire the necessary motivation to act because she believes that she has no genuine control over her own behaviour. Thus, her intention does not translate into action. Alternatively, the agent may fail to sustain her own motivation to act, if she has attitudes that conflict with her finding the goal desirable. A third hypothesis is that the social and contextual factors lead the agent to see herself as incompetent in performing the relevant action (Ryan & Deci, 2000). This is the case when the agent lacks a sense of autonomy (intended as the belief that the action is actually caused by her) and a sense of relatedness (intended as support from her close personal relationships). It may not be a coincidence that some of the conditions responsible for lack of motivation are also among the causal factors contributing to psychopathology (Ryan & Deci, 2000, p. 76), such as the impression that there is excessive external control over one’s thoughts and actions, which compromises the agent’s sense of autonomy, and the absence of supportive personal relationships, which negatively affects the sense of relatedness.
Foussias and Remington (2008) suggest that people with schizophrenia are not necessarily unable to represent their goals as desirable. Rather, they find it harder than participants in control conditions to act in such a way as to enjoy the pleasant emotions associated with the pursuit and achievement of their goals and to channel them into action. Studies presented and reviewed by Gard, Kring, Germans Gard, Horan, and Green (2007) and Kring and Germans (2004) seem to confirm this hypothesis. If people with schizophrenia are asked to predict how much pleasure they will derive from a potentially pleasurable experience, they predict that they will derive less pleasure from it than participants in control conditions. Similarly, when asked to report after the experience how pleasant the experience was, people with schizophrenia report that they felt less pleasure than participants in control conditions. The hypothesis is that there are several emotional components to the enjoyment of pleasant experiences. The anticipatory component concerns the pleasure derived from the imagination or the expectation of a rewarding experience. The consummatory component concerns the pleasure derived from the actual pursuit of and engagement in the desired activity. Finally, there is also the issue of whether pleasurable experiences are successfully encoded and can be recalled as pleasurable at a later time. Judging from self-reports, people with schizophrenia seem to experience less pleasure than participants in control conditions, but this may not be the case. Neurobiological data suggest that people with schizophrenia are able to enjoy pleasurable actions as much as participants in control conditions. A possible explanation for their self-reports is that differences between people with schizophrenia and participants in control conditions emerge at the stage of anticipation and encoding, and do not affect the actual experience.
What are the implications of the avolition literature for double bookkeeping? Avolition is often characterized as a form of weakness of will and distinguished from absence of hedonic reward. But one hypothesis is that people are less motivated to act in a way that is consistent with the content of their delusions because they find it harder to imagine the future outcomes of their actions and to anticipate the pleasure they may derive from the achievement of their goals. This hypothesis predicts that failures of imagination and anticipation would affect one’s motivation to act in general, and not just the motivation to act in accordance with delusional beliefs.
Another reason why people might fail to commit behaviourally to their delusions may be found in emotional disturbances. These phenomena may contribute to a failure of motivation which results in an agent ceasing to pursue her initial goal. Bleuler (1950, p. 70), who identifies schizophrenia with a “breakdown of the emotions,” notices that people with schizophrenia often appear indifferent in the sense that they do not express the emotions they feel. Such indifference would now be considered as a negative symptom of schizophrenia.
In cognitive neuro-psychological approaches to schizophrenia the relationship between emotions and psychotic symptoms is an object of controversy. The accepted view is that emotional disturbances (e.g., emotional excesses and deficits or lack of regulation) are not a direct cause of psychotic symptoms, but contribute to their maintenance and severity. For instance, in people with schizophrenia, negative self-evaluation is correlated with more severe positive symptoms (Barrowclough et al., 2003). In people with delusions, distress is correlated with the severity of the delusions (Lysaker, Lancaster, Nees, & Davis, 2003) and high levels of anger are often recorded (Cullari, 1994; Siris, 1995). More recently, Freeman and Garety (2003) have challenged the accepted view and suggested that emotions directly cause delusions. This is because anxiety contributes to delusional conviction, in a way that is quite independent of reasoning. “It is proposed that delusional explanations are a direct reflection of pre-existing beliefs about the self, world and others, and that these beliefs are intimately linked to emotion” (Freeman & Garety, 2003, p. 931). Broome et al. (2005), who investigated the developmental and epidemiological factors influencing prodromal symptoms (i.e., the symptoms immediately prior to the onset of a disease), observed how people at high risk of psychosis experience distress, decreased motivation, and poor socialization from an early age. Those in the “high-risk” sample who make the transition to “psychotic” are often depressed and anxious before suffering from positive symptoms.
Evidence that seems to support a positive correlation between emotion and motivation emerges from the observation that, when there are strong emotional reactions relevant to a person’s delusions, such as anger, the person is more likely to act on her delusions. If the emotions typically associated with the content of the delusions are not manifested, as with emotional disturbances, then the motivation is undermined as a result.
Lack of Commitment and the Responsiveness of the World
Here we shall consider a further explanation for people failing to express behavioural commitment to their beliefs. Agents may find themselves in a physically or socially structured environment in which there are serious obstacles to exhibiting the type of behaviour that would be consistent with their beliefs. A typical case is that of a person failing to act on her delusion because, given the contents of the delusion and the constraints imposed by the world in which she lives, either there is no appropriate action that she can take, or the only appropriate action would have unpleasant or dangerous consequences.
A woman believes that the world is ending and she is the only one who can save the world by deciphering signs that God sends her in her dreams. Although the woman’s verbal behaviour may be a testimony of her commitment to the delusion, it is difficult to identify desirable goals that she could achieve if she decided to act on her delusions. The woman is well aware that other people are unlikely to believe her, so she may not even warn others about the end of the world.
When a man with Capgras delusion says that he can’t go to the police to report the disappearance of his wife because the police wouldn’t believe that aliens abducted her and replaced her with an impostor, it is obvious to him as well as to others that his social environment would not be supportive of his action. Action may be inhibited as a result.
In both the cases above, people fail to act on their delusions because they retain an awareness of how odd their beliefs and behaviour may appear to others. In more radical cases, the delusion conflicts with our current understanding of the physical world. One case discussed by Campbell (2009) and by Broome, Bortolotti, and Mameli (2010) is that of a man who believed that a lizard was inside his body due to the scaly appearance of his skin. As a result, he tried to remove the lizard with a knife, harming himself as a result (Browning & Jones, 1988). Arguably it is not unreasonable to try and remove a source of danger from oneself if one believes that the danger is real. If the man believed that the doctor could not help him, and that there were no professional lizard killers around, then the prospect of removing the lizard himself with a knife may have seemed to him the only rational thing to do. By comparison, one can think about the case of a person stranded on Mount Everest who rationally decides to remove a gangrenous or frostbitten arm to save her life. The rational agent balances perceived risks in order to maximize her chances of survival: in this case, the relevant risks are (a) the risk incurred in cutting oneself with a knife and (b) the risk of being eaten from the inside by a poisonous lizard (compare the latter with the risk of gangrene leading to certain death).
A similar risk–benefit analysis can result in inaction rather than action for the person with delusions. If the outcome of the risk–benefit analysis had been different, then the person afflicted by the delusion of lizard infestation would have refrained from acting. He could have concluded that it was less dangerous to have his body colonized by reptiles than to attempt to remove the reptiles with a knife. This would have led the man to do nothing about the infestation, or maybe search for other ways to stop it.
The point we are attempting to make is that, in the case of some delusional beliefs that are held with absolute conviction, the very strangeness of the belief seems to inhibit action altogether, or to lead to undesirable or dangerous actions for which motivation is likely to falter. Examples encountered in clinical practice by one of us (MB) tend to be beliefs that conflict with the basic laws of physics and biology:
a man who believed that he had a full-scale nuclear reactor inside himself;
a man who felt that his body was occupied by a superhero team devoted to battling for the good of Crystal Palace Football Club;
a woman who believed that she was endlessly pregnant and giving birth to a series of Messiahs.
The people in the second and third cases felt privileged about their conditions and, other than talking about their beliefs, they felt no need to act on them. They, as individuals, were “containers” of other entities and they thought that they were themselves not under any threat. The person in the first case did get concerned about the presence of the nuclear reactor inside himself. However, due to the sheer impossibility and paradoxical nature of his claims, he found it very difficult to talk about his belief to those around him. Nonetheless, the belief had a strong negative impact on his life.
In the description of a nuclear reactor residing inside one’s own body, language gives way because soon a point is reached where the chain of reasoning and justification can go no further (see Bortolotti & Broome, 2008). So, the person in the first case often said “That’s just the way it is” or “There is no way I can make you understand,” and no further explanation was given as to how he could house a nuclear reactor inside himself. He was not attempting to mislead: He was genuinely trying to explain his predicament to those whom he came into contact. However, given the strangeness of his belief and experiences, there was no clear or obvious way for himself or others to act in response to his assertions. This caused frustration and impotence in the sufferer, and bafflement and perplexity in the people surrounding him. This is sadly a common occurrence in people with delusions: As a result of these unsuccessful attempts at communication, they may just stop trying to engage others in their beliefs.
For someone with very odd delusions, and in particular for someone who holds beliefs which cannot be true, given the physical laws that make up the universe, it has been suggested that a private reality is occupied by the person with the delusion (Gallagher, 2009) or that her thoughts spin “frictionlessly in the void” (McDowell, 1994, p. 18). The person with such odd beliefs has become disconnected from the rational constraints of the world in parts of her thinking. However, this disconnection is two-sided: As well as freeing thought from the world, it frees the world from the thought. This idea is discussed in Campbell with respect to Cotard’s syndrome: “The problem is how any experience at all, let alone an experience of marble tables, could be relevant to the verification of the proposition, ‘the world is ending’” (Campbell, 2001, p. 95). If the world is such that people with bizarre delusions cannot think of experiences that support their reports, then such delusions may also fail to give rise to attainable or desirable goals, or fail to give rise to any goals whatsoever.
Conclusions
The phenomenon of double bookkeeping in delusions is of great interest: Why do people seem to lack commitment to the content of their delusional beliefs? The standard approach is to reject the view that delusions are beliefs and emphasize the disanalogy between delusions and beliefs: The latter are manifested behaviourally, whereas the former are behaviourally inert.
In this article, we suggested that there is an alternative explanation that hasn’t been sufficiently explored in the philosophical literature: People may fail to commit behaviourally to the content of their delusions when they fail to acquire or sustain the motivation to act on their delusions. In attempting to make this alternative explanation plausible, we stressed the analogy between delusions and beliefs: Both may fail to be acted upon when certain conditions obtain, such as the relevant goals appearing either unattainable or undesirable to the agent.
We explored different routes to undermining motivation in psychopathology and briefly examined the role of avolition and emotional disturbances in the explanation of double bookkeeping. Then, we considered the contribution of the surrounding environment to the agent’s appreciation of the desirability or attainability of the goals that are relevant to her delusions.